Article Text

Abstract
Objective To assess current management practice of heart failure with reduced ejection fraction (HFrEF) in multinational primary care (PC) and determine whether N-terminal-pro-B-type natriuretic peptide (NT-pro-BNP)-guided referral of HFrEF patients from PC to a cardiologist could improve care, defined as adherence to European Society of Cardiology (ESC) guideline-recommended pharmacotherapy.
Methods PRospective Evaluation of natriuretic peptide-based reFERral of patients with chronic HF in PC (PREFER) study enrolled HFrEF patients from PC considered clinically stable and those with NT-pro-BNP ≥600 pg/mL were referred to a cardiologist for optimisation of HF treatment. The primary outcome of adherence to ESC HF guidelines after referral to specialist was assessed at the second visit within 4 weeks of cardiologist’s referral and no later than 6 months after the baseline visit. Based on futility interim analysis, the study was terminated early.
Results In total, 1415 HFrEF patients from 223 PCs from 18 countries in Europe were enrolled. Of these, 1324 (96.9%) were considered clinically stable and 920 (65.0%) had NT-pro-BNP ≥600 pg/mL (mean: 2631 pg/mL). In total, 861 (60.8%) patients fulfilled both criteria and were referred to a cardiologist. Before cardiologist consultation, 10.1% of patients were on ESC guideline-recommended HFrEF medications and 2.7% were on recommended dosages of HFrEF medication (defined as ≥50% of ESC guideline-recommended dose). Postreferral, prescribed HFrEF drugs remained largely unchanged except for an increase in diuretics (+4.6%) and mineralocorticoid receptor antagonists (+7.9%). No significant increase in patients’ adherence to guideline-defined drug combinations (11.2% post-referral vs 10.1% baseline) or drug combinations and dosages (3.3% postreferral vs 2.7% baseline) was observed after cardiologist consultation.
Conclusions PREFER demonstrates substantial suboptimal treatment of HFrEF patients in the real world. Referral of patients with elevated NT-pro-BNP levels from PC to cardiologist did not result in meaningful treatment optimisation for treatments with known mortality and morbidity benefit.
- heart failure
- primary care
- outcome assessment
- health care
Data availability statement
Data may be obtained from a third party and are not publicly available. Data may be available on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known about this subject?
Despite considerable advances in the pharmacological and non-pharmacological treatment of heart failure (HF) over the last two to three decades, the mortality and morbidity remains high. In part, this can be due to the ‘implementation gap’ between guideline recommendations and clinical practice. In the majority of European countries, most patients with HF in primary care are managed by general physicians in concert with cardiologists. Previous studies have shown that HF diagnosis and management in primary care often remains inadequate, especially in patients perceived as clinically stable.
What does this study add?
N-terminal-pro-B-type natriuretic peptide (NT-pro-BNP) is a good prognostic marker to predict all-cause and cardiovascular death in stable patients with HF and may offer a means of identifying patients at higher risk of adverse outcomes. PRospective Evaluation of natriuretic peptide-based reFERral of patients with chronic HF in primary care is one of the few studies that uses a biomarker-based (NT-pro-BNP) approach as a clinical tool for referral of HF with reduced ejection fraction (HFrEF) patients from primary care to cardiologists. However, referral of patients with considerable elevated NT-pro-BNP levels from primary care to cardiologists did not result in meaningful treatment optimisation by the cardiologists.
How might this impact on clinical practice?
Despite well-defined guidelines for the treatment of HFrEF, adherence to recommendations is often below par, leading to suboptimal management of patients. For this reason, strategies to improve adherence to evidence-based therapies are needed.
Introduction
Heart failure (HF) is a leading cause of mortality and morbidity and is associated with significant socioeconomic burden.1 Despite considerable advances in HF pharmacological and non-pharmacological treatment, mortality and morbidity remain high,2 perhaps partially due to an ‘implementation gap’ between guideline recommendations and clinical practice.3 HF diagnosis and treatment in primary care (PC) often remains inadequate.3 4 A half-day training session for PC physicians (PCPs) did not improve the evidence-based drug treatment of HF with reduced ejection fraction (HFrEF).5
Undertreatment or non-compliance with guideline-directed medical therapy (GDMT) is a leading cause of hospitalisation.6 In patients with HF managed by cardiologists and at specialised HF outpatient clinics, improved adherence to HF guidelines is associated with decreased HF severity, long-term mortality7 and prevention of acute HF admissions.8 Contemporary data on patients with HF managed by PCPs are scarce, but adherence is lower among patients managed by PC centres compared with cardiology specialty centres.4 9–12
Patients with HF are often considered clinically stable if they show no signs and symptoms of a worsening disease state. In the 2016 European Society of Cardiology (ESC) guidelines for the diagnosis and treatment of acute and chronic HF, clinically stable HFrEF are recommended (level I-A) concomitant treatment with a b-blocker and an ACE inhibitor (ACEI), or an angiotensin receptor blocker (ARB) if an ACEI is not tolerated. In patients who remain symptomatic and have a left ventricular ejection fraction (LVEF) ≤35%, a mineralocorticoid receptor antagonist (MRA) is recommended to be added (level I-A).2 13 As HF is a progressive disease, it may be desirable to identify patients who are suboptimally treated and thus at higher risk of decompensation, despite appearing ‘clinically stable’.14 N-terminal-pro-B-type natriuretic peptide (NT-pro-BNP) is a prognostic biomarker of all-cause and cardiovascular death in stable patients with HF15 and may support to identify patients at higher risk of adverse outcomes.
Referral of selected patients with HF from PC to cardiologists could improve adherence to GDMTs, resulting in better clinical outcome. To test this hypothesis, we assessed whether one time referral of clinically stable, high-risk HFrEF patients (with elevated NT-pro-BNP) from PCPs to cardiologist across Europe would lead to treatment optimisation. Here treatment optimisation was defined as adherence to HF treatment recommendations per ESC guidelines. In addition, data from this study were used to understand demographic, clinical and treatment characteristics of clinically stable patients with HF with elevated NT-pro-BNP levels who are managed in the PC setting across Europe.
Methods
Study design
The PRospective Evaluation of natriuretic peptide-based reFERral of patients with chronic HF in PC (PREFER) trial (NCT02807857) was an international, prospective study enrolling HFrEF patients (LVEF ≤40%) from 223 PC settings in 18 countries in Europe. The study enrolled consecutive adult HFrEF patients (evidence of LVEF ≤40% at any point in the patient’s medical history) routinely visiting their PCPs (enrolled set) (online supplemental material, inclusion)/exclusion criteria, enrolled set). All patients provided signed informed consent prior to collection of any data. All PCPs and cardiologists were aware that their therapy decisions were being monitored. The study was conducted in compliance with Good Clinical Practice and according to the ethical principles laid down in the Declaration of Helsinki.
Supplemental material
The study composed of three visits to PCPs over a maximum period of 10 months (figure 1). Patients assessed by PCPs as clinically stable (whose PCP did not consider it necessary to amend the ongoing HFrEF treatment during baseline visit and whose HFrEF treatment had not changed in the 3 months before the baseline visit) and with NT-pro-BNP ≥600 pg/mL were referred to a cardiologist and were followed up till the end of study (follow-up set). In the referral letter, the PCP specified that the patient had stable HFrEF and that the referral was based on the specified NT-pro-BNP level. The cardiologist was requested to assess the patient for potential treatment optimisation.

Study design. *Where the PCP did not consider it necessary to amend the ongoing HFrEF treatment during baseline visit and whose HFrEF treatment had not changed in the 3 months prior to the baseline visit. HF, heart failure; HFrEF, heart failure with reduced ejection fraction; NT-pro-BNP, N-terminal-pro-B-type natriuretic peptide; PCP, primary care physician.
Study outcomes
The primary study objective was to assess whether NT-pro-BNP measurement-guided cardiologist referral of chronic HFrEF patients, otherwise considered clinically stable by their PCPs, would lead to optimisation of HFrEF treatment as recommended in ESC HF guidelines. Two levels of guideline adherence were used for the analysis (table 1). Guideline adherence was defined as prescription of HFrEF indicated drugs (level I-A) for a given patient’s clinical status at a dose ≥50% of ESC guideline-recommended daily dose. Only pharmacotherapies with established HF disease-modifying doses based on randomised clinical trials (RCTs) in HFrEF as defined in the 2016 ESC HF guidelines2 and/or with an HFrEF indication (drugs recommended for the treatment of HFrEF by the ESC guidelines) were considered relevant for the primary analysis. The cardiologist’s advice was analysed within the follow-up set (online supplemental information) on cardiologist’s advice). The primary outcome of adherence to ESC HF guidelines after referral to specialist was assessed at visit 2 (within 4 weeks of cardiologist’s referral and no later than 6 months after the baseline visit).
Definitions of levels of guideline adherence*
A key secondary objective of the study was to document the current PC management practice of HFrEF patients (online supplemental table S1). The HF treatment was analysed by assessing prescription rates for HF treatments derived from the patient’s PC chart.
HF hospitalisation history and emergency department admissions due to HF over the 12 months before baseline were recorded. All adverse events (AEs) and serious AEs (SAEs) were documented.
Statistical analysis
The enrolled set comprised all eligible patients entering the study. The follow-up set comprised patients entering the prospective period of the study (patients referred to the cardiologist). Patients considered not clinically stable and/or with NT-pro-BNP <600 pg/mL did not enter the prospective period and so were excluded from the follow-up set, but their baseline information was documented and analysed as part of the enrolled set. The primary analysis on guideline adherence level 1 was performed by estimating the proportion of patients who were switched to an ESC guideline recommendation-adherent regimen after referral to a cardiologist. Respective frequency distributions of guideline adherence were provided for the follow-up set for every visit. LVEF values were not available for all patients judged by their PCPs as having HFrEF at baseline. Therefore, a sensitivity analysis was conducted wherein missing values for LVEF at baseline were replaced by ‘>35’. Further, adherence to ESC HF guideline recommendations was also assessed without considering use of MRAs. For the enrolled set, adherence to ESC HF guidelines was analysed and further stratified by inclusion into the prospective period of the study. As some drugs within ACEIs, ARBs and β-blockers do not have an HFrEF indication and/or are lacking evidence of efficacy/dose information in HFrEF (moexipril, zofenopril (both ACEIs); eprosartan, irbesartan, olmesartan medoxomil, telmisartan (all ARBs); and atenolol, betaxolol, sotalol (all β-blockers)), additional sensitivity analyses were performed for drugs regardless of HFrEF indication/evidence. nQuery Advisor V.7.0 was used for sample size calculations. Previous studies estimated that adherence to ESC guideline-recommended HF drug dose for patients with CHF managed by PCPs increased from 20% to 30% following referral to a cardiologist.4 4 9 9 12 12 Based on this, 2160 patients would be required to enter the prospective period of the study in order to estimate treatment optimisation in 25% of patients with a precision of ±2% using a 95% CI, and a subgroup analysis with a precision of ±5%. After adjusting for the number of patients with NT-pro-BNP ≥600 pg/mL at baseline and a 10% drop-out rate, we planned to enlist 4000 patients with ~2400 patients estimated to enter the prospective period (follow-up set).
Interim analysis
An interim analysis was performed on 1 February 2018, with the first 1041 patients included, 629 of whom had entered the prospective period. As the assumptions for the sample size calculation were based on small datasets bound with uncertainty, the interim analysis aimed to assess whether statistical assumptions for the study were appropriate and to perform an analysis for the primary objective. The interim analysis showed no increase in adherence to ESC guidelines among patients referred to cardiologists. Based on this, a decision to prematurely terminate the study was taken by the sponsor in collaboration with the study steering committee.
Results
Patient disposition
Due to early termination of the study, only 1415 of the planned ~4000 patients were enrolled. Patient disposition is summarised in figure 2. Both criteria (NT-pro-BNP and clinical stability) were fulfilled by 864 patients, of whom 861 had been referred to a cardiologist. The country-specific analysis set is given in online supplemental table S2. The baseline prevalence of comorbid diseases is presented in online supplemental table S3; hypertension (74.2% (1047/1415)) was the most common comorbidity.
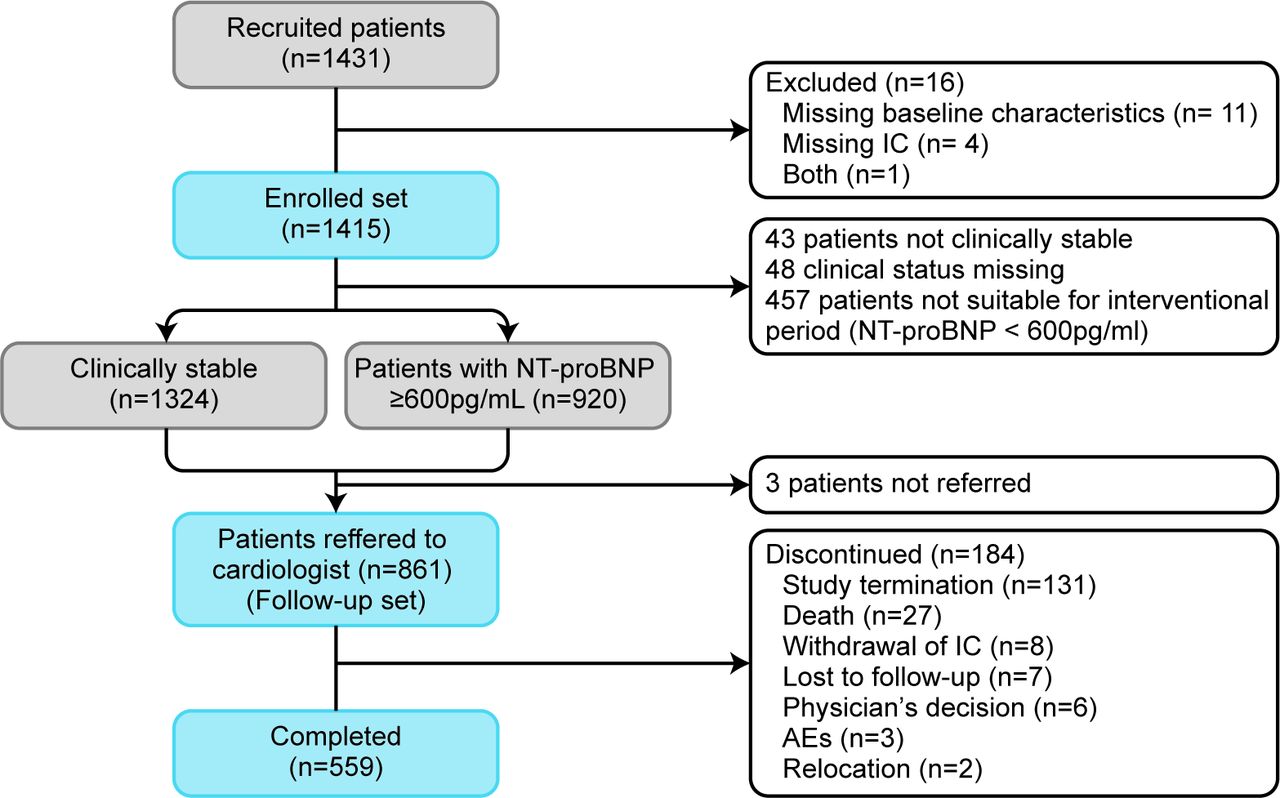
Patient disposition. Few patients were either ‘not clinically stable’ or clinical stability data were missing (but had increased NT-pro-BNP levels). AEs, adverse events; IC, informed consent; NT-pro-BNP, N-terminal-pro-B-type natriuretic peptide.
Demographic and other baseline characteristics
Most patients were male (69.2%), mean age was 69.8 years, and the average HFrEF duration was more than 6 years. At baseline, most patients (60.9%) had an ischaemic HF aetiology (table 2). Most patients at baseline were in New York Heart Association (NYHA) functional class II (table 2). Mean heart rate was ~72 bpm and mean systolic blood pressure (BP)/diastolic BP and renal function at baseline (assessed by estimated glomerular filtration rate (eGFR)) were similar in the overall cohort and those referred to cardiologists (table 2). As per study design, NT-pro-BNP levels were substantially lower in patients not referred to cardiologists. Of note, 50% of referred patients had an NT-pro-BNP level >2000 pg/mL (table 2). In the 12 months before the study, 44.4% (628/1415) of patients had visited an HF outpatient clinic or a cardiologist an average of 2.1 times (online supplemental table S4). LVEF was assessed at visits 1, 2, and 3. At visit 2, echocardiograms were requested mainly by the cardiologist for 30.3% of patients. At visit 3, echocardiograms were less frequently performed (9.2%). For patients where echocardiogram was performed, mean LVEF was <40% at visits 2 and 3 (online supplemental table S5).
Demographics, baseline characteristics and disease status
Primary outcomes
At the baseline, 279 patients could not be classified according to adherence in the follow-up set due to missing LVEF values, and the analysis included 582 patients. At baseline visit, 10.1% (59/582) of patients in the follow-up set were on guideline-adherent treatment with respect to drug types (level 1) and 2.7% (16/582) with respect to drug types and drug dose (level 2) (figure 3). Postreferral, 15 (3.3%, 95% CI 1.8% to 5.4%) patients who were on non-adherent guideline treatment at baseline became adherent at level 1, whereas 4 (0.8%, 95% CI 0.2% to 2.1%) patients who were non-adherent at baseline became adherent postreferral according to the guideline at level 2. However, 11/53 (20.8%, 95% CI 10.8% to 34.1%, 6 patients missing) of patients on ESC guideline-adherent treatment at baseline became non-adherent postreferral (level 1). When the adherence to ESC guideline was analysed with missing LVEF treated as >35% at visit 2 for follow-up set, adherence to ESC guidelines did not meaningfully improve following cardiologist referral; postreferral adherence rates were 11.2% (85/753) and 3.3% (28/753), respectively, for levels 1 and 2. There were no significant differences in adherence between baseline and postreferral population among Western and Eastern Europe (online supplemental table S6).

Adherence to ESC guidelinesa (follow-up set). aAs recommended by the ESC guidelines available at the time of patient recruitment. bTreatment with an ACEI or sacubitril/valsartan or an ARB (only HF treatment), in combination with a β-blocker and an MRA for patients with an LVEF ≤35% at baseline visit. Treatment with an ACEI (only HF treatment) or sacubitril/valsartan or an ARB, in combination with a β-blocker but without an MRA for patients with an LVEF >35% at baseline visit. cGuideline adherence with respect to drug types and dosage of all respective guideline-defined drugs ≥50% of the recommended target dose. ACEI, ACE inhibitor; ARB, angiotensin receptor blocker; ESC, European Society of Cardiology; HF, heart failure; LVEF, left ventricular ejection fraction; MRA, mineralocorticoid receptor antagonist.
Prespecified sensitivity analyses
The primary analysis used stringent criteria to quantify true adherence to ESC guidelines; the use of ACEIs, ARBs and β-blockers without an HFrEF indication and/or lack of documented evidence of efficacy/dosage were categorised as ‘non-adherent to guidelines’. A prespecified supportive analysis included patients treated with drugs lacking HFrEF indication/evidence. In the supportive analysis, baseline guideline adherence level 1 was slightly higher for enrolled and follow-up sets compared with the primary analyses (online supplemental table S7). At postreferral visit, 7.7% (35/457) patients on non-adherent treatment at baseline were put on adherent treatment. In contrast, only a few initially adherent patients became non-adherent at postreferral visit (13.7%) compared with the primary analysis. The overall proportions of patients with ESC guideline-adherent treatment increased slightly at postreferral visit to 15.3%. An LVEF value was unavailable in 279 patients in the follow-up set, thus, these patients were not included in the primary analysis. However, changes in guideline adherence between baseline visit and postreferral visit did not differ from the primary analysis when missing LVEF values at baseline were replaced by ‘>35%’. Similarly, there was no change in ESC guideline adherence without considering requirement of MRA in patients with known LVEF (online supplemental table S7).
These different sensitivity analyses characterise adherence to ESC guidelines with a more pragmatic approach than in the stringent definitions of the primary analysis. Renal function, serum potassium, heart rate and BP were unlikely to be major barriers for initiation and/or uptitration of the therapies in most of the patients during the study (table 2 and online supplemental table S8).
Secondary outcomes
Pharmacological treatments of interest
We analysed treatment patterns independently of the strict ESC guideline-adherence requirement applied for the primary analysis. Figure 4A shows the proportion of patients in the follow-up set with an HFrEF drug combination considering drugs with HFrEF indication/evidence; figure 4B shows HF treatment combinations without considering the need for HFrEF indication/evidence. These observations suggest that a substantial proportion of patients are prescribed ACEIs/ARBs and β-blockers that are not indicated for HFrEF. Generally, when assessing the prescribed drug classes independently of each other, the most prescribed drug class at baseline visit (follow-up set) was diuretics (72.6%), β-blockers (69.9%), drugs acting on the renin–angiotensin system (RAS; 57.0%), and MRAs (48.3%). At postreferral visit (follow-up set), the prescribed HFrEF disease-modifying drugs remained largely unchanged, except for an increase in the proportion of patients on MRAs and diuretics (absolute increase, 7.9% and 4.6%, respectively) verssus enrolled patients and patients in the follow-up group at baseline (figure 4C).
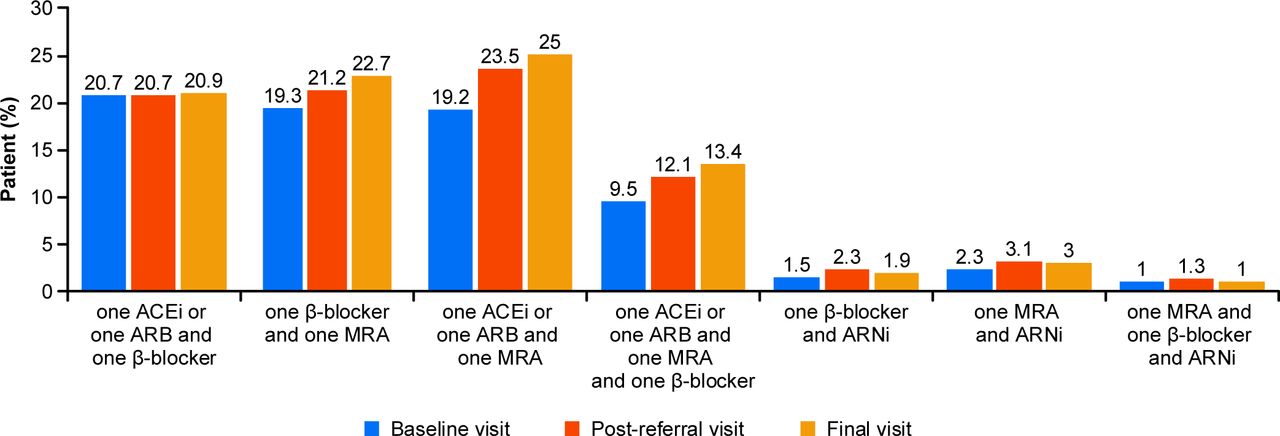
Combinations of treatment of interest by visit (follow-up set)a: (A) HF treatment combinations (only considering drugs with HFrEF indication/evidence); (B) HF treatment combinations (without considering need for HFrEF indication/evidence); (C) most frequently observed HF and non-HF treatments (>1% patients). aFrequency of patients with a specific HF treatment combination of drugs used for defining guideline adherence without considering LVEF. bCardiac therapy: amiodarone, digitalis glycosides, digitoxin, digoxin, glyceryl trinitrate, isosorbide dinitrate, isosorbide mononitrate, ivabradine, meldonium, metildigoxin, midodrine hydrochloride, molsidomine, nicorandil, ranolazine, sacubitril, trimetazidine. ACEI, ACE inhibitor; ARB, angiotensin receptor blocker; ARNI, angiotensin-neprilysin inhibitor; HF, heart failure; HFrEF, heart failure with reduced ejection fraction; LVEF, left ventricular ejection fraction; MRA, mineralocorticoid receptor antagonist.
Cardiologist’s advice
Cardiologists recommended no changes in current HF and non-HF therapy for 45.1% (337/748) of patients. Cardiologists advised treatment intensification, treatment reduction and general treatment adaption (ie, at least one advice for treatment intensification and one for treatment reduction) for 30.7%, 6.3% and 17.9% of patients (figure 5A), respectively. In most cases, all recommended changes were implemented by the cardiologist himself/herself (83.4%, 341/411; figure 5B) and for 88.0% (360/409) of the patients with recommended treatment changes, all changes were accepted and implemented by the PCP (figure 5C). Reasons for PCPs not accepting the cardiologist’s advice included unwillingness by patients, intolerance/AEs, previous treatment with other drugs of the same class, cost of therapy and lack of treatment reimbursement (data not shown). Advanced therapeutic procedures such as cardiac resynchronisation therapy device (CRT) implantable cardioverter defibrillator (ICD), left ventricular assist device (LVAD) requested by the cardiologists were only documented rarely at visit 2 and visit 3 (CRT-5 (0.7%) and 5 (0.7%); ICD-3 (0.4%) and 4 (0.7%); LVAD and heart transplantation-0 (0%), respectively).

Cardiologist’s advice, implementation and acceptance: (A) Cardiologist’s advice on treatment change; (B) implementation of changes by cardiologists himself/herself: HF and non-HF treatment; (C) Acceptance/implementation of cardiologist changes by primary care physicians: HF and non-HF treatment. aAT least one change implemented and one other change not implemented. bAt least one change accepted/implemented and one other change not accepted/implemented. HF, heart failure.
Guideline adherence and HF-related use of medical resources
At baseline visit, 49.2% (29/59) of ESC guideline-adherent patients had reported hospitalisations due to HF (average 1.8 hospitalisations) vs 39.8% (208/523) of non-adherent patients (average 1.4) in the past 12 months. Conversely, greater proportion of non-adherent patients had visited an outpatient clinic/cardiologist (48.4% (253/523)) than guideline-adherent patients (37.3% (22/59)) at the baseline visit.
Prospective safety
In the follow-up set, 256 patients (29.7%) experienced at least one AE during the study (online supplemental table S9) and 114 patients (13.2%) experienced an SAE during the study. SAEs causally linked to HF were most common (5.5%; 47/861). In total, 30 patients died (3.5%; follow-up set) during the study and HF was the most common cause of death (n=19). Among patients who completed the study, the rates of any AE, any SAE, and mortality during follow-up (mean 170 days, minimum 13 days, maximum 454 days) were 32.9%, 14.7% and 4%, respectively. Numbers in subgroups of interest are recorded in online supplemental file 2.
Supplemental material
Discussion
This large multinational, prospective low-intervention study evaluated treatment adjustments in HFrEF patients managed in PC who were considered ‘clinically stable’ by using natriuretic peptide (NP)-guided referral from PCPs to cardiologists.
Baseline adherence to ESC guidelines was remarkably low, and a referral of patients with elevated NP levels to cardiologists did not improve HFrEF treatment optimisation to a meaningful extent. The cardiologists did not increase the use of, or intensify disease-modifying HFrEF treatments such as β-blockers, ACEIs or ARBs. However, a slight increase in both diuretics and MRAs was observed between the first and last visit. The increase in diuretic use was possibly because cardiologists considered patients as symptomatic and/or congested and prioritised better symptom control over disease-modifying therapies.
Our findings show a significant gap in implementation of ESC guideline recommendations for HFrEF treatment in Europe, at both the PCP and cardiologist level, even in patients with considerably elevated NP values and despite most being symptomatic (~90% in NYHA class ≥II). In patients primarily managed by cardiologists, HF guideline adherence is reported to vary but is better than what we had observed. For instance, in the ESC-HF Long-Term Registry, the proportion of patients on disease-modifying treatment on target doses was 29.3% for ACEIs, 24.1% for ARBs, 17.5% for b-blockers and 30.5% for MRAs.9 However, in the recent CHAMP-HF study, <30% of patients received target doses of ACEIs/ARBs/angiotensin-neprilysin inhibitor (ARNIs)/MRAs/b-blockers16 and 22%10 were simultaneously prescribed ACEIs/ARBs/ARNIs, b-blockers and MRAs, with <1% receiving target doses. The use of diuretics was lower among patients enrolled in PREFER; notably, both CHAMP-HF and a Swedish cross-sectional study also had ~61% patients on diuretics.17 18 In contrast, the CHECK-HF registry reported considerably higher rates of ACEI/ARB (84%), b-blocker (86%) and MRA (56%) prescriptions, whereas the combination of an RAS inhibitor and β-blocker was 68.6% in HFrEF patients.11 One can only speculate about the potential barriers or clinical inertia that contribute to low adherence,19 and if a longer follow-up in PREFER could have potentially resulted in better optimisation.6 PREFER is unique as we studied seemingly ‘clinically stable’ HFrEF patients managed by PCPs, all with increased risk, mostly symptomatic, and all referred to cardiologists specifically for HF treatment optimisation. Although we rigorously defined ESC guideline treatment adherence, applying different sensitivity analyses did not alter the conclusions. Nor did we notice differences in guideline adherence between patients from Western versus Eastern Europe, which suggests that differences in regional treatment practices do not explain the low adherence to guidelines observed.
In the PREFER study, all-cause mortality rate was low (3.5%) during the 6-month follow-up. In a previous study, mortality in patients without symptoms at the clinic visit was 22% at 5 years. This was 40% in patients who were symptomatic at 5 years, which was significantly higher than for patients who had never had symptoms nor signs (4% mortality at 5 years).20
Elevated NT-pro-BNP levels predict a significantly increased risk of adverse outcomes21 22 and have shown similar predictive validity on mortality and cardiovascular events as traditional outcomes in HF.23 24 Although cut-offs of NT-pro-BNP indicating an increased risk are not well defined, early treatment of high-risk patients with HF based on BNP/NT-pro-BNP testing might prevent or delay onset of HF.25 26 Whether NT-pro-BNP-based management improves outcomes in high-risk patients with stable HFrEF remains uncertain.27 28 Previous studies have shown that early treatment of those identified at high risk of HF based on BNP/NT-pro-BNP testing might prevent or delay onset of HF,25 26 suggesting that NPs have a potential for optimising HF management. However, these findings have not been consistently reported and further research is needed from more trials on NP-guided therapy.28
To our knowledge, PREFER is the first study to use NT-pro-BNP in stable HFrEF patients as a clinical tool for a referral from PC to cardiologists. The rationale for the cut-off value for NT-pro-BNP (600 pg/mL) in PREFER was pragmatic, based on insights from RCTs and, specifically, the 2016 ESC HF guidelines.2 29 30 Even in asymptomatic patients with HF (NT-pro-BNP >600 pg/mL), studies indicate that cardiologist referral may be beneficial31 and a study using BNP-guided collaborative care showed that an NP-based screening (BNP >50 pg/mL) approach reduced the incidence of left ventricular dysfunction and HF by ~50%.25 However, these cut-off values are not based on any specific underlying cardiac pathophysiology and there is currently limited evidence regarding the utility of higher/lower NT-pro-BNP cut-off values (figure 6).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Use of general cardiovascular therapies, not specific for heart failure, at each visit. MRAs, mineralocorticoid receptor antagonist.
There is a common misconception that therapeutic success is achieved when patients with HF have no or mild symptoms (NYHA class II) and are perceived as ‘clinically stable’, and such patients are likely to be undertreated as providers may believe that patients with milder symptoms have low morbidity and mortality.20 However, deterioration of cardiac structure and function is often subclinical and proceeds unrecognised, eventually increasing the patient’s risk of an adverse outcome.32 In PREFER, despite the majority of patients being in NYHA class II and considered ‘stable’, nearly two-thirds had markedly elevated NT-pro-BNP levels of ≥600 pg/mL, about half needed inpatient care in the 12 months prior to entering the study, and in the relatively short follow-up time, about 15% of referred patients experienced an SAE (majority causally related to HFrEF). These observations emphasise the need to optimise GDMT, even in patients considered mildly symptomatic or clinically stable, with a better multidisciplinary approach involving PCPs, cardiologists, nurses and pharmacists.32
PARADIGM-HF run-in study assessed the tolerability of sacubitril/valsartan and enalapril at target dose (200 mg two times per day) in patients with HF. In this study, 80% of patients tolerated the target dose and many patients with low BP, eGFR <60 mL/min per 1.73 m2, and more advanced HF were successfully randomised.33 This study results indicate that eGFR or hypotension are unlikely to be a major barrier to prevent therapy in ~90% of patients, although it is likely to influence treatment decisions in some patients. However, these factors were not considered while assessing the primary outcome of adherence to ESC guideline recommendation. The low rate of adherence observed limits precision of estimates in further subgroups. Hence, statistical analysis of confounding factors such as renal function and hypotension were not performed.
The main limitation of PREFER was its premature termination, which in turn led to significant loss to follow-up. Since the recruitment to the trial before study termination was across multiple sites and eligible subjects were recruited from routine follow-up in PC, systematic bias is unlikely among subjects included in the analysis. However, the loss to follow-up did not affect adherence to ESC guideline-recommended pharmacotherapy. The sensitivity analysis partly addressed this limitation. Furthermore, the study included a representational portion of patients from European countries, although some countries with close general practitioner (GP)-specialist collaboration (United Kingdom, Netherlands and Germany) were unable to participate in this pragmatic trial for a variety of reasons. Patients recruited in PREFER were consecutive HFrEF patients visiting their GP. A limitation could have been selection bias of patients during the assessment of ‘clinical stability.’ However, despite being assessed as stable, this population of patients with HF had significant morbidity; the majority were symptomatic, and 3.5% died during the relatively short follow-up. An encouraging note is that in ~88% of cases wherein cardiologists had advised a treatment change, PCPs accepted and implemented the recommendation. Other limitations were the reduced sample size of the study because of early termination.
In conclusion, we demonstrate major clinical inertia in HFrEF patients managed in 18 countries in Europe. Patients are substantially undertreated in PC and yet a simple prompt for referral of high-risk patients to specialist care, based on elevated NT-pro-BNP level, did not result in substantial management changes. This was despite this contemporary HF population reporting high prior healthcare utilisation and being a population wherein preventive management strategies should be beneficial. There is an urgent need to develop health system care strategies to improve evidence-based guideline implementation and adherence.
Data availability statement
Data may be obtained from a third party and are not publicly available. Data may be available on reasonable request.
Ethics statements
Patient consent for publication
Acknowledgments
Medical writing and editorial assistance were provided by Shweta Vadnerkar and Viswanatha Matada (Novartis Healthcare, Hyderabad, India). The authors are grateful to all the patients who participated as well as the study site personnel. Central clinical trial operational management was provided by Paul Hoper, Svenja Mix-Geldern and Paloma de la Fuente. Contribution from the study monitors and support from the management personnel was appreciated.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors All authors contributed to the intellectual conceptualisation of PREFER, study design, planning and collection of PREFER data. MO contributed to the statistical analysis. All authors interpreted the data, drafted and reviewed the manuscript. All authors approved the submitted manuscript.
Funding This work was supported by Novartis Pharma AG.
Competing interests RH acknowledges his part-funding from the National Institute for Health Research (NIHR) School for Primary Care Research, the NIHR Collaboration for Leadership in Health Research and Care (CLARHC) Oxford, the NIHR Oxford Biomedical Research Centre (BRC, UHT), and the NIHR Oxford Medtech and In-Vitro Diagnostics Co-operative (MIC) and has received occasional fees for consulting or speaking from companies including Novartis. RH and PF are employees of Novartis. HB receives research funding from the Instituto de Salud Carlos III, Spain (PIE16/00021 & PI17/01799), Astra-Zeneca, BMS, Janssen and Novartis and has received consulting fees from Astra-Zeneca, Bayer, BMS-Pfizer, Novartis; and speaking fees or support for attending scientific meetings from Astra-Zeneca, Bayer, BMS-Pfizer, Novartis, and MEDSCAPE-the heart.og. YMP received consultancy fees from Novartis, Roche Diagnostics and holds minority shares in a University spin-off. FG has received fees for consulting and speaking honoraria from Novartis, Carmat, Orion and fees for consulting, speaking and as an investigator from Abbott. He has also received research grant from Orion and speaking honoraria from Boehringer-Ingelheim and received fees for consulting from Bayer and Pfizer. MO has been contracted by Novartis.
Provenance and peer review Not commissioned; externally peer reviewed.