Article Text

Abstract
Background The main aim was to examine age-specific risk factor associations with incident atrial fibrillation (AF) and their attributable fraction in a large European cohort. Additionally, we aimed to examine risk of stroke and mortality in relation to new-onset AF across age.
Methods We used individual-level data (n=66 951, 49.1% men, age range 40–98 years at baseline) from five European cohorts of the MOnica Risk, Genetics, Archiving and Monograph Consortium. The participants were followed for incident AF for up to 10 years and the association with modifiable risk factors from the baseline examinations (body mass index (BMI), hypertension, diabetes, daily smoking, alcohol consumption and history of stroke and myocardial infarction (MI)) was examined. Additionally, the participants were followed up for incident stroke and all-cause mortality after new-onset AF.
Results AF incidence increased from 0.9 per 1000 person-years at baseline age 40–49 years, to 17.7 at baseline age ≥70 years. Multivariable-adjusted Cox models showed that higher BMI, hypertension, high alcohol consumption and a history of stroke or MI were associated with increased risk of AF across age groups (p<0.05). Between 30% and 40% of the AF risk could be attributed to BMI, hypertension and a history of stroke or MI. New-onset AF was associated with a twofold increase in risk of stroke and death at ages≥70 years (p≤0.001).
Conclusion In this large European cohort aged 40 years and above, risk of AF was largely attributed to BMI, high alcohol consumption and a history MI or stroke from middle age. Thus, preventive measures for AF should target risk factors such as obesity and hypertension from early age and continue throughout life.
- atrial fibrillation
- risk factors
- stroke
- epidemiology
Data availability statement
The data are not available in a public repository. Access to the data is restricted by the ethical approvals and the legislation of the European Union and the countries of each MORGAM study. Approval by the Principal Investigator of each cohort study and the MORGAM/BiomarCaRE Steering Group will be required for release of the data. The MORGAM Manual at https://www.thl.fi/publications/morgam/manual/contents.htm gives more information on access to the data.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known about this subject?
Modifiable risk factors for atrial fibrillation (AF), such as obesity, hypertension, diabetes, smoking and previous cardiovascular disease, may together account for more than 50% of the AF burden. However, although risk factors for AF have been extensively examined, limited attention has been devoted to their attributable fraction in relation to age.
What does this study add?
In this large cohort of adult and elderly European men and women, risk of AF was primarily attributed to body mass index, hypertension and previous stroke or myocardial infarction, together explaining 30%–40% of the AF risk. Population attributable risk varied with age, with a substantial AF burden attributed to body mass index at ages 40–69 years, whereas population attributable risk for hypertension was highest and significant only at ages ≥60 years. The AF risk attributed to previous myocardial infarction or stroke increased slightly with age.
How might this impact on clinical practice?
Increased understanding of the relative contribution of modifiable risk factors to the development of AF, as well as complications of AF across age groups, would help target prevention and allocate healthcare resources specific to age group needs.
Introduction
Atrial fibrillation (AF) has become a disease with significant public health impact, estimated to affect 20 million men and 12 million women worldwide.1 Major complications of AF include stroke,2 hospitalisations3 and mortality.4 Several predictors for AF have been described, including modifiable risk factors such as obesity, hypertension, diabetes, smoking and previous cardiovascular disease,5–7 which may together account for more than 50% of the AF burden.8 AF incidence increases with age9–11 and is commonly related to the presence of cardiovascular risk factors or disease in older individuals.12 On the other hand, transition to unhealthy metabolic risk factor constellations occurs earlier in life,13 and a recent study suggests that even in early-onset AF, 90% of individuals had metabolic risk factors and comorbidities.14 Although several large cohort studies have addressed the role of lifestyle risk factor for AF15 16 and potential sex differences,17 there is a lack of research on the impact of the risk factors in relation to age at AF onset.
Increased understanding of the contribution of modifiable risk factors in relation to age at AF onset, as well as complications of AF across age groups, would help target prevention and allocate healthcare resources specific to age group needs. The MOnica Risk, Genetics, Archiving and Monograph (MORGAM) consortium provides a unique opportunity to expand the understanding of AF risk factors and complications from middle aged to older individuals. The main aim of this study was to examine age-specific risk factor associations with incident AF and their attributable fraction in European adults and elderly. Furthermore, we aimed to examine the risk of stroke and all-cause mortality after new-onset AF at different ages.
Methods
Study population
This study is based on the MORGAM consortium, which is a multinational collaborative initiative addressing cardiovascular biomarkers, risk factors and endpoints using pooled and harmonised data from European community-based cohorts.18 In this study, individual-level data from five cohort studies in the MORGAM consortium18; DAN-MONICA (Denmark),19 FINRISK (Finland)20 Moli-sani (Italy),21 Northern Sweden MONICA,22 and the Tromsø Study (Norway)23 were included. Cohort-specific procedures for enrolment and follow-up are provided in the online supplemental D1. In brief, all included cohort studies are population-based with repeated surveys. The studies included in MORGAM are population-based studies covering a specific region in several European countries, recruiting from birth cohorts or random sampling from a national or local population register. Most studies do not specify exclusion criteria.
Supplemental material
In total, 66 951 individuals from the five MORGAM cohort studies were included in our analyses, after exclusion due to left censoring (n=448), prevalent AF at baseline (n=879) and/or missing baseline AF information (n=6757). Only individuals aged ≥40 years at baseline were included in order to harmonise the age range.
Risk factors and biomarkers
Data on risk factors were available from the baseline examinations, which were conducted between 1982 and 2010. Systolic blood pressure (SBP), total cholesterol, weight and height were measured by standardised methods and body mass index (BMI) (kg/m2) was calculated. Information on daily smoking, average alcohol consumption, diabetes, antihypertensive medication, history of stroke and myocardial infarction (MI) was self-reported. Harmonised data from the various studies were transferred to the MORGAM Data Centre in Helsinki.24
Biomarkers were available for 39%–49% of the participants (available in FINRISK, Moli-sani, Northern Sweden, and Dan-MONICA) (online supplemental tables S1–S5). Measurements from stored blood samples include C reactive protein (CRP) (n=32 893), which was determined by latex immunoassay CRP16 (Abbott, Architect c8000), and N-terminal-pro B-type natriuretic peptide (Nt-pro-BNP) (n=26 048, measured on the ELECSYS 2010 platform using an electrochemiluminescence immunoassay (Roche Diagnostics). Analyses of estimated glomerular filtration rate (eGFR), CRP, and Nt-proBNP are described in detail elsewhere.25
Follow-up for AF, stroke and mortality
Incident AF, non-fatal and fatal stroke events, and death during follow-up were identified by linkage to regional or national hospital discharge registries, diagnosis registries, and causes of death registries, which were also screened for incident AF as a comorbidity of individuals who died of other causes. Follow-up lasted from the date of the baseline examinations to the end of 2010 (DAN-MONICA, Tromsø and FINRISK) or 2011 (Moli-sani and Northern Sweden), truncated at 10 years for the data analysis (median (IQR): 10.0 (4.8–10.0) years).
Statistical analyses
For each age group (40–49, 50–59, 60–69 and ≥70 years at baseline), AF incidence rates were calculated as the number of AF cases per 1000 person-years within the 10-year follow-up period. The association between risk factors and incident AF within each age stratum was estimated as HR with 95% CI using Cox regression. The goodness-of-fit of all Cox models was checked with respect to the proportional hazard (PH) assumption. In order to assure that the PH assumption was valid during the Cox regressions, interactions with time were adjusted for when needed. The PH assumptions were tested using the Schoenfeld residuals. Prevalent AF cases were excluded from the analysis. Multivariable-adjusted models include adjustment for age, sex, BMI, hypertension (SBP ≥140 mm Hg and/or taking antihypertensive drugs), total serum cholesterol, smoking, history of diabetes, alcohol consumption and study site. We set the follow-up duration to a fixed maximum value (10 years) to avoid large differences in follow-up. Missing data were handled by using available cases.
Population attributable fraction (PAF) was calculated for each categorical risk factor. In each age group, the PAF for a risk factor was estimated using the fully adjusted estimated HRs and the following equation26:

where PAFi is the PAF of the i-th category, HRi is the fully adjusted HR for the i-th category, pdi is the proportion of those in the i-th category among the cases during the first 5 years of the follow-up. The total PAF of a risk factor was calculated as the sum of all PAFi over i=1 to n, where n is the number of categories of the risk factor in question. For each PAFi and PAF, a 95% CI was calculated using bootstrapping. Bootstrapping was also used to estimate the p values for the differences between PAFs of different age groups for the same risk factor. To decide whether a difference was significant, a (Bonferroni-corrected) alpha level of 0.05/N was used, where N is the number of comparisons per risk factor category level (there are four age groups, so N is (4×4–4)/2=6, so alpha=0.05/6=0.008).
In online supplemental table S6, second-order interactions between covariates were included if they reached significance (taking into account multiple testing). Interactions with time since baseline (included in the analysis as a time-varying covariate) were included when needed to avoid violations of the PH assumption. The PAF analyses used fully adjusted HRs.
In order to estimate the HRs of new-onset AF for stroke and mortality by age-decades, time-dependent multiple adjusted Cox regressions were performed in each age stratum where incident AF was used to predict time to event (where event is (1) stroke and (2) mortality). For the stroke analysis, cases with previous stroke history were excluded.
Analyses were performed in R V.3.5.3, in which Cox regressions were performed using the survival package. We assumed a two-tailed p<0.05 as statistically significant.
Results
The median age at baseline was 53.5 years (IQR 46.4–61.2), ranging from 40 to 98 years, and 49.1% of the 66 951 participants were men (table 1). The prevalence of previous disease (diabetes and history of MI or stroke) was low (<6%), although more than half of the participants (52.2%) had an SBP ≥140 mm Hg or were taking antihypertensive drugs. About one-fourth (26.0%) of the participants smoked daily. Study characteristics by cohort are shown in online supplemental tables S1–S5. Risk factor distributions at baseline were in general more favourable at younger age (table 2). Prevalence of hypertension, overweight, diabetes and previous MI or stroke increased with age, whereas smoking decreased gradually by age, and daily consumption of alcohol showed a stable pattern across all age groups.
Baseline characteristics of the pooled MORGAM cohort (n=66 951)
Risk factor distribution by age groups at baseline
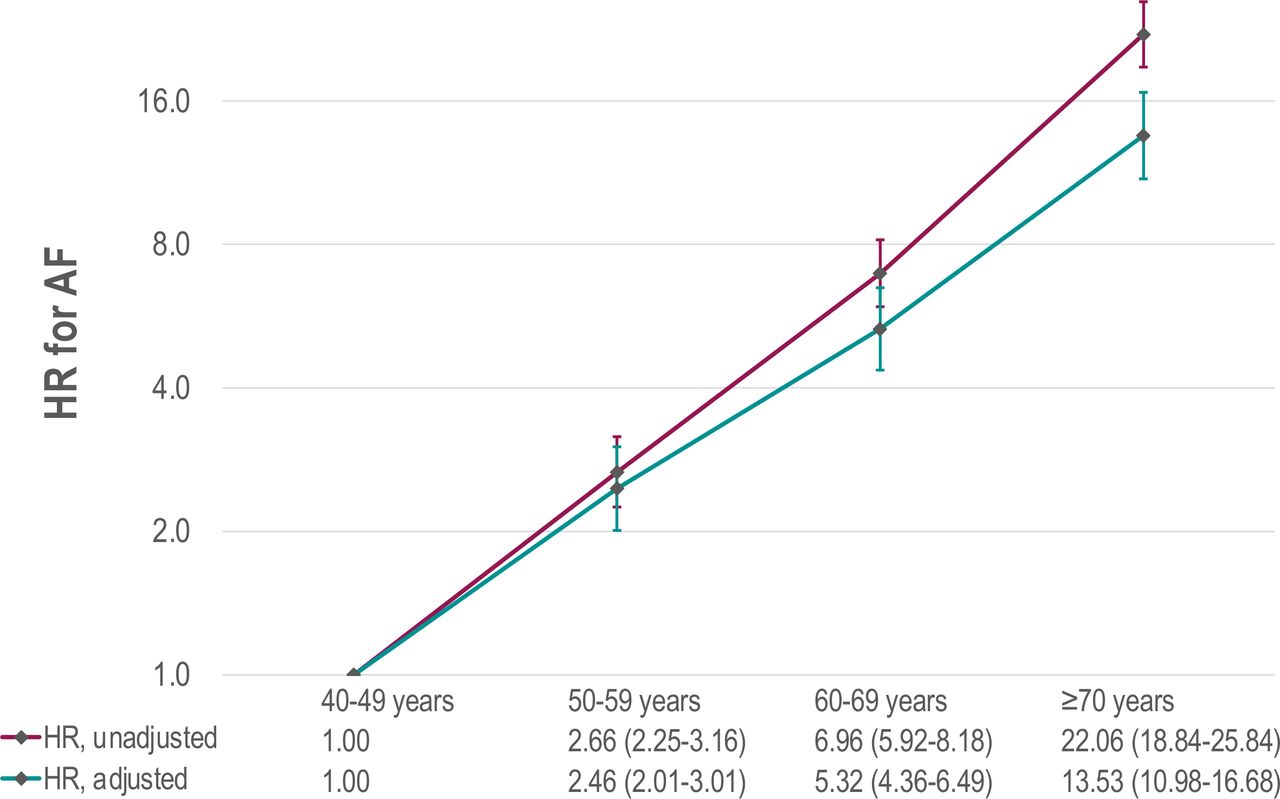
Over a follow-up time of up to 10.0 years, 2021 (3.0%) cases of AF were detected. AF incidence rate increased gradually from 0.9 per 1000 person-years at age 40–49 years to 17.7 at the age of ≥70 years. Adjusted HR for AF increased exponentially with age and was 13.5 times higher (HR 13.53, 95% CI 10.98 to 16.68) at ages ≥70 compared with 40–49 years (figure 1).

Risk of AF by age groups, presented as HR with 95% CI. HRs were presented on a log scale with base 2, adjusted for sex, BMI, SBP, total serum cholesterol, daily smoking, history of diabetes, antihypertensive drugs, daily alcohol consumption, and study site. AF, atrial fibrillation; BMI, body mass index; SBP, systolic blood pressure.
Age-stratified unadjusted risk of AF for each risk factor is shown in online supplemental table S7. Age-stratified multivariable-adjusted Cox regression models showed that BMI and a history of MI or stroke were consistently associated with increased risk of AF in all age groups (p<0.001) (table 3), whereas high alcohol consumption, total serum cholesterol, and hypertension increased the risk of AF only at certain ages. For each 5 kg/m2 increase in BMI, risk of AF increased significantly with 37%–41% (p≤0.001) at ages 40–69 years. At the age of ≥70 years, AF risk was still positively associated with BMI (HR 1.17, 95% CI 1.06 to 1.29), but the risk was lower than at younger ages (difference from ages 40-69: p≤0.033). A history of MI or stroke significantly increased the risk of AF (p≤0.001 at all ages), with highest HRs at age 40–49 years (HR 4.60, 95% CI 2.56 to 8.27; p≥0.011 compared with other age groups). High alcohol consumption significantly increased the risk of AF by 13%–18% at ages up to 70 years (p<0.05), but not in participants ≥70 years. Total serum cholesterol decreased the risk of AF by 4%–11%, but significantly only at ages 50–69 years (p<0.05), whereas hypertension increased the risk of AF by 19%–40%, although significantly only at older ages (≥60 years) (p<0.05). Smoking, CRP and eGFR were not significantly associated with AF, whereas participants with Nt-pro-BNP levels ≥900 pg/mL showed higher AF risk at all ages (p≤0.001).
Multivariable-adjusted HR for AF by age groups
Table 4 shows risk of AF attributed to each modifiable risk factor in age strata (ie, PAF for 5-year incident AF). Among lifestyle risk factors, BMI contributed to 8%–18% of the AF risk at ages <70, but at older ages, the relative attribution to BMI was low and non-significant (4.0%, 95% CI −1.31 to 9.20). Hypertension showed significant PAFs of 20% only at ages≥60 years, whereas diabetes showed a significant PAF only at ages≥70 years (6.0%, 95% CI 2.21 to 9.68). A history of stroke or MI contributed significantly to AF risk in all age groups with PAFs increasing gradually from 5% to 10%. Smoking and alcohol intake showed modest and non-significant PAFs. In general, 30%–40% of the AF risk could be attributed to BMI, hypertension and a history of stroke or MI.
Multivariable-adjusted population attributable fraction for AF by age groups
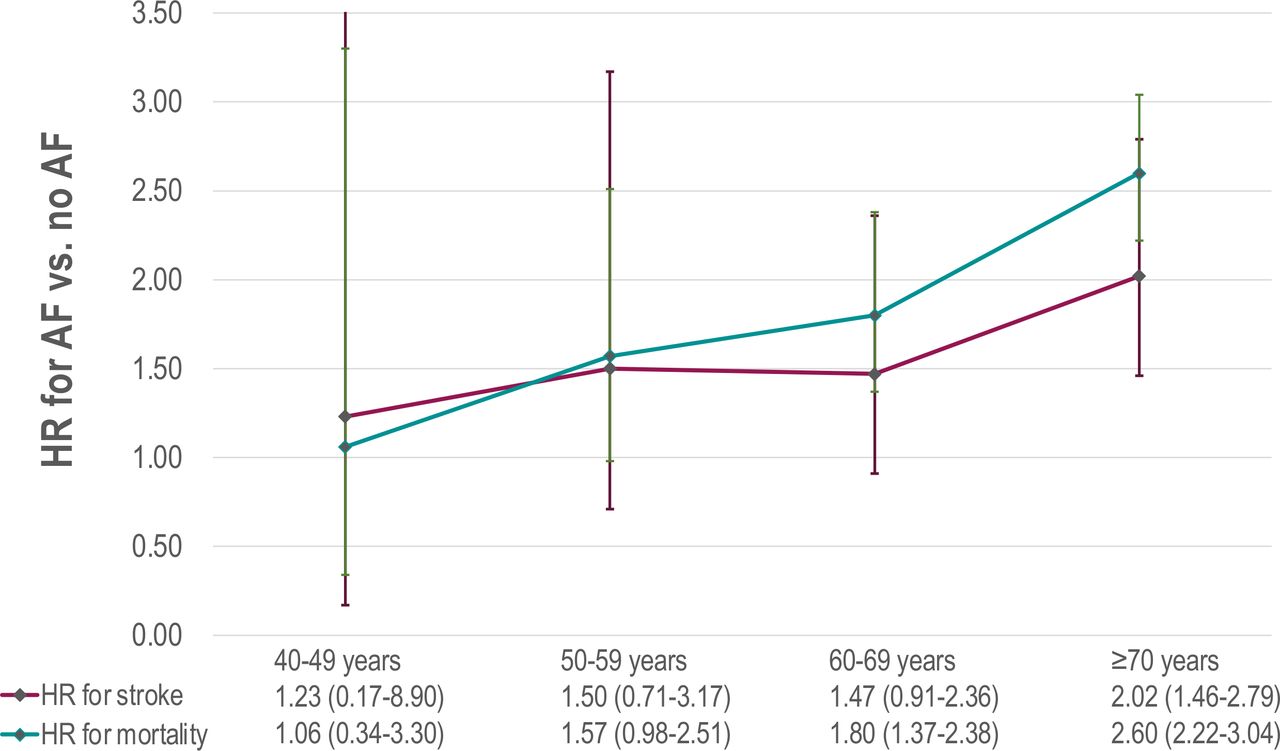
During the follow-up, 8.4% (n=5622) participants died, whereas 3.1% (n=2055) were diagnosed with stroke. New-onset AF was associated with a 1.8-fold to 2.6-fold increase in risk of death at ages ≥60 years (multivariable-adjusted p≤0.001, figure 2) and with a twofold risk of stroke at ages ≥70 years (HR 2.02, 95% CI 1.46 to 2.79, figure 2).

{kind=link}
{kind=link}
Risk of stroke and mortality according to new-onset AF versus no AF, presented as HR with 95% CI. HRs were adjusted for age, sex, BMI, SBP, total serum cholesterol, daily smoking, history of diabetes, antihypertensive drugs, daily alcohol consumption, and study site. AF, atrial fibrillation; BMI, body mass index; SBP, systolic blood pressure.
Discussion
In this large, community-based cohort, risk of new-onset AF was associated with several lifestyle-related risk factors such as overweight, hypertension, high alcohol consumption and a history of MI or stroke. In all age groups, AF burden was largely attributable to BMI, hypertension, and previous stroke or MI, together explaining 30%–40% of the AF risk. However, their PAF varied with age, as we found a substantial AF burden attributed to BMI at ages 40–69 years, but low PAF for BMI among the oldest. PAF for hypertension was highest and significant only at ages ≥60 years, whereas PAF for previous MI or stroke showed a slight increase with age. Finally, we found that newly diagnosed AF was associated with a twofold increase in risk of death and stroke but only at older ages.
AF incidence, risk factors and attributable risks
We observed a substantial increase in AF incidence with age that is comparable to age-specific incidence rates in the Rotterdam Study11 and the Reykjavik study9 but somewhat lower than the Framingham Study incidence rates.10 The increasing incidence of AF9–11 highlights the importance of modifiable risk factors,27 28 which can be targeted and may contribute to prevention or deferral of AF onset. In the present study, several modifiable risk factors such as BMI, previous MI or stroke, hypertension and alcohol consumption were associated with increased risk of AF, the first two consistently in all age groups. These observations are largely in agreement with a study of 10 million individuals in a national Korean health insurance database,29 which showed that modifiable risk factors such as BMI, high alcohol intake, and hypertension increased the risk of AF in all age groups.
Our study extends previous research by addressing the proportion of incident AF that could be attributed to a risk factor at different ages. The proportion of AF risk attributed to BMI increased with age up to 70 years, with PAFs of 15%–18% which is comparable to the Atherosclerosis Risk in Communities Study.8 At ages ≥70 years, PAF for BMI was low and not statistically significant, suggesting that at older ages new-onset AF is primarily attributed to factors other than BMI. The risk of AF attributed to hypertension was high at all ages with the highest attributable fractions in participants ≥60 years, accounting for 20% of incident AF, which is similar to results reported from other studies.8 30 As expected at population level, the risk of AF attributed to previous MI or stroke increased with age, possibly due to the observed age-related increase in prevalence of MI and stroke. Our findings underline the need to prevent and monitor cardiovascular risk factors and disease onset at an early age in order to prevent or postpone AF and its sequelae.
Stroke and mortality after AF onset
Increased risks of stroke and mortality are well-known complications of AF.17 However, age-specific complications of AF are scarcely examined in large cohorts, although clinically, older age is a strong predictor of stroke in AF patients,31 manifested through integration in stroke prediction scores such as the ABC and CHA2DS2-VASc scores. In the present study, AF significantly predicted stroke only at ages ≥70 years, with a twofold increase in stroke risk. This is in contrast to a large Danish study, showing increased stroke risks due to AF of 1.6–2.0 as early as the age of 50 years.32 Wolf et al2 found no differences in stroke risk due to AF with advancing age in the Framingham Study, although the proportion of strokes attributed to AF increased from 1.5% at ages 50–59 years to 23% at ages 80–89.2 Oral anticoagulation or alternative ways of stroke risk reduction need to be addressed thoroughly in all age groups, but with an emphasis in older patients.
We found that AF significantly increased the risk of death at ages ≥60 years, with a 1.8-fold to 2.6-fold increase in mortality in AF patients. A large cohort study of Japanese men and women showed similar mortality rates in relation to AF in the age range 40–69 years.33 However, AF itself accounts for a comparatively small fraction of deaths worldwide,1 since the mortality risk in AF patients is attributed to other causes such as heart failure and stroke.34
Limitations and strengths
The included cohorts originate from population-based studies to which entire birth cohorts or random samples were invited; however, we cannot rule out selection bias due to selective participation. Previous studies indicate that non-participants may have lower socioeconomic status and higher prevalences of non-communicable diseases.35 Participation among the oldest old was lower, which prompted us to merge data on participants >70 years, limiting knowledge among this specific group. We did not stratify by sex, as sex differences in AF risk factors were addressed previously in a similar cohort.17
Furthermore, misclassification and lack of valid data on potential residual confounders such as physical activity may lead to biased estimates. Combining data from heterogeneous cohorts may introduce misclassification, although we attempted to improve the goodness-of-fit of the Cox models by adjusting for study cohort. Data on risk factors were available only at baseline, and procedures and thresholds may have changed during follow-up. Information on AF is derived from hospital discharge records and individuals with paroxysmal AF and silent AF are probably underrepresented, which may weaken the associations, although validation studies show high positive and negative predictive values for AF diagnoses from diagnosis registers.36 37
Strengths of this study include the prospective design with long-term follow-up, rigorously harmonised risk factors and endpoints and a large sample size, representing Europe from North to South.
Conclusions
In this cohort of adult and elderly European men and women, incidence of AF increased significantly with age. High BMI, hypertension, high alcohol consumption and previous stroke or MI predicted risk of AF across age groups. In particular, the PAF of BMI was substantial at ages 40–69 years, and a large proportion of the AF risk was attributed to hypertension, with an age-related increase. Therefore, preventive measures should target risk factors rigorously from middle-aged to older individuals. Newly diagnosed AF was associated with a high risk of stroke and mortality in risk factor adjusted analyses, in particular at older age. Our study, thus, emphasises the potential role of risk factor control for prevention and adequate patient management after AF diagnosis in the older age groups, including the oldest old.
Data availability statement
The data are not available in a public repository. Access to the data is restricted by the ethical approvals and the legislation of the European Union and the countries of each MORGAM study. Approval by the Principal Investigator of each cohort study and the MORGAM/BiomarCaRE Steering Group will be required for release of the data. The MORGAM Manual at https://www.thl.fi/publications/morgam/manual/contents.htm gives more information on access to the data.
Ethics statements
Ethics approval
Each participating study was approved by the local ethics committee and/or institutional review board. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. Written or verbal informed consent was obtained from all individual participants.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @MorsethBente
Contributors RBS, BM, BG and M-LL contributed to the conception and the design of the work. M-LL, BG, BM, RBS, KK, VS, TJN, LI, SC, JKKV, IN, EBM, AL, TW, SS and LJ contributed to the acquisition, analysis or interpretation of data for the work. BM, RBS, BG and M-LL drafted the manuscript. All authors critically revised the manuscript. All gave final approval and agreed to be accountable for all aspects of work ensuring integrity and accuracy.
Funding The MORGAM Project has received funding from EU projects MORGAM (Biomed, BMH4-CT98-3183), GenomEUtwin (FP5, QLG2-CT-2002-01254), ENGAGE (FP7, HEALTH-F4-2007-201413), CHANCES (FP7, HEALTH-F3-2010-242244), BiomarCaRE (FP7, HEALTH-F2-2011-278913), euCanSHare (Horizon 2020, No. 825903) and AFFECT-EU (Horizon 2020, No. 847770); and Medical Research Council, London (G0601463, No. 80983: Biomarkers in the MORGAM Populations). This has supported central coordination, workshops and part of the activities of the MORGAM Data Centre, the MORGAM Laboratories and the MORGAM Participating Centres. TJN was supported by the Emil Aaltonen Foundation, Paavo Nurmi Foundation, Finnish Medical Foundation, and Academy of Finland (grant number 321351). RBS has received funding from the European Research Council (ERC) under the European Union’s Horizon 2020 research and innovation programme under the grant agreement No 648131, from the European Union’s Horizon 2020 research and innovation programme under the grant agreement No 847770 (AFFECT-EU) and German Center for Cardiovascular Research (DZHK e.V.) (81Z1710103); German Ministry of Research and Education (BMBF 01ZX1408A) and ERACoSysMed3 (031L0239).
Competing interests RBS has received lecture fees and advisory board fees from BMS/Pfizer outside this work.
Provenance and peer review Not commissioned; externally peer reviewed.