Article Text

Abstract
Objectives We sought to evaluate the physiology of non-culprit lesions by using vessel fractional flow reserve (vFFR) among patients with ST elevation myocardial infarction (STEMI) and multivessel disease (MVD).
Methods From January 2017 to December 2019, 354 patients with STEMI in the Taipei Veterans General Hospital Acute Myocardial Infarction Registry were screened. Patients who underwent successful primary percutaneous coronary intervention (PCI) for culprit lesions, with at least one non-culprit lesion with stenosis of ≥50%, were eligible. vFFR was computed retrospectively.
Results A total of 156 patients with 217 non-culprit lesions were eligible for this study. Aortic root pressure and two good angiograms were available for 139 non-culprit lesions for vFFR analysis. Based on the vFFR analysis, 59 non-culprit lesions (43.2%) had a vFFR value >0.80, and PCI was deferred in 45 lesions (76.3%). Meanwhile, 80 non-culprit lesions (56.8%) had a vFFR value ≤0.80; however, PCI was only performed in 31 lesions (38.7%) (p=0.142). The incidence of vessel-oriented composite endpoint was numerically higher in non-culprit lesions with vFFR ≤0.80 than those with vFFR >0.80 (6.3% vs 1.7%, HR: 3.59, 95% CI: 0.42 to 30.8, p=0.243).
Conclusion Functional incomplete revascularisation is common among patients with STEMI and MVD. The adoption of vFFR to assess non-culprit lesions may reclassify the coronary revascularisation strategy that is usually guided by angiography only in this acute setting.
- acute coronary syndrome
- coronary artery disease
- coronary stenosis
Data availability statement
No data are available.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known about this subject?
Fractional flow reserve (FFR)-guided percutaneous coronary intervention (PCI) of non-culprit lesions in patients with ST elevation myocardial infarction (STEMI) had significantly lower adverse event rates compared to culprit-lesion-only PCI. Nevertheless, FFR is rarely used in clinical practice during primary PCI for patients with STEMI and multivessel disease (MVD).
What does this study add?
We demonstrated that functional incomplete revascularisation is common in angiography-guided PCI in patients with STEMI and MVD. The vessel FFR (vFFR) can be used to assess non-culprit lesions based on angiograms of the index procedure in a post hoc manner. vFFR of non-culprit lesions was highly correlated in the acute and staged procedures.
How might this impact on clinical practice?
vFFR may increase the adoption rate of physiology assessment for non-culprit lesions in patients with STEMI and MVD. The use of vFFR may reduce the number of unnecessary downstream invasive coronary angiography procedures and may lead to an increase in functional complete revascularisation.
Introduction
Coronary angiography and primary percutaneous coronary intervention (PCI) are the current standards of care for managing ST elevation myocardial infarction (STEMI). The COMPLETE trial indicated that in patients with STEMI and multivessel disease (MVD), complete revascularisation for non-culprit lesions with stenosis >70% was superior to culprit-lesion-only PCI.1 Recently, DANAMI-3–PRIMULTI and COMPARE-ACUTE, two large randomised clinical studies, have demonstrated that fractional flow reserve (FFR)-guided PCI of non-culprit lesions in patients with STEMI had significantly lower adverse event rates compared with culprit-lesion-only PCI.2 3 Nevertheless, FFR is rarely used in clinical practice in primary PCI for patients with STEMI and MVD. The use of FFR is limited by the necessity of intravenous or intracoronary adenosine infusion and additional equipment. Therefore, the decision of revascularisation for non-culprit lesions in patients with STEMI is typically based on coronary angiograms of the index procedure, or a staged procedure is needed at the operator’s discretion. Based on the literature, further study is needed to assess the implications of coronary physiology in this setting.
Currently, coronary physiology can be assessed without medications or a pressure wire. Vessel FFR (vFFR) is a novel physiological index that is calculated based on computational fluid dynamics and a three-dimensional reconstruction model. The Fast Assessment of STenosis severity (FAST) Study showed a strong linear correlation between FFR and vFFR, with good reproducibility and high diagnostic accuracy.4 This angiography-derived functional assessment can be performed ad hoc or retrospectively when treating patients with STEMI and MVD. In this context, we sought to evaluate vFFR values of non-culprit lesions and investigate the concordance rate of revascularisation strategy that is suggested by vFFR and the actual treatment performed in patients with STEMI and MVD.
Methods
Study design and participants
The present study was an observational, retrospective, single-centre study. From January 2017 to December 2019, patients presenting with STEMI at Taipei Veterans General Hospital were screened. STEMI was defined according to the Third Universal Myocardial Infarction definition.5 Patients who underwent successful primary PCI for culprit lesions, with at least one non-culprit lesion with stenosis of ≥50% with a reference vessel diameter ≥2.0 mm (by visual estimation) on coronary angiography, were eligible. Patients who presented with cardiac arrest, profound cardiogenic shock or ostial or left main non-culprit lesions were excluded. The decision for treatment of non-culprit lesions was based on coronary angiograms and clinical factors. PCIs for non-culprit lesions were performed at the time of primary PCI or in a staged procedure. A staged procedure was defined as a planned intervention, and the procedure should be performed electively within 16 weeks after the primary PCI.6 The study was approved by the Taipei Veterans General Hospital’s research ethics committee and was conducted in accordance with the Declaration of Helsinki.
vFFR analysis
The vFFR analysis was performed by independent analysts using CAAS Workstation (V.8.2; Pie Medical Imaging, Maastricht, the Netherlands) and was based on previous reports of image acquisition and processing.4 Briefly, two angiograms with at least a 30° difference in rotation/angulation are required to create a 3D reconstruction of the coronary artery. Coronary angiography was performed using a conventional radiation mode (15 frames per second and 15 pulses per second). The software contour detection was performed semiautomatically, delineating the vessel contour from the ostium to a distal position, with manual correction performed when needed. A 3D quantitative coronary angiography (QCA) and vFFR values were automatically generated.
Clinical endpoints per vessel
The primary endpoint of this study was the vessel-oriented composite endpoint (VOCE) during clinical follow-up, defined as a composite of vessel-related cardiac death, vessel-related myocardial infarction (MI) and target vessel revascularisation (TVR). Cardiac death was defined as death resulting from cardiovascular causes (eg, acute MI, cardiac death or unwitnessed death or heart failure).7 MI was defined according to the Third Universal Myocardial Infarction definition.5 TVR was defined as any repeat percutaneous intervention or surgical bypass of any segment of the target vessel including the target lesion.7 VOCE was analysed in a hierarchical manner.
Clinical events were counted per vessel and were classified as vessel related or not vessel related. If the patient was classified as cardiac death without a clear correlation to a specific vessel (eg, heart failure or unwitnessed death) at follow-up, the worst scenario was considered, and the death was adjudicated as a vessel-related cardiac death. Whenever an MI or revascularisation occurred, angiograms at event and medical records were reviewed by investigators for clinical event adjudication.
Statistical methods
Categorical variables are presented as percentages and numbers. Continuous variables are presented as the mean±SD. Pearson’s correlation coefficient and Cohen’s kappa coefficient were used to evaluate the correlation and agreement of vFFR values at two different times (primary PCI vs staged PCI). Survival curves were constructed using Kaplan-Meier estimates and the log-rank test to compare between-group differences. An HR was reported with 95% CIs based on the Cox regression model. A two-sided p value of <0.05 was considered statistically significant. Data were analysed using SPSS software (V.25).
Results
A total of 354 patients who presented with STEMI were screened, and 156 patients with 217 non-culprit lesions were eligible for this study. Among these patients, aortic root pressure and two good angiograms were available for vFFR analysis of 139 non-culprit lesions. The retrospective analysability was 64%, and the reasons of being non-analysable were mainly due to no appropriate two projections to perform vFFR analysis for non-culprit lesions. A representative case of vFFR analysis is shown in figure 1. The baseline characteristics of the eligible patients are shown in table 1. The mean age was 65.8±14.5 years, 86.5% were men and 34.6% had diabetes. Most patients (84.6%) only underwent PCI for culprit lesions in the index procedure, whereas 14.7% also received PCI for non-culprit lesions during the index procedure. Drug-eluting stents were deployed in 76.3% of patients.

A representative case of vFFR analysis. vFFR=vessel fraction flow reserve.
Baseline characteristics of patients
The locations of non-culprit lesions and 3D QCA data are provided in table 2. The mean minimal lumen diameter, percent diameter stenosis and obstruction length were 1.44±0.51 mm, 44.5%±12.5%, and 19.2±12.5 mm, respectively. The mean vFFR values of non-culprit lesions included the following: left anterior descending artery, 0.72±0.13; left circumflex artery, 0.74±0.17; and right coronary artery, 0.81±0.19, respectively (table 3). Based on the vFFR analysis, 59 non-culprit lesions (43.2%) had a vFFR value >0.80, and PCI was deferred in 45 lesions (76.3%). Meanwhile, 80 non-culprit lesions (56.8%) had a vFFR value ≤0.80; however, PCI was only performed in 31 lesions (38.7%) (p=0.142) (table 4). The concordance rate of revascularisation strategy recommended by the post hoc vFFR was only 54.4% (76/139) with the actual treatment, which was mainly guided by angiography. During a mean follow-up of 672±412 days, the incidence of VOCE was numerically higher in non-culprit lesions with a vFFR value ≤0.80 than those >0.80 (6.3% vs 1.7%, HR: 3.59, 95% CI: 0.42 to 30.8, p=0.243) (figure 2A). We further stratified non-culprit lesions into four groups based on PCI deferred or performed. In lesions with a vFFR value ≤0.80, the incidence of VOCE was similar between the deferred and performed groups (figure 2B).
Actual management of non-culprit lesions
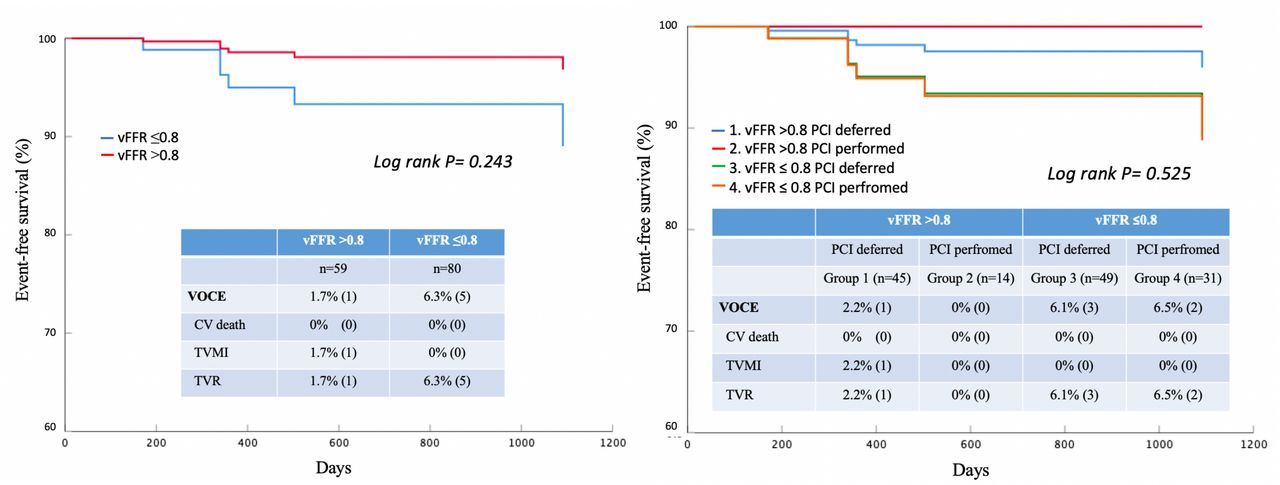
Event-free survival curves. CV=cardiovascular, vFFR=vessel fraction flow reserve, VOCE=vessel-oriented composite endpoint, TVMI=target vessel myocardial infarction and TVR=target vessel revascularisation.
Baseline characteristics of non-culprit lesions studied
Vessel fraction flow reserve (vFFR) values of non-culprit lesions
Among the 32 non-culprit lesions that underwent a staged PCI, vFFR analysis was feasible in 22 lesions. The mean duration between index and staged PCI was 46±36 days. The correlation of vFFR of the same non-culprit lesions between primary and staged PCI was significant (r=0.822, p<0.001). Similarly, agreement in functional significance was also significant (Cohen’s kappa=0.861). The Bland-Altman plots that displayed a mean difference between index and staged vFFR were 0.03 (95% CI: −0.15 to 0.21) (figure 3).

{kind=link}
{kind=link}
{kind=link}
Correlation between vFFR in primary and staged PCI. PCI=percutaneous coronary intervention and vFFR=vessel fraction flow reserve.
Discussion
In the present study, we investigated the coronary physiology of non-culprit lesions using vFFR analysis in patients with STEMI and MVD. The main findings of the present study are as follows. In the setting of angiography-guided PCI, more than half of non-culprit lesions with vFFR ≤0.8 remained with functional incomplete revascularisation. Also, the vFFR of non-culprit lesions measured acutely was highly correlated with vFFR measured subsequently after STEMI. Given that vFFR analysis can be performed acutely or retrospectively, vFFR can be used to assess the coronary physiology of non-culprit lesions after primary PCI.
Previous studies have shown that patients with functional incomplete revascularisation had a significantly higher rate of major adverse cardiac events than those with functional complete revascularisation.8 However, the utilisation rate of FFR for assessing intermediate coronary lesions is only about 15%.9 10 Although randomised trials have demonstrated the benefit of FFR-guided complete revascularisation in patients with STEMI and MVD, it is not realistic to perform FFR measurement for non-culprit lesions acutely in primary PCI. In addition, the accuracy of wire-based physiological indices may be slightly affected in the setting of acute MI due to disturbed microvascular function.11 12 In this setting, angiography-guided decision-making for the treatment of non-culprit lesions was commonly adopted rather than physiology-guided PCI. In the COMPLETE trial, non-culprit lesions with more than 70% stenosis by visual assessment were treated with PCI directly, while those with a stenosis between 50% and 70% were assessed with pressure wire. Physiology-guided revascularisation was used in only 1.4% of the lesions.1 Alternatively, the mismatch between anatomical and functional assessment of coronary lesions has been extensively reported and showed a significant reclassification in indication for revascularisation.13 14 In our study, a quarter of non-culprit lesions with vFFR values >0.8 underwent PCI, whereas more than half of the lesions with vFFR ≤0.8 were left untreated. Although there are a multitude of reasons for the undertreatment of functionally significant lesions in our cohort, there is a need to implement functional assessment in the management of non-culprit lesions in a more practical way rather than using FFR in primary PCI. In our study, vFFR of non-culprit lesions was highly correlated in the acute and staged procedures. vFFR may be used to assess non-culprit lesions based on angiograms of the index procedure in an ad hoc or post hoc manner. The same type of analysis using quantitative flow ratio (QFR) for non-culprit lesion of STEMI has been reported.15 Acute QFR of non-culprit lesions had a good diagnostic performance with both staged QFR and staged FFR. Therefore, the use of angiography-derived FFR, such as vFFR and QFR, may reduce the number of unnecessary downstream invasive coronary angiography procedures and may also lead to an increase in functional complete revascularisation in patients with STEMI and MVD.
QFR and vFFR are both a type of angiography-derived FFR. They are computed using different fluid dynamics models.16 A Bayesian meta-analysis has shown that the diagnostic performance of angiography-derived FFR is good with high sensitivity and specificity with pressure wire-based FFR as reference.17 There are no differences in accuracy for detecting functionally significant lesions between vFFR, QFR and FFRangio. At variance with FFR or instantaneous wave-free ratio (iFR), the prognostic value of angiography-derived FFR is under investigation.18–20 In our study, lesions with vFFR ≤0.8 had a numerically higher rate of VOCE than lesions with vFFR >0.8. However, the event rate was relatively low in our study to demonstrate meaningful differences, and potential confounding variables may affect our findings. A large-scale, prospective study with adequate power is demanded to evaluate whether the implementation of vFFR for assessing non-culprit lesions in patients with STEMI and MVD has an influence on clinical outcomes compared with angiography-guided revascularisation.
Limitations
Our study has several limitations. First, this was a retrospective study; therefore, coronary angiograms were obtained based on routine clinical practice. As such, the retrospective analysability of vFFR for non-culprit lesions was limited in our study since interventionists usually focused on the culprit lesions during the primary PCI. Similarly, the reported analysability of QFR was also low in the same setting.15 Further studies with a dedicated imaging acquisition protocol are warranted to evaluate the analysability in this acute setting. Also, our results obtained from a single centre with a limited sample size need to be confirmed in future studies. Additionally, FFR was not performed for non-culprit lesions in our study. Therefore, the correlation between FFR and vFFR in patients with acute coronary syndrome warrants further investigation.
Conclusion
Functional incomplete revascularisation is common in real-world practice in patients with STEMI and MVD. The vFFR might be an alternative physiological index used to assess non-culprit lesions in this acute setting, and the adoption of vFFR may reclassify the coronary revascularisation strategy that is guided by angiography.
Data availability statement
No data are available.
Ethics statements
Ethics approval
The study was approved by the Taipei Veterans General Hospital’s research ethics committee and was conducted in accordance with the Declaration of Helsinki.
Acknowledgments
All authors would like to thank Jan-Jurre Mordang and Jorn Roijen from Pie Medical Imaging for their technical support.
References
Footnotes
Contributors CCC, PHH and SJL contributed to the conception and design of the study. CCC, YHL, MJC, YWL, YLT, RHC, CHW and TML contributed to data collection. CCC, YHL and MJC analysed and interpreted the data. CCC, YHL and MJC drafted the report, which was critically revised for important intellectual content by TML, PHH and SJL. All authors approved the final version of the report.
Funding This study was supported in part by research grants from the Novel Bioengineering and Technological Approaches to Solve Two Major Health Problems in Taiwan programme sponsored by the Taiwan Ministry of Science and Technology Academic Excellence Programme (108–2633-B-009–001) and Taipei Veterans General Hospital (VGH-V100E2-002 and VGHUST103-G7-2-1).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.