Article Text

Abstract
Objectives This meta-analysis aims to (1) evaluate the efficacy of physical activity interventions in heart failure and (2) to identify intervention characteristics significantly associated with the interventions’ efficacy.
Methods Randomised controlled trials reporting intervention effects on physical activity in heart failure were combined in a meta-analysis using a random-effect model. Exploratory meta-analysis was performed by specifying the general approach (eg, cardiac rehabilitation), strategies used (eg, action planning), setting (eg, centre based), mode of delivery (eg, face to face or online), facilitator (eg, nurse), contact time and behavioural change theory use as predictors in the random-effect model.
Results Interventions (n=21) had a significant overall effect (SMD=0.54, 95% CI (0.13 to 0.95), p<0.0005). Combining an exercise programme with behavioural change intervention was found efficacious (SMD=1.26, 95% CI (0.26 to 2.26), p<0.05). Centre-based (SMD=0.98, 95% CI (0.35 to 1.62), and group-based (SMD=0.89, 95% CI (0.29 to 1.50),) delivery by a physiotherapist (SMD=0.84, 95% CI (0.03 to 1.65),) were significantly associated with efficacy. The following strategies were identified efficacious: prompts/cues (SMD=3.29, 95% CI (1.97 to 4.62)), credible source (standardised mean difference, SMD=2.08, 95% CI (0.95;3.22)), adding objects to the environment (SMD=1.47, 95% CI (0.41 to 2.53)), generalisation of the target behaviour SMD=1.32, 95% CI (0.22 to 2.41)), monitoring of behaviour by others without feedback (SMD=1.02, 95% CI (0.05 to 1.98)), self-monitoring of outcome(s) of behaviour (SMD=0.79, 95% CI (0.06 to 1.52), graded tasks (SMD=0.73, 95% CI (0.22 to 1.24)), behavioural practice/rehearsal (SMD=0.72, 95% CI (0.26 to 1.18)), action planning (SMD=0.62, 95% CI (0.03 to 1.21)) and goal setting (behaviour) (SMD=0.56, 95% CI (0.03 to 1.08)).
Conclusion The meta-analysis suggests intervention characteristics that may be suitable for promoting physical activity in heart failure. There is moderate evidence in support of an exercise programme combined with a behavioural change intervention delivered by a physiotherapist in a group-based and centre-based settings.
PROSPERO registeration CRD42015015280.
- heart failure
- cardiac rehabilitation
- education
- medical
- telemedicine
- meta-analysis
Data availability statement
All data relevant to the study are included in the article or uploaded as online supplemental information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known about this subject?
Individuals diagnosed with heart failure (HF) are advised to engage in physical activity. However, physical activity levels remain extremely low in this population group. Cardiac rehabilitation (CR) is routinely offered to newly diagnosed HF patients. CR is multifaceted; It is unknown which specific components result in physical activity improvements once the programme has ended. It is essential to understand how best to improve everyday physical activity engagement in HF.
What does this study add?
This meta-analysis assessed what constitutes a successful physical activity intervention designed for individuals living with HF. The findings pinpoint specific intervention features and components that contribute to physical activity improvements in HF. Centre-based interventions that are delivered by a physiotherapist, in group format, which combine exercise with behavioural change intervention are promising for attaining physical activity improvements.
How might this impact on clinical practice?
The findings of this meta-analysis may inform physical activity intervention designed for individuals diagnosed with HF. There is a need for additional training for physiotherapists in delivering behavioural change interventions alongside an exercise programme that includes the identified efficacious strategies.
Introduction
The levels of engagement in physical activity of medically stable individuals diagnosed with heart failure (HF) are low.1 Physical activity is a treatment strategy.2 Cardiac rehabilitation (CR) and other exercise-based programmes have been shown to improve quality of life (QoL)3 4 and reduce hospitalisation in HF.4 5 However, a recent meta-analysis suggested that CR is less likely to be efficacious in sustaining physical activity in HF in particular compared with other cardiovascular diseases (CVD).6 The uptake of CR remains suboptimal.7 Therefore, it is essential to evaluate the efficacy of alternative interventions as well as CR and identify content and features that are likely to be successful in promoting physical activity.
CR is a complex intervention. It is unclear which components are responsible for what outcomes and for which patient group.8 There is a need to explore this intervention complexity and identify what makes an intervention successful.9 Past reviews have suggested that short-term intervention effects are associated with strategies such as exercise prescription; goal setting; feedback and problem solving; and the use of a behavioural change theory.10
CR might be missing some efficacious elements. Clark et al pointed out that previous healthcare services research has not emphasised CR’s goal: how best to ensure that CVD patients benefit from a healthy lifestyle, including physical activity. Clark et al also made a call to evaluate a range of potentially effective interventions that are facilitated by various professionals and make use of a diverse set of methods (eg, remote monitoring). Evaluation of home-based and remote interventions is especially vital, given the recent restriction following the SARS-CoV-2 outbreak. It is also essential to understand what features of centre-based, group-based interventions contribute to physical activity improvement. The present meta-analysis of randomised controlled trials (RCTs) reviewed physical activity interventions, including CR, to identify intervention features that contribute to efficacy in improving physical activity.
Methods
Information sources
The review protocol was registered on PROSPERO database (CRD42015015280). Cochrane Library, MEDLINE, CINAHL, EMBASE, AMED, HEED, PsycArticles, PsycINFO, Global Health, Web of Science: Conference Proceedings, ‘Be Part of Research’ and ClinicalTrials.gov were searched from inception to 20 February 2020. The search strategy is described in online supplemental material 1.
Supplemental material
Eligibility criteria and study selection
Titles, abstracts and full texts were independently screened by two reviewers (AA and PW). The criteria for considering RCTs were: (1) adults diagnosed with HF, (2) intervention targeting physical activity (compared with usual care and/or education), and (3) report of a numerical result for physical activity outcome at intervention completion for both groups. Physical activity outcome was defined as any bodily movement produced by skeletal muscles that requires energy expenditure. Exercise is a subset of physical activity defined as structured physical activity.11 Exercise, in the context of HF, is defined as selfcare behaviour (ie, ‘I exercise regularly’).
Data collection process
Relevant information was extracted from trial reports (article, online supplemental materials and protocols) using a standardised Cochrane data extraction form.12
Risk of bias in individual studies
The risk of bias at the study level was assessed using the Cochrane Collaboration Risk of Bias tool2 13 and informed sensitivity analysis.
Data items
Interventions were classified in terms of their general approach to physical activity promotion (eg, exercise), setting (eg, home vs centre), mode of delivery (eg, group vs individual) and facilitator (eg, nurse). The Theory Coding Scheme (TCS)14 was used to describe the extent to which trials employed a behavioural change theory in the intervention design. TCS scores range from 0 (no theory) to 8 (most extensive theory use). The intervention and comparator treatment were described in terms of the included behavioural change techniques. Interventions’ content was independently annotated by AA (100%) and TF (61.90%) using the Behaviour Change Techniques Taxonomy (BCTTv1).15
Statistical analysis
Meta-analysis was performed using the metafor library in R.16 A random-effect model was used to estimate the overall efficacy of interventions using restricted maximum likelihood. The standardised mean difference (SMD) in physical activity levels between the main intervention and the comparator group was selected as the estimate of efficacy. Heterogeneity index ( ) was reported as the total unexplained variability in effect. Assessments at the 3 months, 6 months (short-term) and 12 months (long-term) follow-up were included. Meta-regression was performed to explore whether the efficacy was associated with the following: general approach (eg, exercise programme), setting, mode of delivery (eg, home-based), facilitator (eg, nurse), behavioural change strategies (eg, goal setting) and participant characteristics (ie, mean age, New York Heart Association (NYHA) class, proportion of males, mean ejection fraction (EF, %), aeschimic aetiology (%)) were specified as predictors in the model.17 We accounted for the fact that a small number of trials were presenting a particular intervention characteristic using Hartung-Knapp-Sidik adjustment as recommended by Debray et al.18
) was reported as the total unexplained variability in effect. Assessments at the 3 months, 6 months (short-term) and 12 months (long-term) follow-up were included. Meta-regression was performed to explore whether the efficacy was associated with the following: general approach (eg, exercise programme), setting, mode of delivery (eg, home-based), facilitator (eg, nurse), behavioural change strategies (eg, goal setting) and participant characteristics (ie, mean age, New York Heart Association (NYHA) class, proportion of males, mean ejection fraction (EF, %), aeschimic aetiology (%)) were specified as predictors in the model.17 We accounted for the fact that a small number of trials were presenting a particular intervention characteristic using Hartung-Knapp-Sidik adjustment as recommended by Debray et al.18
Risk of bias across studies
The small study bias was evaluated using a funnel plot assessment and Egger’s test.
Patient and public involvement
No patients were involved in formulating the research question, the outcome measures or findings interpretation. Patients were not involved in planning or designing of the meta-analysis. This is due to the lack of funding available to include patients as partners in this meta-analysis. Results of this meta-analysis will be disseminated to the relevant patient organisations.
Results
Search results
Search results and reasons for exclusion are listed in the Preferred Reporting Items for Systematic Reviews and Meta-Analyses diagram (figure 1). A total of 20 trials evaluating 22 interventions postcompletion (n=21,19–37), at 6 months (n=5,29 32 33 35 38) and 12 months (n=5,26 27 29 36–38) follow-up were included in the meta-analysis.

The study flow chart (PRISMA, 2009). HF, heart failure; PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Study characteristics
The trials were conducted between 1999 and 2018. The trials included a total of 6277 participants, and the median sample size was 100 (IQR: 60–204). A large proportion (37%) of participants were drawn from the HF-ACTION trial (n=2331).37
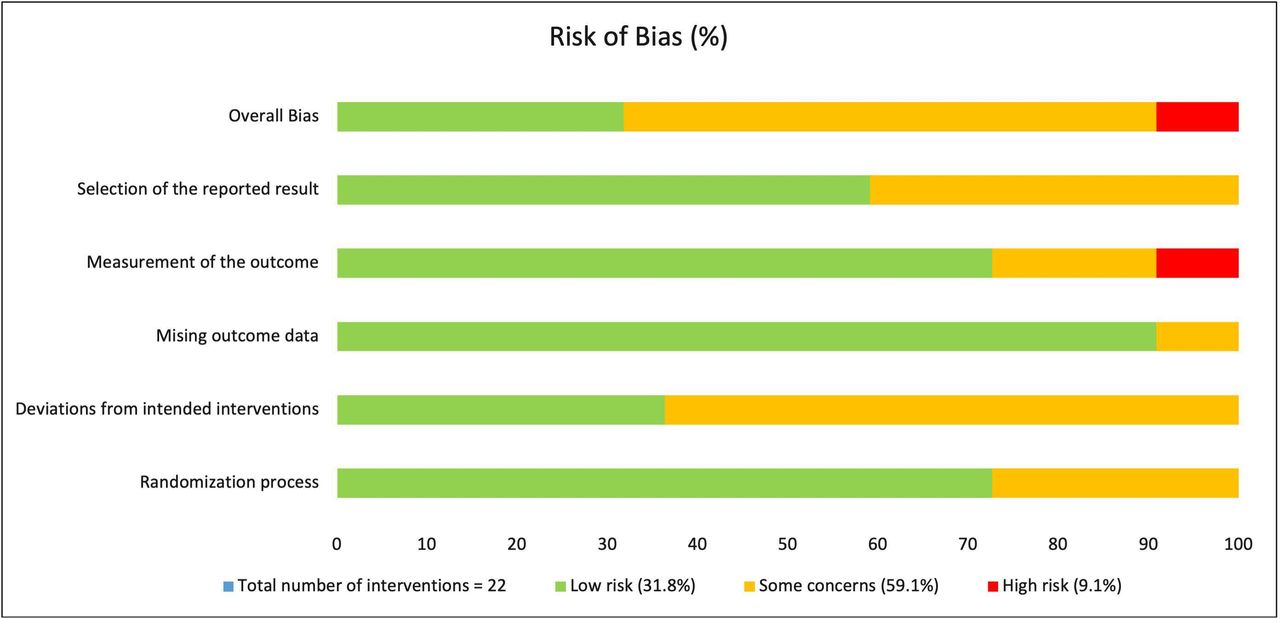
Risk of bias
The overall risk of bias is summarised in figure 2. Six out of 20 trials reported low risk of bias.20 22 26 27 29 37 A high risk of bias was present in two trials.19 30 The sources of bias for each trial are summarised in online supplemental material 2. Five trials evaluated the intervention against an active comparator:education.19 21 22 27 38

The risk of bias summary. The Cochrane Collaboration Risk of Bias tool (V.2).15
Participant characteristics
Mean age ranged from 5419 to 80 years old33 (SD=7.28; IQR 62–70), and the majority of the sample was male 69.49% (table 1).
Study and participant characteristics
Postcompletion efficacy
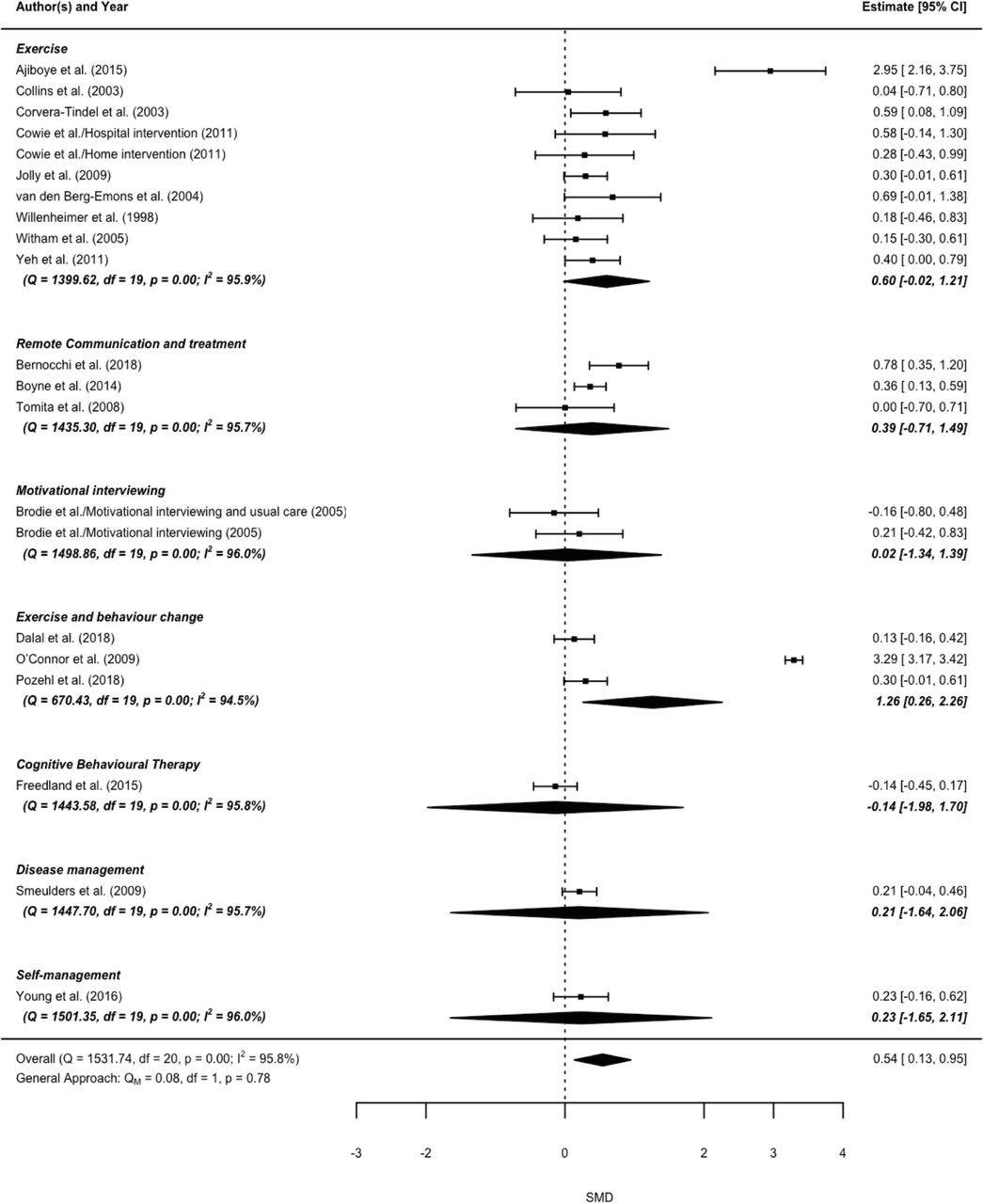
The present meta-analysis found a significant overall effect as assessed at postcompletion (SMD=0.54, 95% CI (0.13 to 0.95), p<0.005). There was significant high heterogeneity in the estimated effect, I2=95.8%, (Q=1531.74, p<0.001) (figure 3). The following intervention characteristics contributed to the heterogeneity in efficacy: general approach of the interventions, setting (ie, centre based vs home based), facilitator and several strategies.

Forest plot illustrating overall estimated effect (SMD) and 95% CI and SMD and 95% CI for component trials. SMD, standardised mean difference.
General approach
The included trials delivered interventions that were classified as exercise (k=10, 47.62%), exercise and behavioural change (k=3, 14.29%), motivational interviewing (k=2, 9.42%), remote communication and treatment (k=3, 14.29%), cognitive–behavioural therapy (k=1, 4.76%), disease management (k=1, 4.76%) and self-management (k=1, 4.76%) (table 2). Exercise combined with behavioural change is an efficacious approach (figure 4).
Intervention characteristics
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Forest plot illustrating the standardised mean differences (SMD, 95% CI) moderated by the general approach.
Intervention strategies
A total of 38 strategies (ie, behaviour change techniques, (BCTs)) were present across included trials (online supplemental material 4). Interventions included a mean of 8.90 (SD=3.77; IQR=8–10) strategies. The following strategies were associated with moderate to large effects: prompts/cues, credible source, adding objects to the environment, generalisation of target behaviour, monitoring of behaviour by others without feedback, self-monitoring of outcome(s) of behaviour, graded tasks, behavioural practice/rehearsal, action planning, goal setting (behaviour) (SMD: 0.56–3.29) (table 3).
Intervention characteristics associated with efficacy
Settings, facilitator and duration
Interventions were delivered at home (n=8, 38%), in a hospital/clinic (n=8, 38%), or both (n=5, 24%). Only centre-based delivery significantly moderated the efficacy of the included interventions (table 3). Interventions were facilitated by general practice nurses (n=9, 42.85%), physiotherapists (n=6, 28.6%), HF nurses (n=4, 19%), exercise instructors (n=3, 14.29%), researchers (n=2, 9.42%), lay leaders (n=1, 4.76%), advanced practice nurse (n=1, 4.76%), psychologists (n=14.76%), and clinical psychology trainees (n=1, 4.76%). Intervention delivery by a physiotherapist was associated with efficacy (table 3). Intervention duration varied from 1 day to 72 weeks. Mean contact time was 1849.38 min (SD=1716.40) and was not associated with intervention efficacy.
Theory use
Seven interventions were based on a behavioural change theory (online supplemental material 4). The extent of theory use (TCS) was not associated with efficacy (SMD=0.13, p=0.059, 95% CI (−0.006 to 0.27)).
Sample characteristics, including mean age, gender, mean left-venticular ejection fraction (LVEF, %), New York Heart Association (NYHA) class, and aetiology, were not significantly associated with intervention efficacy (online supplemental material 5). Likewise, the differences in efficacy between trials using self-reports and trials using accelerometer or pedometer were non-significant (online supplemental material 5).
Long-term efficacy
The included interventions assessed physical activity at a 2-month, 6-month, 12-month and 30-month follow-up. The overall short-term effect was non-significant at the 6 month, (SMD=0.06, 95% CI (−0.49 to 0.38), p=0.80) and 12-month follow-up, (SMD=−0.11, 95% CI (−0.77 to 0.55), p=0.80). Due to the small number of interventions reporting follow-up assessment, it was not feasible to evaluate the long-term effects associated with the individual intervention characteristics.
Sensitivity analysis
Interventions were compared with usual care,20 23–26 28–30 33–37 education delivered by an HF specialist nurse21 22 27 38 or unspecified health professional,19 and discouragement to exercise.32 The comparator treatments included a mean of 1.15 (SD=1.49) strategies (online supplemental material 4). When trials comparing the main intervention to education were excluded, the effects of exercise and behavioural change, remote monitoring and treatment, and exercise were significant (online supplemental material 6). The exclusion of a large (N=2331) trial with a younger (56 years old) sample37 resulted in a significant decrease in the overall effect. The effect estimates for exercise and behavioural change approach, prompts/cues, credible source, adding objects to the environment, generalisation of the target behaviour, monitoring of behaviour by others without feedback, self-monitoring of outcome(s) of behaviour, action planning, and goal setting (behaviour) were sensitive to the inclusion of the trial (online supplemental material 6). The exclusion of interventions with a high risk of bias indicated that the efficacy of Exercise approach was overestimated. The effects of the following strategies were underestimated: social support (emotional), social support (practical), theory use (TCS score), information about health consequences and information on how to perform the behaviour.
Small study bias
A funnel plot for SMD against SE is available in online supplemental material 7. The Egger’s test suggested a lack of publication and small study bias (test for funnel plot asymmetry:  )
)
Discussion
The present meta-analysis found moderate evidence in support of existing physical activity interventions designed for individuals living with HF. Centre-based interventions that are delivered by a physiotherapist, in group format, which combine exercise with behavioural change intervention are promising for attaining physical activity improvements. Intervention strategies identified as efficacious are: prompts/cues, credible source, adding objects to the environment, generalisation of the target behaviour, monitoring of behaviour by others without feedback, self-monitoring of outcome(s) of behaviour, graded tasks, behavioural practice/rehearsal, action planning, and goal setting (behaviour). To our knowledge, this is the first meta-analysis evaluating the components of behavioural interventions that are associated with increased physical activity in HF. Interventions that were delivered by a physiotherapist in a centre-based setting were more promising in attaining physical activity improvement than home-based interventions or those delivered by facilitators other than physiotherapist (ie, nurse, lay leader, researcher). This is in contrast to the findings of a previous meta-analysis suggesting that centre-based and home-based programmes delivered to individuals post-myocardial infarction or revascularisation, and with HF are equivalent in their efficacy in improving survival, QoL and exercise capacity.39 The present meta-analysis found that delivery of an intervention to a group contributed to efficacy. However, given the ongoing pandemic, it is essential to optimise delivery of physical activity interventions in home settings. Group-based interventions contribute to behavioural change via social comparison, changes in normative beliefs about health behaviour and group member identity.40 These factors can also be considered when designing home-based, contact-free physical activity interventions for older adults with HF.
A previous systematic review of CR programmes found that, in general, educational and behavioural elements of CR did not result in physical activity improvements beyond those achieved by exercise-based programmes.6 However, behavioural elements are diverse and vary in their efficacy. The present meta-analysis evaluated a range of such elements and outlined those that are efficacious. A combination of an exercise and behavioural change approach was found to be more efficacious than other approaches, including exercise alone. Several strategies to improve physical activity appear promising (table 3). Theoretical explanations for the efficacy of these strategies were previously offered.41 Graded tasks exert an effect on physical activity by fostering positive beliefs about capability through skill mastery (eg, exercise training).41 Self-monitoring, monitoring by others, planning, goal-setting and feedback are theorised to improve control and regulation of behaviour.42 Finally, the efficacy of adding an object associated with physical activity (eg, treadmill) indicates the relevance of cueing (ie, automatic association and non-deliberate regulation of behaviour).41
Implications for clinical practice and future research
The present meta-analysis found moderate evidence in support of combining exercise programme with behavioural change intervention, delivered by a physiotherapist. Thus, there is a need for additional training for physiotherapists in delivering behavioural change interventions that will include the identified efficacious strategies. Practical limitations of the identified efficacious strategy need to be considered when designing interventions. Adding objects to the environment to support physically activity lifestyle (eg, a treadmill) may not be affordable or practical, and does not satisfy the principle of health equity.43 In addition, further research investigating how best to promote a physically active lifestyle in the older HF population is encouraged. The clinical profiles of older adults differ from younger adults, with a significantly worse prognosis and a larger number of comorbidities in the former.44 Older adults may also differ in their beliefs about physical activity; and strategies that are suited for promoting an active lifestyle in older adults are different to those that are efficacious for the general population.45 Investigation of which behavioural change theory should form the basis for an intervention is also warranted. Only five trials assessed physical activity at 6-month and 12-month follow-ups. Long-term efficacy was not supported. Thus, it is important to investigate how sustained physical activity improvements can be established.
Study-level limitations
High risk of bias was observed in two trials.21 32 The sensitivity analysis indicated that the inclusion of these trials may overestimate the efficacy of exercise programmes and underestimate the efficacy of remote monitoring and treatment. Remote communication and feedback interventions that include strategies such as biological feedback (eg, symptom monitoring and feedback) delivered by a nurse using telehealth device, as well as self-monitoring of the behaviour and information about health consequences22 23 are identified as efficacious when high risk of bias trials are excluded. The HF-ACTION37 trial constituted the majority of the meta-analysis sample and when it was excluded in the sensitivity analysis, only a small non-significant effect of exercise combined with behavioural change was observed. High-quality trials assessing the short and long-term effects of behavioural change; remote communication and treatment; and exercise programmes on physical activity in older adults (>70 years old) with HF are required.
Strengths and limitations of the review
A Cochrane overview of reviews recommended exploring intervention complexity using meta-regression to evaluate the association between intervention characteristics and efficacy.9 This meta-analysis identified, annotated and classified behavioural change interventions in terms of their general approach, strategies, settings, facilitator, delivery mode, duration and use of theory; and using meta-regression assessed the association between these characteristics and the efficacy. The clear, consistent and systematic description of the interventions facilitated the reliable grouping and analysis. This helped pinpoint specific efficacious features and elements that can be applied, either as part of CR or otherwise, to improve physical activity outcomes in HF. However, there are a few limitations. Intervention features were present in clusters across the included trials. Given the small number of RCTs evaluating any single included characteristic, multiple comparisons were not feasible. It is not possible to ascertain whether each of the evaluated features is efficacious on their own or only in combination. These features need to be evaluated in a multiarm trial comparing their effects.
Conclusions
This meta-analysis explored intervention complexity and identified some features of potentially promising physical activity interventions designed for people living with HF. The present review provides moderate evidence that an exercise programme combined with a behavioural change intervention is a promising approach to increasing physical activity in HF. The meta-analysis suggests behavioural change strategies that may be useful in promoting physical activity in HF.
Data availability statement
All data relevant to the study are included in the article or uploaded as online supplemental information.
Ethics statements
Acknowledgments
We would like to thank the authors of the included studies for providing the information required for the detailed description of the interventions and data analysis. Many thanks to Professor Gary Morgan at City, the University of London, for his support throughout the review. We thank Dr Raisa Jessica Aquino for her comments on the earlier version of data extraction (excluded at the later stage of the review). We also thank Dr Michael J. Shoemaker (Grand Valley State University) for sharing details on one of the pilot studies he and his colleagues carried out (excluded at the later stage of the review).
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @tzellofouska
Contributors All authors contributed to design and planning. AA and PW contributed by screening articles for inclusion. AA and TF contributed to data extraction and risk of bias assessment. AA implemented the analysis. AA, TF and MH contributed to reporting. TF and MH contributed to the critical revision of the manuscript.
Funding Funding The review was supported by a City, University of London Postgraduate Studentship Grant.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.