Article Text

Statistics from Altmetric.com
COVID-19 swept the world by surprise after December 2019. Its human, psychosocial and economical toll has been high, while the emergence of variants from the UK, South Africa and Brazil has delayed our hope for an early end to this pandemic through widespread vaccination. Patients with congenital heart disease (CHD) were considered to be particularly vulnerable to infection due to the cardiovascular and systemic sequelae of their underlying complex conditions and fragile pathophysiology, as well as the higher morbidity and mortality seen in non-CHD patients with cardiovascular disease.1 The European Society of Cardiology Working Group of Adult Congenital Heart Disease (ACHD) and the International Society for Adult Congenital Heart Disease published an early position statement that recommended risk stratifying ACHD patients using a combination of underlying anatomy and current physiology.2
In this issue of Open Heart, Ruperti-Repilado et al surveyed 24 ACHD experts at 23 European centres to determine their perceived risk factors for adverse outcomes after COVID-19 infection, prior to available real-world data and in comparison to risk factors highlighted by the European Society of Cardiology and International Society for Adult Congenital Heart Disease position paper.3 Participants selected general and ACHD-specific risk factors for poor outcomes and estimated the overall risk for each of seven case scenarios. This study was part of the European collaboration for Prospective Outcome research in Congenital Heart disease (EPOCH), which recently published their results on the independent predictors of death or severe COVID-19 infection in CHD patients.4
Importantly but unsurprisingly, most clinicians (82%) felt that ACHD patients were not equally at risk. This likely reflects the variability that exists in patients’ anatomy and residual sequelae, partly as a consequence of the decades of increasing surgical and interventional expertise. More than 90% of experts felt that pulmonary arterial hypertension, cyanotic heart disease and Fontan palliation were the most important risk factors for adverse outcomes after COVID-19 infection. Systolic dysfunction of the subaortic or subpulmonary ventricle was felt to be important by more than 80% and 65% of experts, respectively. Thirty-three percent of experts considered anatomical complexity as the most important risk factor, though they all appear to have incorporated this into their assessment of the seven case vignettes presented by Ruperti-Repilado et al. Together, these vignettes present an interesting cross-section of the prevalent issues facing our current ACHD patient cohort as well as the important risk factors for death or severe infection that were identified in non-CHD patients. There was remarkable variability in the risk estimated by experts across scenarios: most rated at very high risk the Down syndrome patient with Eisenmenger physiology, moderate to high risk the patient with an extracardiac Fontan and low risk the patient with previously repaired ventricular septal defect, left ventricular non-compaction and left ventricular ejection fraction of 50%. The remaining patients were rated at low to moderate risk.
Overall, only 1/3 of experts (29%) identified comorbidities as important. Of these, almost all clinicians (90%–100%) agreed that patient-specific risk factors such as age, symptomatic heart failure, immunosuppression, advanced lung disease, advanced renal disease and diabetes were important. Approximately 2/3 of experts felt that male gender or arterial hypertension were important, while 1/3 felt that a genetic syndrome (Down or 22q11 deletion syndrome) was important. This contrasts with these patients’ immune dysfunction and Down syndrome patients’ greater vulnerability to respiratory infections.
How does this compare with real-world experience?
Lewis et al were the first to publish their assessment of risk factors for death or hospitalisation after COVID-19 infection from their single-centre experience of 53 adults and children with CHD.5 Second, Schwerzmann et al published their results of 105 adults with CHD and COVID-19 infection as part of the EPOCH.4 Most recently, Broberg et al published the results of their retrospective study of 1044 adults with CHD and COVID-19 infection across 58 international centres.6 The authors aimed to determine the independent predictors of death (primary outcome) or severe infection (secondary outcome), which they defined as acute respiratory distress syndrome or the need for intensive care unit admission, invasive ventilation (intubation) or renal replacement therapy. All three studies included patients with biochemically confirmed infection or suspected infection based on clinical symptoms and circumstances. Importantly, there appears to be only minor overlap between study cohorts.4–6
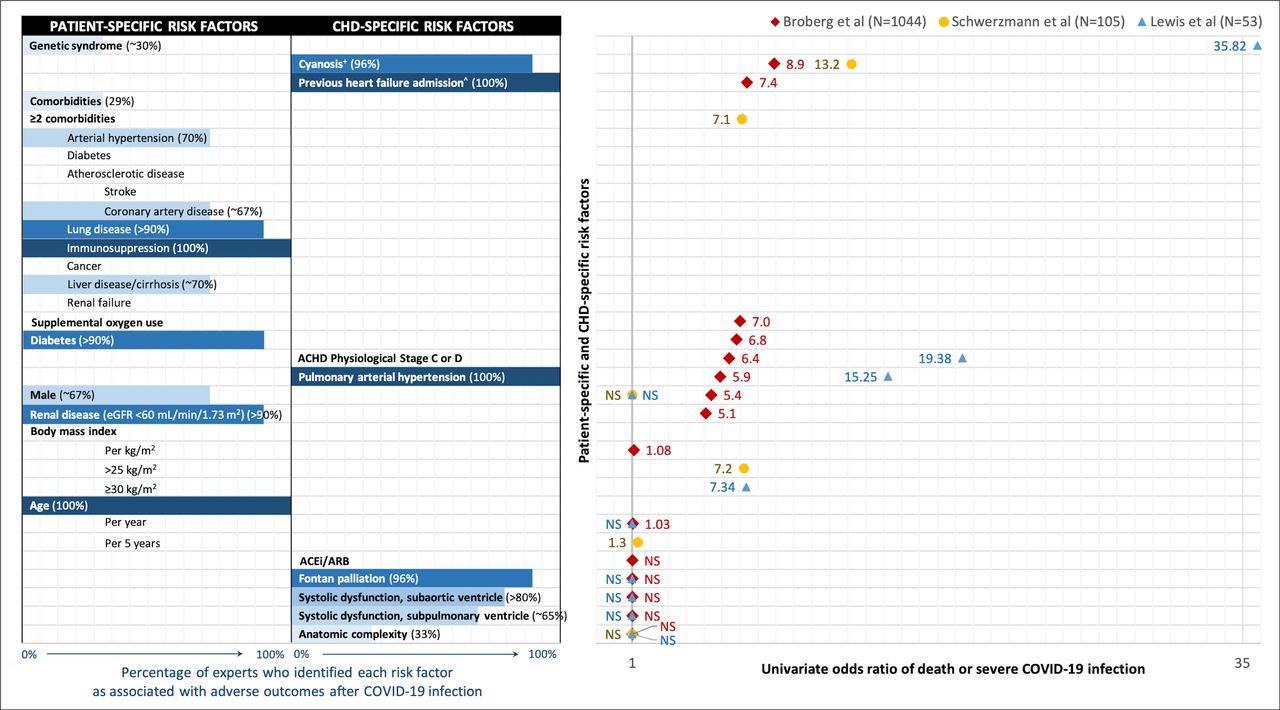
Overall, ACHD experts underestimated the importance of patient-specific risk factors such as body mass index, male sex and genetic syndrome (figure 1). They overestimated the importance of CHD-specific risk factors such as anatomical complexity and Fontan palliation, but correctly identified the importance of cyanosis, pulmonary arterial hypertension (or Eisenmenger syndrome) and clinical heart failure.
{kind=link}
Comparison of expert opinion vs real-world data on independent predictors of death or severe COVID-19 infection in ACHD patients. Patient-specific and CHD-specific risk factors assessed by Ruperti-Repilado et al, Broberg et al, Schwerzmann et al and Lewis et al are presented in two columns on the left. Blue horizontal bars indicate the percentage (%) of surveyed experts who perceived each risk factor to be associated with adverse outcomes after COVID-19 infection.3 Risk factors are listed by decreasing magnitude of OR from univariate analysis from Broberg et al (red diamond), Schwerzmann et al (yellow circle) and Lewis et al (blue triangle). ORs are plotted on the right from 1 (not statistically significant, NS) to 36. Overall, ACHD experts underestimated the importance of patient-specific risk factors, particularly that of body mass index, male sex and genetic syndrome. They overestimated the importance of CHD-specific risk factors such as anatomical complexity and Fontan palliation, and correctly identified the importance of cyanosis, pulmonary arterial hypertension or Eisenmenger syndrome and clinical heart failure. ACE inhibitor (ACEi) or angiotensin receptor blocker (ARB) use were not associated with adverse outcomes after COVID-19 infection. ˆIncluded as ‘symptomatic heart failure’ in Ruperti-Repilado et al’s survey. +Defined as: oxygen saturation<90% in Broberg et al; cyanotic heart disease or Eisenmenger syndrome in Schwerzmann et al. ACHD, adults with congenital heart disease. CHD, congenital heart disease.
That anatomical complexity does not predict adverse outcomes after COVID-19 infection is a major discovery from real-world data.4–6 This makes sense in context. Markers of current physiology or cardiac sequelae such as previous heart failure admission, cyanosis, Eisenmenger syndrome or ACHD Physiological Stage C or D identify patients with reduced cardiovascular reserve to cope with the specific pathophysiologic demands of COVID-19 infection. It is interesting to consider why previous heart failure admission rather than systolic dysfunction of the subaortic or subpulmonary ventricle was predictive of death after COVID-19 infection.5 6 This may have been due to the relatively modest event rate in all three studies, or the authors’ different definitions of ventricular dysfunction by subjective assessment or echocardiographic ejection fraction, or that previous heart failure admission better captures the complement of heart failure phenotypes that render patients vulnerable to infection, such as systolic/diastolic dysfunction, residual shunt and/or valvular disease.4–6 Relatedly, ventricular systolic function was not wholly unimportant as Broberg et al found that reduced left ventricular ejection fraction was predictive of death (primary outcome) in the subgroup of patients with biochemically confirmed COVID-19 infection. A subaortic right ventricle was also associated with severe infection (secondary outcome) though not with death in the entire cohort.6
The second unanticipated finding from real-world data is that Fontan palliation does not appear to increase patients’ risk of adverse outcomes.4–6 This may reflect their younger age and the greater relative importance of current physiological status as discussed above. It may also reflect a lack of associated patient-specific comorbidities, which were found to be equally important predictors of adverse outcomes after COVID-19 infection and the third surprising finding from real-world data. This may also be a good reminder of the increasing importance of acquired cardiovascular comorbidities over the lifetime for ACHD patients.
These results also highlight geographical differences in approach. The EPOCH studies did not consider ACHD Physiological Stage as a risk factor, which likely reflects the authors’ and participants’ European practice.3 4 In comparison, Lewis et al and Broberg et al were based in the USA.5 6
Finally, Broberg et al also assessed the impact of medications on clinical course. Their results confirmed that ACE inhibitors and angiotensin receptor blockers remain safe for ACHD patients during this pandemic. In comparison, beta blockers were associated with severe infection in the entire cohort and with death in the subgroup of patients with biochemically confirmed infection. This is intriguing to consider in the context of the adverse effects of beta blockers in non-CHD patients with decompensated heart failure, or may be a marker of underlying ventricular dysfunction or arrhythmias. Alternatively, the confirmed cases may represent a more vulnerable population who presented with more severe illness and therefore obtained testing.
A changing paradigm of risk: from anatomy to physiology
The alignment between results from Schwerzmann et al and Ruperti-Repilando et al is perhaps not surprising. By the time Ruperti-Repilado et al surveyed EPOCH centres, 13/23 (57%) centres already had experience treating COVID-19 infection. Regardless, their results provide important real-time cross-sectional assessment of experts’ approach to risk stratification.
The subsequent discussion here highlights the fact that surveyed experts were able to identify most major risk factors for adverse outcomes after COVID-19 infection in ACHD patients prior to available real-world data. However, experts seriously overestimated the importance of anatomical complexity and Fontan palliation, and underestimated the importance of patient-specific risk factors.
Meanwhile, published results have demonstrated the surprising parallels between CHD and non-CHD patients after COVID-19 infection with respect to their overall trajectory of infection (mild, moderate, severe or death) and important patient-specific risk factors. Key CHD-specific risk factors that were identified are cyanosis, supplemental oxygen use, pulmonary arterial hypertension, previous heart failure admission and ACHD Physiological Stage C or D.
These results provide important guidance for priorotising vaccinations as well as our advice to patients. Until now, we as individual providers have been less able to reassure patients regarding their individual risk. Potential sequelae from this include patient-driven delayed or missed care due to their greater worry about attending in-person visits than worry about harm from postponed medical care, unexpected deaths and further psychological distress in this already vulnerable population.7 8 Finally, looking forward, the comparison between real-world data and Ruperti-Repilado et al’s results offers food for thought regarding our current conceptualisation of ‘complexity’ in ACHD patients. Perhaps as a field, we ought to shift away from an anatomy-based model of risk towards a physiology-based model of risk in ACHD patients.
Acknowledgments
Dr EO currently holds the Bitove Family Professorship of Adult Congenital Heart Disease.
Footnotes
Twitter @EOechslin
Contributors Dr EO and Dr SY designed, drafted and critically revised the editorial comment and figure 1. The authors approved the final, submitted version.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Commissioned; internally peer reviewed.