Article Text

Abstract
Objective We surveyed UK practice of National Institute for Health and Care Excellence (NICE) “Recent onset chest pain” guidance (CG95, 2016), stratified by sex. We looked for sex-related differences in referral to computed tomographic coronary angiography (CTCA) and subsequent functional imaging (FI), invasive coronary angiography (ICA) and revascularisation.
Methods This was a prospective analysis of CTCA practice in 8 UK centres between 2018 and 2020. Coronary artery disease (CAD) was recorded with the CAD-reporting and data system. Local electronic records/archiving/communication systems were used to collect data regarding subsequent FI, ICA and revascularisation.
Results 2301 women, 2326 men underwent CTCA; women were older (58±11 vs 55±12 years, p<0.001) but more likely to have normal coronary arteries (46% (1047) vs 29% (685); p<0.001) and less likely to have severe stenosis (7% (169) vs 13% (307); p<0.001). FI was used less for 4% (93) women, 5% (108) men; ICA was also used less for women (8% (182) vs 14% (321)), as was revascularisation (4% (83) vs 8% (177), p<0.001 for all), including those with ≥moderate CTCA stenosis undergoing ICA (53% (79) vs 61% (166); p<0.001).
Conclusions Women referred for a NICE CG95 (2016) CTCA are more likely to have normal coronary arteries and men more likely to have CAD. More men than women will then undergo ICA and revascularisation even after adjustments for CTCA disease severity. Raised awareness of these inequalities may improve contemporary chest pain care.
- computed tomography angiography
- chest pain
- quality of health care
Data availability statement
Deidentified participant data are available on reasonable request from ORCID iD 000-0001-8568-6440.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known about this subject?
The 2016 iteration of the National Institute for Health and Care Excellence (NICE) guidance for the assessment and diagnosis of recent-onset stable chest pain of suspected cardiac origin (Clinical Guideline 95 (CG95 2016)) is clear in its recommendations regarding computed tomographic coronary angiography (CTCA) as a first-line investigation and when, and how, to do onward cardiac investigations. Post hoc analysis of the ‘test and treat’ research studies evaluating CTCA and non-invasive cardiac imaging predominantly for patients with stable chest pain have given evidence of a disproportionate number of women with normal coronary arteries but also a tendency to offer more men than women invasive testing and subsequent revascularisation.
What is not known is whether these sex-related differences exist in the contemporary hospital clinical management of stable chest pain and whether NICE CG 95 (2016) may have had a beneficial effect on the subsequent use of cardiac tests and revascularisation.
What does this study add?
In routine clinical use CTCA, for recent-onset chest pain assessment, has been shown to be a robust test, undertaken with sex equality. However, more women have normal coronary arteries and more men have atheroma, whether ischaemia is inferred or not, suggesting that NICE CG 95 (2016) is not being implemented in a sex-equivalent fashion. Subsequent to CTCA, more men are offered invasive coronary angiography (ICA) and revascularisation. These differences favouring more invasive investigation and treatment for men persist when comparisons are made for patients with comparable CT angiographic disease. Furthermore, for patients undergoing ICA, having had a CTCA finding of atheroma possibly or probably associated with ischaemia, women are less likely to undergo revascularisation.
How might this impact on clinical practice?
The difference in the rate of normal coronary arteries between the sexes suggests we are testing too few men, or less likely, too many women. Once we have found potentially obstructive disease with CTCA then equivalent care between the sexes might be expected. Unfortunately despite the advent of first line anatomical testing with CTCA for stable chest pain there are stark differences between how ICA and revascularisation are used, between the sexes. Increased awareness and focus on these factors by cardiologists across the UK may help to level off this currently uneven playing field.
Introduction
Traditionally, in the management of suspected stable angina, women are less likely than men to be referred for cardiac investigations or undergo coronary revascularisation.1 More recently, the major ‘test and treat’ studies for the evaluation of stable chest pain comparing computed tomographic coronary angiography (CTCA) to functional cardiac imaging or standard care have undergone post hoc analysis stratified by sex, which have revealed interesting disparities.2 3 Obstructive coronary artery disease is less common in the women enrolled into these research studies, compared with the men. However, CTCA is also advocated as providing as much, or possibly more, benefit to women as compared with men in terms of offering accurate diagnosis and subsequent treatment.2 3
The 2016 iteration of the National Institute for Health and Care Excellence (NICE) guidance for the assessment and diagnosis of recent-onset chest pain of suspected cardiac origin (Clinical Guideline 95 (CG95)) recommends diagnostic testing when stable angina cannot be excluded by clinical assessment alone.4 The first-line diagnostic test suggested is CTCA. The guideline then recommends additional diagnostic investigation which may be needed following a CTCA, when evidence of coronary artery disease of uncertain functional significance is found or the scan is non-diagnostic. Through collaboration with the British Society of Cardiovascular Imaging/British Society of Cardiovascular Computed Tomography (BSCI/BSCCT), we studied 5293 patients across the UK referred for CTCA, following recent-onset chest pain assessment, according to NICE CG95 (2016) as a service improvement initiative.5 We reported the disease distribution and down-stream testing provided for these patients, of whom 50% were female. Although there has been recent publication on the ‘changing landscape of non-invasive cardiac testing’ in the UK, no clinical sex-related data have been presented.6
It is possible that the previously described sex-based disparities in the cardiac investigation and revascularisation rates of patients with stable chest pain may have been modified by the advent of first-line testing with CTCA. Therefore, we investigated this using ‘real world’ data. We hypothesised that CTCA, by offering a more accurate delineation of the extent of any CAD present, may lead to rates of invasive coronary angiography (ICA) and revascularisation that are similar between the sexes for patients with equivalent disease.
Methods
Study design
This is a multicentre, prospective analysis of the onward investigation and treatment of patients with suspected stable coronary artery disease. Centres across the UK undertaking CTCA in accordance with NICE CG95 (2016) were offered the opportunity to collect prospective data on patients attending for CTCA through email communication from the BSCI/BSCCT. It was a requirement that centres had access to information on subsequent activity for patients. The study was registered as a national audit and service evaluation in Plymouth (National audit of downstream testing after CTCA following NICE CG95 (2016) reference: CA_2017-18-191). Centres agreeing to collect data registered with their local audit departments. Written informed consent and ethical approval was not obtained as patient care was not affected. Only fully anonymised data were transferred and used in analysis.
Data collection
Each site was required to make two data collections: baseline data and follow-up data, within 12 months. Baseline data were collected for consecutive patients, fulfilling NICE CG95 (2016) referral criteria at the time of the CTCA, by 10 centres across the UK between January 2018 and March 2019. Local electronic patient records and picture archiving and communication systems (PACS) were then used to collect follow-up data, which was completed by March 2020.
The first data collection covered demographic information and CTCA results. Demographic information included age, sex and body mass index (BMI). The reporting cardiologist or radiologist decided whether the CTCA was diagnostic or not, primarily based on their own criteria. For all diagnostic CTCA, the Coronary Artery Disease–Reporting and Data Systems (CAD-RADS) score was provided (CAD-RADS 0=0% coronary stenosis; CAD-RADS 1=1% to 24%; CAD-RADS 2=25% to 49%; CAD-RADS 3=50% to 69%; CAD-RADS 4=70% to 99%; CAD-RADS 5=100% or coronary occlusion), with the most severe stenosis defining the patient’s score.7 The ability to provide a CAD-RADS score was recommended to reporting centres as a secondary method of defining a diagnostic CTCA. The CAD-RADS score was then categorised into three groups: CAD-RADS 0, normal coronary arteries (NCA); CAD-RADS 1–2, atheroma probably not associated with ischaemia; CAD-RADS 3–5, atheroma possibly or probably associated with ischaemia.
The second data collection pertained to the completion of the patient’s diagnostic pathway. Once a decision regarding onward investigation or treatment after CTCA had been made, and any functional testing for ischaemia (FI), ICA or revascularisation by means of percutaneous intervention (PCI) or coronary artery bypass surgery (CABG) had been carried out, then the data collection was complete. If FI was carried out to facilitate the decision-making process regarding the need for ICA, then this was recorded. If patients presented urgently or emergently while planned investigations were pending, and underwent further investigation or treatment, then these data were included in the analysis. Data collection did not allow for re-presentation or re-investigation of stable chest pain symptoms.
All data were then anonymised at the collecting site and collated in Plymouth as the registered national audit centre. One centre submitted uninterpretable data and was excluded from the analysis. One further centre did not submit demographic data, leaving eight centres contributing to this analysis. Once collated, the data were split by sex. The analysis then focused on the distribution of CAD, the subsequent use of FI, ICA, and revascularisation, stratified by sex.
Statistical analysis
Results data are referred to as female for the population of women or male for the population of men. Patient age and BMI are provided as mean±SD; ranges are given in table 1. Ordinal categorical variables (CAD-RADS scores) are presented as a percentage (number of patients) and graphically displayed in bar charts. Statistical analysis was completed using Statistical Package for Social Sciences software statistics V.23 (SPSS, Chicago, Illinois, USA). Age and BMI were compared between males and females by sex using the Wilcoxon rank sum test. Categorical variables were compared by sex using χ2 testing. A similar approach was used to assess the use of FI, ICA and revascularisation across the whole female and male populations and where appropriate for those with atheroma possibly or probably associated with ischaemia, a non-diagnostic CTCA or those undergoing ICA. A two-tailed p value of<0.05 was taken as statistically significant.
Patient numbers and characteristics, by sex
Results
Patient population
The total population contained data from 4627 patients, having removed 666 patients with no demographic data submitted in the previously described service improvement initiative.5 Patients had a mean age of 57±12 years, mean BMI 29±6 kg/m²; 50% (2301) were female and 50% (2326) male. The females were older than the males (58±11 years vs 55±12 years, p<0.001) but had a lower body mass index (28.7±6 kg/m² vs male 29.0±5 kg/m², p<0.001; table 1).
Disease distribution
Overall, 96% (4446) of CTCA were of diagnostic image quality. The male diagnostic scan rate of 97% (2248) was higher than the female diagnostic scan rate of 96% (2198; p<0.001).
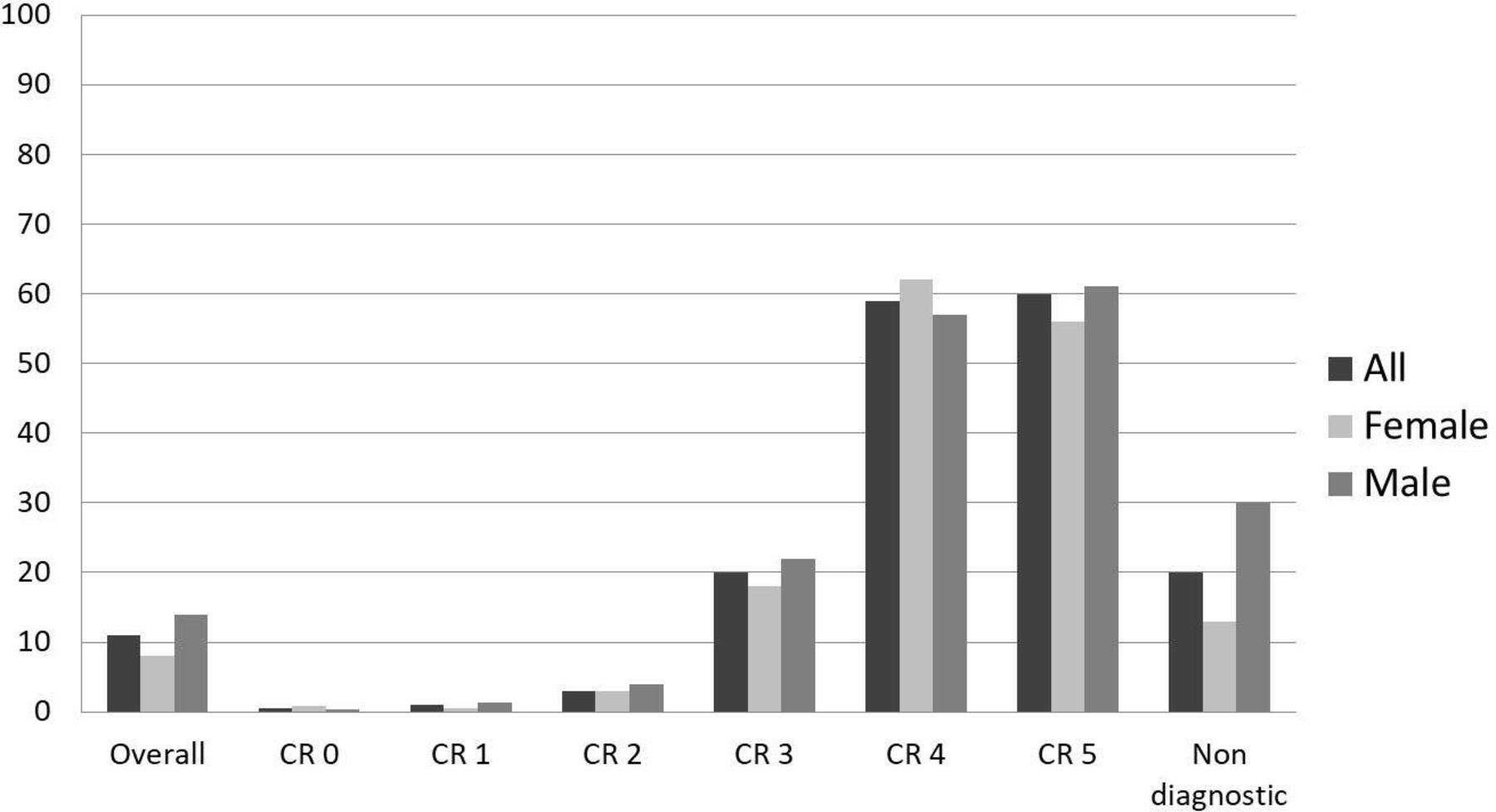
The total and sex-stratified CAD-RADS distributions are given in figure 1. Women were more likely to have normal coronary arteries (CAD-RADS 0) compared with men (46%, n=1047/2301 vs 29% n=685/2326; p<0.001). Furthermore, 7% (169) females had CAD-RADS 4 in comparison with 13% (307) of males (p<0.001). When collated, 17% (n=385) of females had atheroma possibly or probably associated with ischaemia as opposed to 28% (n=647) of males (p<0.001). For atheroma probably not associated with ischaemia, the rates were 33% (n=766) for females and 39% (n=916) for males (p<0.001). Men were therefore more likely to have atheroma, whether ischaemia was inferred or not (table 2).

Distribution of CAD-RADS categories identified on CCTA following NICE CG 95 (2016), stratified by sex: 4627 patients, 2301 women, 2326 men. CAD-RADS (abbreviated to CR), Coronary Artery Disease–Reporting and Data System; CTCA, computed tomographic coronary angiography; NICE CG 95 (2016), National Institute of Clinical Excellence clinical guideline 95, 2016 iteration.
Number (%) of non-diagnostic CTCA, CAD-RADS 0, 1–2 and 3–5 patients, by sex
Functional imaging
Overall, FI was used more frequently in males (5%, n=108) than females (4%, n=93; p<0.001). However, when atheroma possibly or probably associated with ischaemia was identified on CCTA, there was more frequent use of FI in females at 14% (n=55/385) versus males at 11% (n=72/647, p<0.001; table 3). The full FI data stratified by CAD-RADS score and sex are shown in figure 2.
Functional imaging, ICA and revascularisation rates after all CTCA, by sex

Use of functional imaging after CTCA, stratified by CAD-RADS group and sex. CR or CAD-RADS, Coronary Artery Disease–Reporting and Data System; CTCA, computed tomographic coronary angiography. Functional imaging was generally used more for males although for those with atheroma possibly or probably associated with ischaemia (CAD-RADS 3-5), this trend was reversed.
ICA and revascularisation
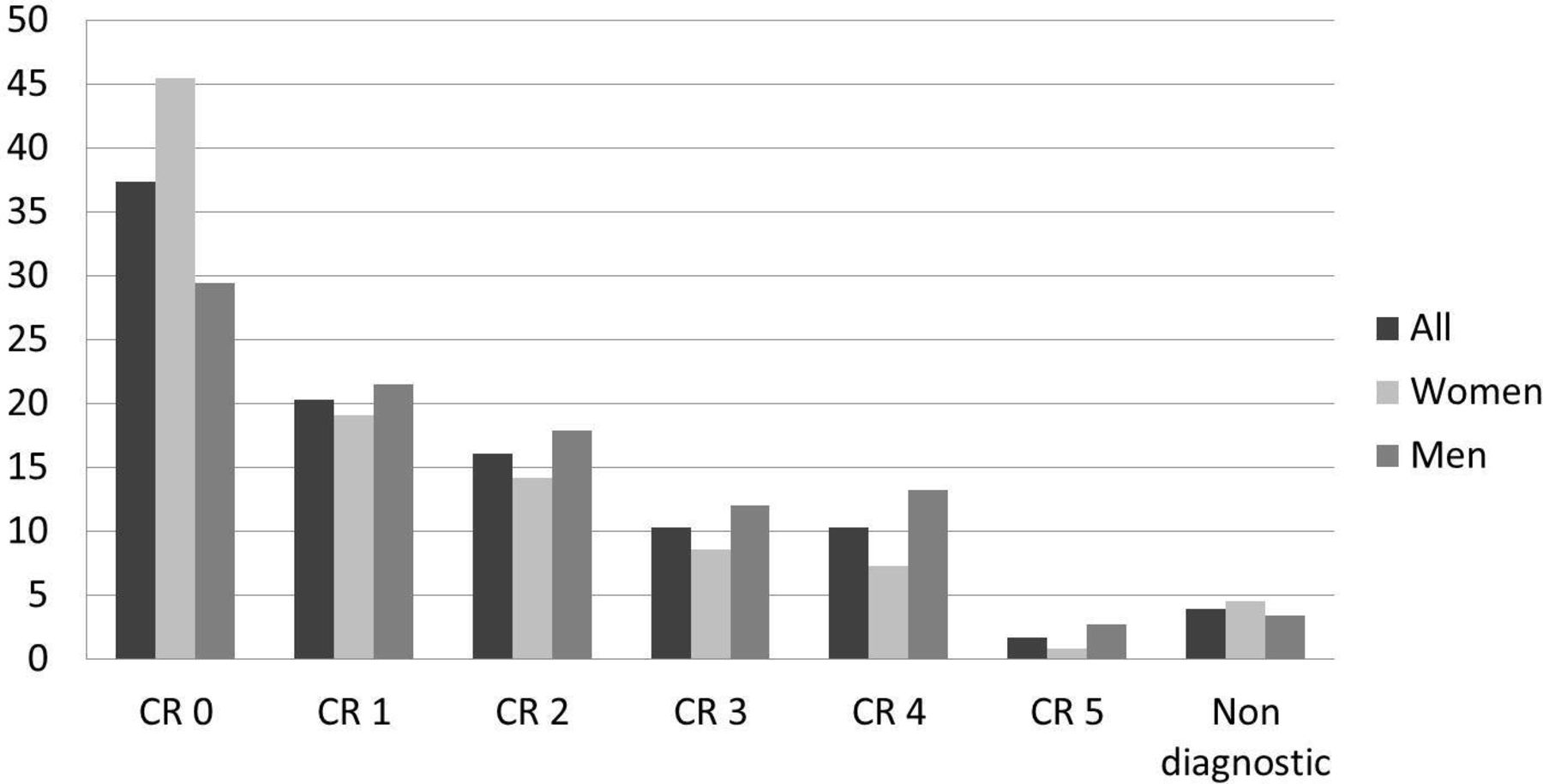
The rate of ICA following CTCA was higher for males at 14% (n=321) than females at 8% (n=182, p<0.001; table 3). The full ICA data stratified by CAD-RADS score and sex are shown in figure 3. When atheroma possibly or probably associated with ischaemia was identified on CCTA, the ICA rate remained lower for females at 39% (n=149/385) than for males at 42% (n=274/647, p<0.001). Males were also more likely to have a non-diagnostic CTCA followed by ICA than females (29%, n=23/78 vs 13%, n=13/103, p<0.001; figure 4).
ICA rates after CTCA, stratified by CAD-RADS score and sex. CR or CAD-RADS, Coronary Artery Disease–Reporting and Data System; CTCA, computed tomographic coronary angiography; ICA, invasive coronary angiography. Males were more likely to undergo ICA after CTCA than females.

ICA rates for various CTCA findings: normal coronary arteries, atheroma probably not associated with ischaemia, atheroma possibly or probably associated with ischaemia and non-diagnostic, by sex. APNI (CAD-RADS 1–2), those with atheroma probably not associated with ischaemia; APPI (CAD-RADS 3–5), those with atheroma possibly or probably associated with ischaemia; CAD-RADS, Coronary Artery Disease–Reporting and Data System; CTCA, computed tomographic coronary angiography; ICA, invasive coronary angiography; NCA (CAD-RADS 0), normal coronary arteries. Males were more likely to undergo ICA than females, adjusted for degree of CAD.
Similarly, the use of revascularisation was generally higher for males at 8% (n=177) compared with females at 4% (n=83, p<0.001; table 3). The full revascularisation data stratified by CAD-RADS score and sex are shown in figure 5. Men were more likely to undergo revascularisation than women when the CTCA was non-diagnostic (12%, n=9/78 vs 4%, n=4/104, p<0.001) and when atheroma possibly or probably associated with ischaemia was identified (26%, n=166 vs 21%, n=79, p<0.001).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Revascularisation rates after CTCA, stratified by CAD-RADS score and sex. CR or CAD-RADS, Coronary Artery Disease–Reporting and Data System; CTCA, computed tomographic coronary angiography. Males were more likely to undergo revascularisation than females.
Discussion
We have shown that despite previous studies establishing sex-based differences in the care of patients with stable chest pain, these still persist in contemporary UK clinical practice and have not been improved by the implementation of NICE CG 95 (2016). One of the major predictors of a CTCA result is the patient’s sex. If the CTCA is abnormal, cardiologists are more likely to proceed to ICA for a man and functional imaging for a woman. For patients undergoing ICA, as a follow-on from CTCA, men are more likely to receive revascularisation.
In the post hoc analysis of the Scottish CT of the Heart (SCOT-HEART) trial, 50% of women and 26% of men had normal coronary arteries at CTCA. Similarly, 41% of women and 25% of men in the CT arm of the post hoc analysis of the Prospective Multicentre Imaging Study for Evaluation of Chest Pain (PROMISE) had normal coronary arteries.2 3 In this paper, we have shown that these findings are consistent with ‘real world’ UK patients with chest pain who are referred for CTCA, with normal coronary arteries occurring in 46% of women and 29% of men. Consistent with the previous studies, atheroma probably not associated with ischaemia, and atheroma possibly or probably associated with ischaemia, are more frequent findings on CCTA in men (39% and 28%, respectively) than women (33% and 17%, respectively). Also as previously described, the women being investigated for suspected coronary artery disease are older than the men, although the men had a higher BMI.2
Traditionally, the higher use of ICA in men following non-invasive cardiac testing may have been attributed to a tendency for cardiologists to dismiss positive FI tests in women as ‘false positive’. One hope therefore was that this would end with the use of CTCA as the primary diagnostic tool, given its more accurate delineation of the extent and severity of CAD. However, we have demonstrated that using CTCA as the primary diagnostic tool for stable chest pain investigation does not lead to equivalent delivery of either ICA or revascularisation, between the sexes. This applies even when grouped by the extent of the disease. A man with a CTCA reporting CAD-RADS 3 to 5 is more likely to undergo ICA and more likely to be treated with revascularisation than a woman with the same category of CTCA stenosis. There is also a potentially concerning difference with the data presented in the post hoc analysis of the PROMISE trial, in which, once ICA was undertaken, the revascularisation rates equalised between the sexes.2 We have been unable to show this, even when only patients with atheroma possibly or probably associated with ischaemia undergoing ICA are considered.
The reasons for our findings are likely to be multifactorial. It is of interest that cardiologists appear more willing to use FI for women when atheroma possibly or probably associated with ischaemia is found, but not invasive investigation or revascularisation. It is possible we have a conditioned response, or implicit bias, to investigate men with chest pain more invasively, possibly even taking the presentation more seriously. Maybe we are asking a lot of a non-invasive imaging test to ‘iron-out’ the differences between how the sexes are managed.
The vast majority of women required no further investigation after CCTA, with 46% having normal coronary arteries and 33% having ≤mild stenosis (CAD-RADS 1 or 2). In the report of the BSCI/BSCCT national audit of downstream testing after a NICE CG95 (2016) CTCA, overuse of ICA was suggested, and the low rate of revascularisation for patients with a moderate stenosis (CAD-RADS 3) was given as a reason to reconsider the need for ‘blanket’ FI in such patients.5 A trend towards less FI may of course be a direct and appropriate consequence of the Ischemia Research Group’s findings.8 However, given the sex-related distribution of CAD demonstrated here, maybe we need to consider if we are putting either too many women, or more likely not enough men, forward for stable chest pain assessment with CTCA in the first place. Neither should we forget the female-specific pathophysiological effects of CAD or the need to pursue aggressive preventative strategies for those women with coronary artery atheroma.9
It may be a disappointment to those involved in cardiac CT services across the UK to see the lack of effect the first-line anatomical approach of NICE CG95 (2016) has had on the sex-related differences in the use of subsequent ICA and revascularisation. It throws up a second challenge to interventional cardiologists. The first challenge is to avoid overuse of ICA or ICA that has little chance of resulting in revascularisation; the second is to simultaneously offer ICA, and indeed revascularisation, in a sex-proportionate and balanced fashion.
Strengths and limitations
Our study provides extensive data, novel in ‘real world’ terms, regarding the contemporary investigation of men and women having stable chest pain investigation. A major strength of this work is the prospective, multicentre design and large number of patients. Furthermore, the data presented are in some ways remarkably consistent with that seen in the carefully constructed and conducted randomised control trials.
There are of course limitations to a service improvement initiative or audit, which involves collection of data in an observational manner. There may be unadjusted confounding factors and referral bias. Every effort has been taken to ensure data collection was accurate and complete, including ensuring that data analysis was re-assessed by each contributing centre to ensure accuracy. However, as with all analyses involving healthcare records, these may be incomplete, inaccurate or unclear. Two centres failed to provide appropriate information and have been excluded from this analysis. Other centres successfully clarified any unclear or incomplete data entries. Furthermore, no information is available for other potentially clinically relevant covariates and therefore no logistic regression modelling to adjust for association between sex and referral for onward testing was possible.
Conclusions
Although CCTA is used in an equal manner for women and men being assessed for stable chest pain, there are sex-based differences in subsequent management. Women are more likely to have normal coronary arteries and men were more likely to have CAD of all severities; we may therefore be under-investigating chest pain in men. Women with abnormal CCTA were more likely to undergo FI than men, whereas men are more likely to undergo ICA and revascularisation. This difference persists when only patients with atheroma possibly or probably associated with ischaemia are considered and we may therefore be missing an opportunity to offer women appropriate revascularisation. We need to raise awareness of this among cardiologists and improve the way in which we offer ICA, and revascularisation, after CTCA while simultaneously ensuring we avoid ICA overuse.
Data availability statement
Deidentified participant data are available on reasonable request from ORCID iD 000-0001-8568-6440.
Ethics statements
Acknowledgments
We thank all the staff who supported this study including Sylvie Dubois-Marshall, NHS Grampian, Aberdeen, UK; Sze Mun Mak, Guy’s and St Thomas’ NHS Foundation Trust, London, UK; and Peter Brown, Sheffield Teaching Hospitals NHS Trust, Sheffield, UK.
Footnotes
Twitter @imagingmedsci
Correction notice Since the publication of this article, Matthias Schmitt has now been added as a co-author.
Contributors GM-H planned and developed the study with help from MCW. The British Society of Cardiac Imaging/British Society of Cardiovascular Computed Tomography supported the study through access to societal membership. GM-H, ML, CAR, AV, FW and SI helped conduct and report the study. GM-H, MCW, CAR, RB and ML contributed significantly to manuscript drafting. All authors reviewed and approved the manuscript and have contributed significantly to the work. GM-H is responsible for the overall content as guarantor.
Funding MCW is supported by the British Heart Foundation (FS/ICRF/20/26002).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.