Article Text

Abstract
Background In patients with ST-segment elevation myocardial infarction (STEMI), it is unknown how patient delay modulates the beneficial effects of timely reperfusion.
Aims To assess the prognostic significance of a contact-to-balloon time of less than 90 min on in-hospital mortality in different categories of symptom-onset-to-first-medical-contact (S2C) times.
Methods A total of 20 005 consecutive patients from the Feedback Intervention and Treatment Times in ST-segment Elevation Myocardial Infarction (FITT-STEMI) programme treated with primary percutaneous coronary intervention (PCI) were included.
Results There were 1554 deaths (7.8%) with a J-shaped relationship between mortality and S2C time. Mortality was 10.0% in patients presenting within 1 hour, and 4.9%, 6.0% and 7.3% in patient groups with longer S2C intervals of 1–2 hours, 2–6 hours and 6–24 hours, respectively. Patients with a short S2C interval of less than 1 hour (S2C<60 min) had the highest survival benefit from timely reperfusion with PCI within 90 min (OR 0.27, 95% CI 0.23 to 0.31, p<0.0001) as compared with the three groups with longer S2C intervals of 1 hour<S2C≤2 hours (OR 0.44, 95% CI 0.33 to 0.59, p<0.0001), 2 hours<S2C≤6 hours (OR 0.49, 95% CI 0.38 to 0.64, p<0.0001) and 6 hours<S2C≤24 hours (OR 0.42, 95% CI 0.30 to 0.58, p<0.0001).
Conclusions Timely reperfusion with a contact-to-balloon time of less than 90 min is most effective in patients presenting with short S2C intervals of less than 1 hour, but has also beneficial effects in patients with S2C intervals of up to 24 hours.
Trial registration number NCT00794001.
- acute coronary syndrome
- chest pain
- myocardial infarction
Data availability statement
All data relevant to the study are included in the article and are available on reasonable request from the last author (TF).
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known about this subject?
In ST-segment elevation myocardial infarction (STEMI) patients, the relationship between in-hospital mortality and total ischaemic time defined as the interval from symptom onset to balloon inflation is J-shaped . However, how patient delay modulates the effects of timely reperfusion remains unknown.
What does this study add?
Timely reperfusion within 90 min of the first medical contact is most effective in STEMI patients presenting within a short interval from symptom onset to first medical contact of less than 1 hour. However, it also has beneficial effects in patients with much longer intervals with respect to better survival.
How might this impact on clinical practice?
Our data suggest for the first time that measures for timely reperfusion should be applied to all patients irrespective of patient delay.
Introduction
Early reversal of abnormal epicardial flow by primary percutaneous coronary intervention (PCI) is the primary strategy in acute ST-segment elevation myocardial infarction (STEMI) management to reduce mortality and improve clinical outcome.1–5 Numerous clinical studies have demonstrated that, in STEMI patients, longer ischaemic time following occlusion of an epicardial coronary artery is associated with higher mortality.6–16 In comparison to prolonged occlusion, shorter ischaemic time resulted in decreased infarct size and reduced myocardial damage.17–19 However, how various categories with respect to the duration from symptom onset to first medical contact affect mortality and, in particular, how patient delay modulates the beneficial effects of timely reperfusion remains unknown.
Therefore, in this post hoc analysis, we tested whether early PCI treatment within 90 min of the first medical contact, which is an established standard process metric in the guideline-directed management of STEMI patients,4 20 had beneficial effects on hospital mortality in different patient groups as stratified by the time interval from of the onset of symptoms to the emergency medical service (EMS) arrival at the scene.
Methods
Participating PCI hospitals
The Feedback Intervention and Treatment Times in STEMI (FITT-STEMI) study is an ongoing multicentre trial currently including a network of 47 PCI hospitals throughout Germany. The study aims to assess the prognostic impact of a standardised feedback-driven quality management initiative for timely reperfusion therapy on treatment times and mortality in local STEMI treatment networks. The current analysis included data from the period from January 2006 to December 2017. Details of the protocol of the FITT-STEMI study including the predefined outcome measures have been published elsewhere.5 21 22 The PCI hospitals are obligated to prospectively enrol, without exception, all consecutive STEMI patients who presented within less than 24 hours after onset of infarct symptoms. The population analysed in the present paper comprised all STEMI patients who arrived at the primary PCI hospital via EMS with treatment times of less than 6 hours from arrival at the scene to balloon inflation.
Assessment of symptom onset
Patients were asked to provide information about their precise time of symptom onset related to the current episode of myocardial infarction. Symptoms of angina pectoris were defined as any complaint of chest pain or compression due to myocardial ischaemia, which did not subside spontaneously and occurred both at rest or during exercise. When related to the current episode, pain radiating to left arm, neck or jaw was taken into account. Symptoms indicative of preinfarction unstable angina pectoris were documented. Symptom-to-contact time intervals were categorised in groups with ‘very early’ (S2C≤1 hour), ‘early’ (1 hour<S2C≤2 hours), ‘intermediate’ (2 hours<S2C≤6 hours) and ‘late’ (6 hours<S2C≤24 hours) presentation. Total ischaemic time was the time elapsed from symptom onset, when chest pain became more intense and sustained, to the balloon inflation in the catheterisation laboratory following wire crossing of the culprit lesion.
Clinical data collection
Besides clinical information on symptom onset, data on pre-hospital and in-hospital treatment times were collected for each consecutive STEMI patient on a case-report form. Key treatment times included the time of arrival on the scene by EMS which in Germany is usually staffed both with a trained physician and experienced paramedics. The duration of the transport to the PCI centre, the intra-hospital transfer of the patient to the catheterisation laboratory as well as the time points of puncture and first balloon inflation of the culprit lesion were documented. Furthermore, data were obtained on comorbid diagnoses, medical history, prior medication, blood pressure, heart rate, Killip classification and the thrombolysis in myocardial infarction (TIMI) risk score for STEMI, which is a well-validated prognostication scheme categorising the patient’s risk of death. Results from coronary angiography and the assessment of Killip class were recorded. The FITT-STEMI study was conducted in accordance with the Declaration of Helsinki.
Data analysis and feedback interventions
Site-specific data assessment was completed for each year, and annual feedback interventions were performed. At these meetings, outcome data for each local PCI clinic were discussed in interactive sessions with members of the interdisciplinary STEMI treatment teams, including staff from the local EMS, all physicians and nurses working in the emergency department and the emergency responding system as well as staff members in the cardiac catheterisation laboratory and interventional cardiologists. Based on the site-specific descriptive data, particular attention was given to identify components in the treatment chain which require further improvement in order to shorten transportation times and prevent procedural delays during the time from the first medical contact to direct handoff in the cardiac catheterisation laboratory.
Statistical analysis
For each STEMI patient, relevant treatment time intervals from first medical contact at the scene to balloon inflation were determined from raw data. Study patients were grouped according to the following four S2C intervals: S2C≤1 hour (group 1), 1 hour<S2C≤2 hours (group 2), 2 hours<S2C≤6 hours (group 3) and 6 hours<S2C≤24 hour (group 4). Continuous data were reported as means and SD and compared using analysis of variance, whereas χ2 tests were used to compare categorical variables among the four groups. In addition, the study population was dichotomised along the guideline-recommended cut-off level for contact-to-balloon time of equal to or less than 90 min. Logistic regression analyses were performed to examine the impact of duration of symptom onset to EMS arrival at the field on mortality and how this relationship was affected by the treatment time to reperfusion. In a basic model, contact-to-balloon time of ≤90 min and its interaction term with symptoms duration as classified by the four groups were used as independent variables. The group with the shortest symptom onset (S2C≤1 hour) was set as the reference category. To identify significant predictors of in-hospital mortality, a logistic regression model was computed using a stepwise backward-selection method. Likewise, the model used dichotomised data for contact-to-balloon time along the 90 min cut-off level as the independent variable and was adjusted for the following potential confounders: age, gender, arterial hypertension, diabetes mellitus, hyperlipoproteinaemia, family history of myocardial infarction, smoker status, previous stroke, renal failure, number of coronary arteries narrowed, electrocardiographic localisation and recanalisation of the culprit coronary artery, chronic vessel occlusion in a non-infarct-related coronary artery, and TIMI flow grades before and after PCI (score ≤2 vs 3). The results from the regression analyses are presented as OR with their 95% CIs. Supporting analyses were carried out taking only patients without out-of-hospital cardiac arrest (OHCA) into consideration; furthermore, the thresholds 60 min and 120 min rather than 90 min for the contact-to-balloon time were additionally used. The reported p values are all two sided, and p values of <0.05 were considered statistically significant. No formal adjustment for multiple testing was carried out. Statistical analyses were performed on a personal computer using the software program SAS V.9.4 (SAS Institute).
Results
Baseline characteristics and treatment times in patients with different symptom-to-first medical contact intervals
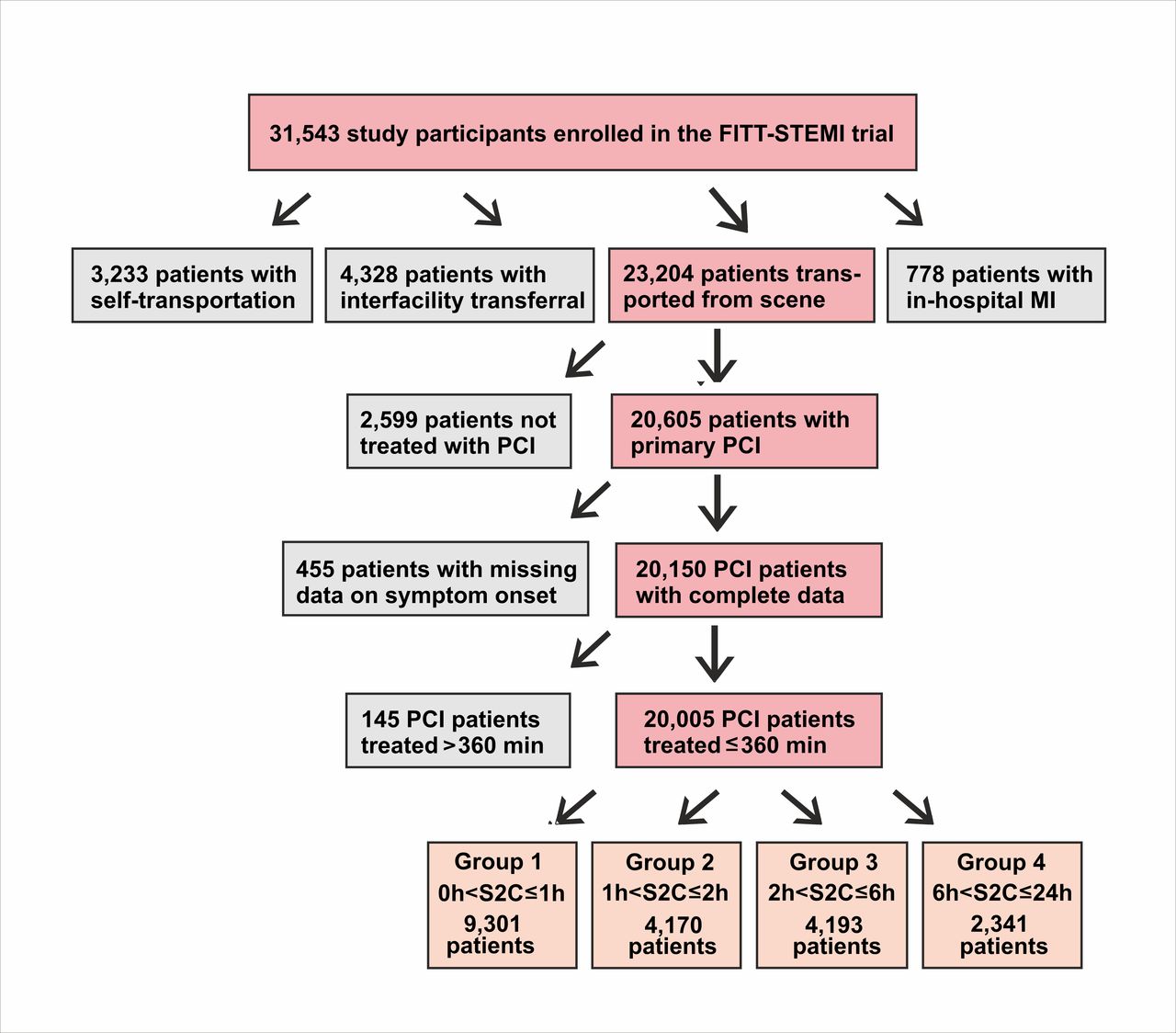
The total study population comprised 20 005 PCI-treated STEMI patients with complete survival data who were transported by EMS and had treatment times of less than 360 min from arrival at the scene to reperfusion (figure 1). The mean age of the study population was 63.8±12.8 years and the majority were men (14 721; 74%). Epidemiological and clinical data including comorbidities of the total study population are presented in table 1. The proportions of females and older subjects increased in patient groups with longer S2C intervals (both p<0.0001). Pre-hospital and intra-hospital times to reperfusion differed with respect to duration of chest pain. Patients with an S2C time lasting longer than 6 hours had the shortest mean contact-to-door time (37.0±15.9 min, p<0.0001) (table 1). In contrast, this group also had the longest documented door-to-balloon time (60.8±44.0 min, p<0.0001) and contact-to-balloon time (97.7±47.3 min, p<0.0001), indicating significant delays in the intra-hospital treatment chain. These delays during intra-hospital transport did not result from a higher proportion of patients transported via the emergency department, since the ratio of patients bypassing the emergency department in this group (54%) was in the same range as in patients with shorter symptom duration (p=0.2640).
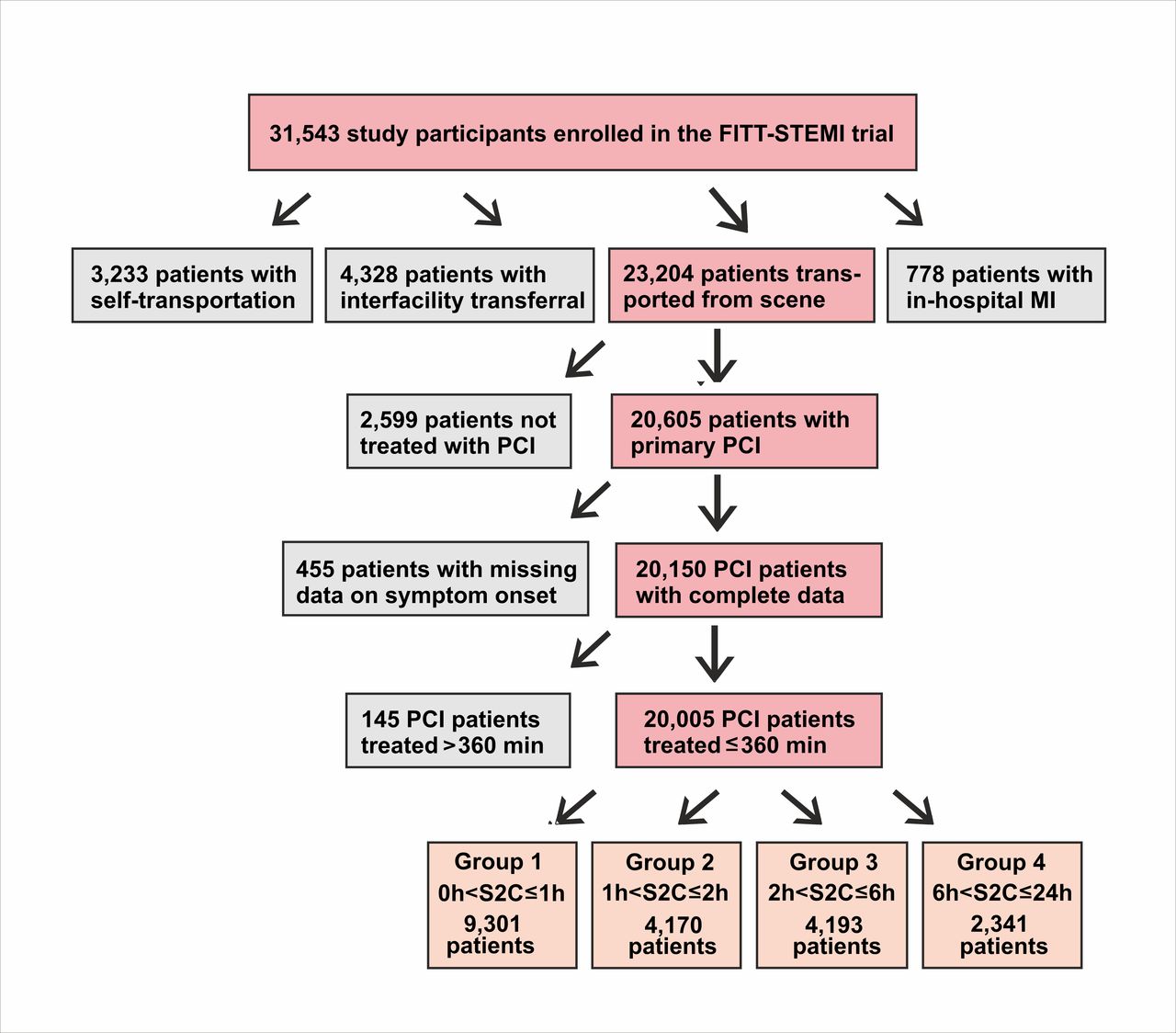
Flow diagram of the PCI-treated STEMI patients from the FITT-STEMI study population as stratified by four groups of symptom-onset-to-first-medical-contact times. FITT-STEMI, Feedback Intervention and Treatment Times in ST-segment Elevation Myocardial Infarction; PCI, percutaneous coronary intervention.
Demographic, clinical and angiographic characteristics of STEMI patients
Hospital mortality depending on patient delay
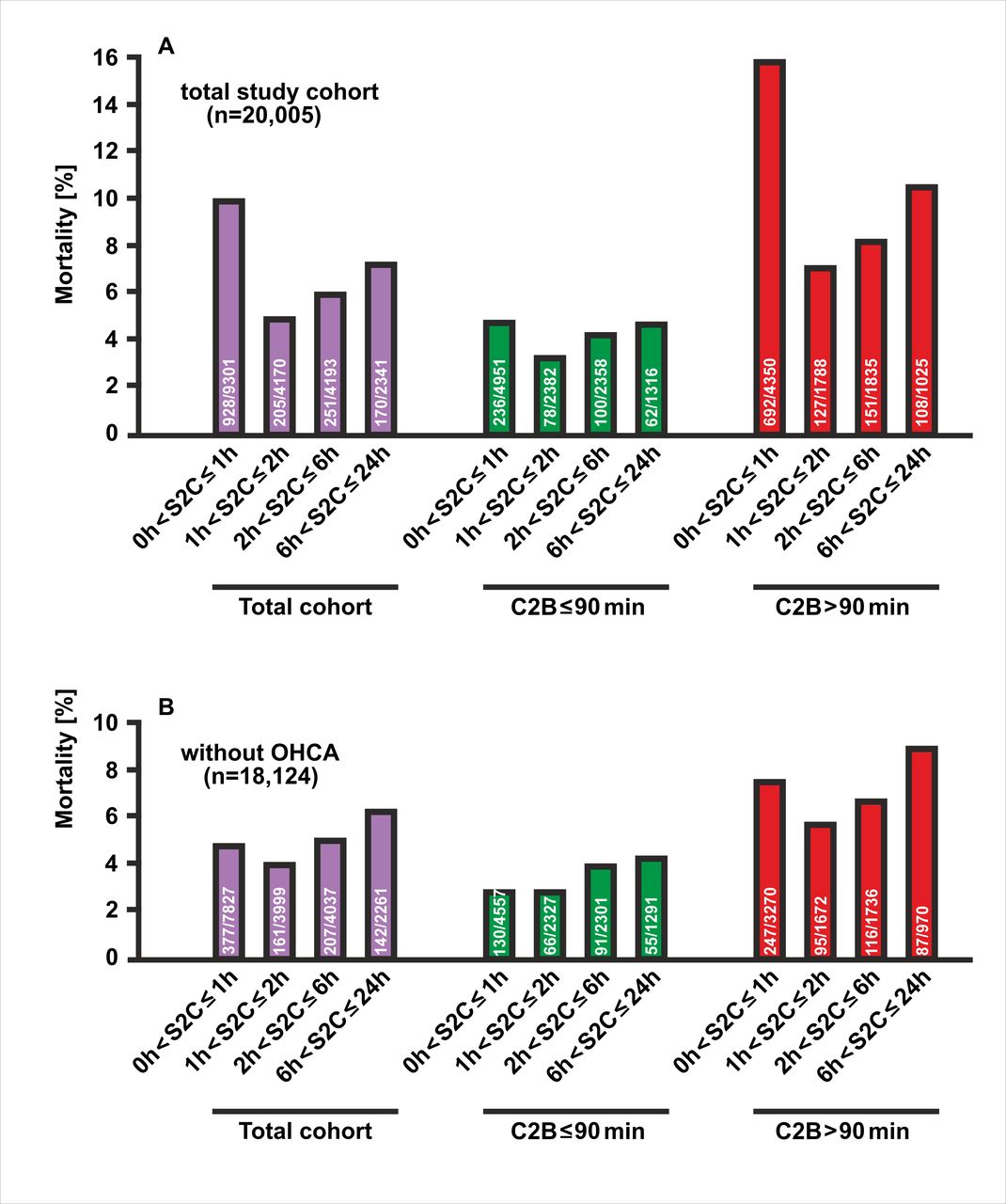
There were 1554 (7.8%) deaths in the total study population. Hospital mortality differed significantly according to the time from symptom onset to first medical contact (p<0.0001). The cohort of 455 patients with unknown times of symptom onset, who were excluded from the present analysis (see figure 1), had the highest mortality rate (79 deaths, 17.4%). Mortality was also high in patients reporting a short S2C time, as 928 out of 9301 study participants in group 1 (10%) died during the hospital treatment (figure 2A). The poor outcome in this group most probably resulted from a more than twofold higher prevalence of cardiogenic shock (18% vs 7%, p<0.0001) and a fourfold higher occurrence of OHCA (16% vs 4%, p<0.0001, table 1) compared with the remaining groups with an interval from symptom onset to EMS arrival of more than one hour. Mortality was lowest in STEMI patients with a moderate S2C time of one to two hours (205 deaths out of 4170 patients, 4.9%). Prolonged chest pain in the two groups with symptom durations ranging from 2 to 6 hours (group 3) and 6 to 24 hours (group 4), respectively, resulted in an increase in mortality (6.0% and 7.3%), which however did not reach the high mortality in STEMI patients with the shortest symptom duration of ≤1 hour (group 1). Excluding patients with OHCA, mortality was considerably reduced in the group with very early presentation (S2C≤1 hour: 377 deaths out of 7827 patients, 4.8%), and decreased moderately in the second group with early presentation (161 deaths out of 3999 patients, 4,0%), and again increased in the other two groups with intermediate (207 deaths out of 4037 patients, 5.1%) and late presentation (142 deaths out of 2261patients, 6.3%) (figure 2B).

In-hospital mortality of PCI-treated STEMI patients by different categories of time intervals from the symptom onset to the arrival of the EMS at the scene. (A) Depicted are the percentages of deaths among the four groups in the total study population (purple), in patients with a contact-to-balloon time of equal to or less than 90 min (green) or longer (red). (B) Mortality data as in (A) for the subgroup of STEMI patients who had not experienced out-of-hospital cardiac arrest (OHCA). EMI, emergency medical service; PCI, percutaneous coronary intervention; STEMI, ST-segment elevation myocardial infarction.
Better survival after timely reperfusion irrespective of symptom duration
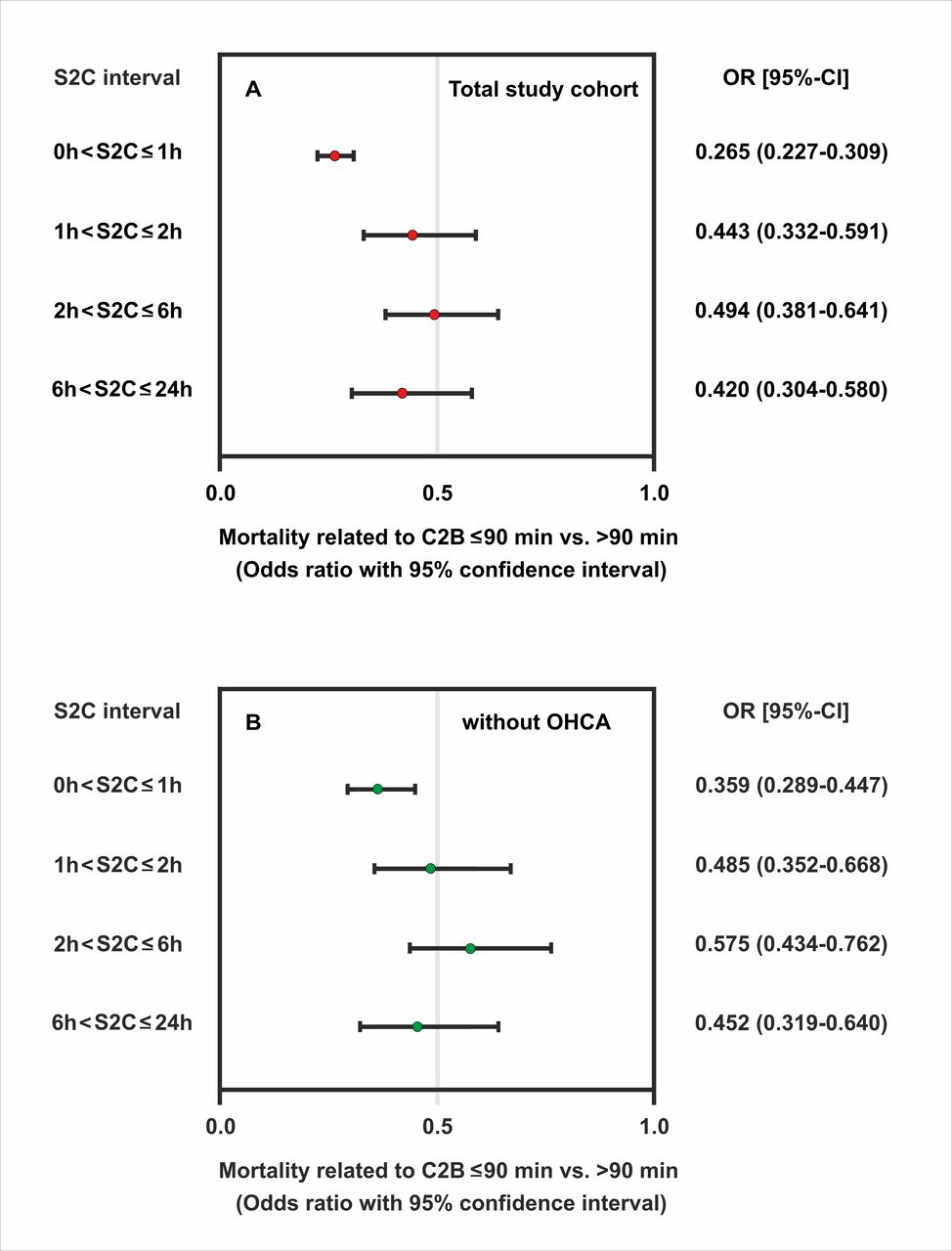
Reperfusion within 90 min of the first medical contact was a significant predictor of better survival, as for all S2C groups there were fewer deaths when time to reperfusion after EMS arrival did not exceed 90 min. Again, there were two peaks of high mortality, irrespective of whether or not the aim of a 90 min contact-to-balloon time was achieved. Mortality was highest in patients with an extremely short symptom duration of not more than 1 hour (4.8% and 15.9%, respectively), followed by a second peak at prolonged symptom duration (4.7% and 10.5%) (figure 2A). In an unadjusted model, patients with a reported symptom onset of ≤1 hour benefited the most from timely reperfusion as determined by a contact-to-balloon time of ≤90 min compared with their counterparts with a time to PCI treatment of >90 min (OR 0.27, 95% CI 0.23 to 0.31, p<0.0001) (figure 3A). Similar results were observed for the remaining three groups with longer symptom onset, as in-hospital mortality was always significantly lower when PCI was performed within 90 min after first medical contact.
{kind=link}
{kind=link}
{kind=link}
Odds ratios of mortality related to timely reperfusion as determined by a contact-to-balloon time of ≤90 min compared with >90 min and their corresponding 95% CI by categories of symptom-onset-to-first-medical contact time. Data are shown for the total study sample (A) and in the subgroup of patients without OHCA (B). OHCA, out-of-hospital cardiac arrest.
Notably, in the subgroup of STEMI patients without OHCA (n=18 124), timely treatment within the guideline-recommended 90 min interval after first medical contact significantly improved survival in each of the four symptom-to-contact groups (figures 2B and 3B). Beneficial effects of timely PCI treatment were also observed for all symptom-to-contact groups using different cut-offs for contact-to-balloon times. Similar mortality profiles were found for the two contact-to-balloon times at 60 min and 120 min, respectively (online supplemental figure 1 and online supplemental table 1).
Supplemental material
Finally, we assessed the impacts of S2C time on timely PCI treatment and their relation to mortality using a logistic regression model adjusted for baseline characteristics (table 2). This model used the four groups of symptom onset and the dichotomised data for contact-to-balloon time along the 90 min cut-off level and was adjusted to a variety of clinically important variables. Again, patients with an onset of symptoms within 60 min of the arrival of the EMS at the scene benefited the most from timely reperfusion with respect to survival (OR 0.56; 95% CI 0.46 to 0.68). Although data indicated better survival with a contact-to-balloon time of ≤90 min across the entire patient population, this did not reach statistical significance for the second to the fourth group.
Multivariable logistic regression model with in-hospital mortality as dependent variable and the guideline-recommended cut-off level of contact-to-balloon time (≤90 min) for four groups of symptom onset as independent variable adjusted to the indicated confounders
Discussion
Analysing the prognostic role of different S2C intervals in STEMI patients, we noted two important findings: first, our data show a J-shaped relationship between the time duration from symptom onset to first medical contact and in-hospital mortality. Second and most importantly, we found that timely reperfusion within 90 min of the first medical contact is most effective in STEMI patients presenting within a short S2C interval of less than 1 hour, but also has beneficial effects in patients with much longer S2C intervals.
While some authors reported that the total ischaemic time (ie, symptom-onset-to-balloon time) was inversely linked to survival,6 10 23 one study demonstrated that the relationship between total ischaemic time and mortality appeared to be rather complex not with a single, but two peaks separated by a trough, indicating lower mortality at 5 hours after symptom onset.24 The investigators in this prospective, observational Japan Acute Myocardial Infarction registry suggested that the link between ischaemic time and mortality was determined by the influence of two independent components: One was the outcome during the initial 3 hours for high-risk STEMI patients, while the other was the outcome of patients who survived the initial high risk period and were then exposed to the haemodynamic consequences of a long-lasting vessel occlusion.24
We observed the highest mortality rates in PCI-treated STEMI patients presenting within 1 hour of onset of symptoms (10%). Patients with S2C times between 1 and 2 hours had the lowest rate of hospital deaths (4.9%). A second mortality peak was seen in the group of patients with prolonged symptom duration lasting for longer than 6 hours before EMS arrival (7.3%).
In our analysis comparing different intervals from symptom onset to first medical contact, we found that patients from the high-risk group with a short symptom onset of within one hour were the youngest and had the lowest proportion of diabetes mellitus. Nevertheless, in this group, the prevalence of cardiogenic shock as a consequence of myocardial infarction was more than twice as high as in any of the other remaining groups (18% vs 7%). Similarly, we observed a high prevalence for OHCA with need of instant cardiopulmonary resuscitation in the patient group with a short interval from symptom onset to arrival of EMS, which was more than four times higher as compared with STEMI patients with a prolonged symptom duration exceeding one hour (15.8% vs 3.8%). The high mortality observed in STEMI patients presenting with an S2C time of ≤1 hour may have resulted from adverse haemodynamic complications, reflecting the severity of the ischaemic myocardial damage in this high-risk group. Excluding patients with OHCA resulted in considerably reduced mortality in the group with very early presentation (S2C≤1 hour). Timely treatment from first medical contact to balloon inflation of less than 90 min resulted in an improved survival in this group and in the other groups with early, intermediate and late presentation.
Terkelsen et al divided the total ischaemic time in ‘patient delay’ and ‘system delay’,2 whereby the latter but not the former can be influenced by the healthcare provider. From the perspective of the healthcare provider, the question is whether the magnitude of the benefit of timely PCI depends on the extent of patient delay (ie, the time from symptom onset to first medical contact). In our analysis, it is striking that shortening system delay (ie, the time from first medical contact to PCI) still has a beneficial effect even with extended patient delays and long S2C time intervals. These beneficial effects of timely reperfusion even in STEMI patients with prolonged duration of symptoms could be due to a variety of mechanisms such as incomplete or intermittent occlusion of the infarct-related artery, residual blood flow by recruitment of collaterals and ischaemic preconditioning, thereby preventing complete necrosis and preserving viable myocardium.25–27
Several issues merit consideration in the interpretation of our findings. First of all, the time point of symptom onset is critical to our analysis but hard to define. Since our study is observational in nature, the collection of patients’ data might be susceptible to unmeasured confounding and selection bias, which were not been systematically evaluated, such as objective criteria for the onset of ischaemia (eg, increase in serum markers such as troponin and imaging). Thus, any conclusion about causality between the time from symptom onset to first medical contact and outcome is of limited validity from our observational study, which of course limits the generalisability of our results in other clinical settings. Owing to the limited follow-up, only in-hospital mortality was included in our analysis, while data on longitudinal outcomes at longer follow-up periods were not available. In addition, our findings from the FITT-STEMI study conducted in Germany may not be directly applicable to STEMI management care systems in other countries, in which physicians experienced in emergency medicine are not part of the EMS teams. Moreover, it cannot be excluded that the attendance of both physicians and paramedics in EMS transportation might have accounted for the beneficial effects of shortened treatment times on survival seen in our different patient groups. Another limitation relates to the fact that it is unknown how the exclusion of formalised data analysis and interactive feedback sessions would affect the results from similar investigations without this intervention, since quality management improvement is an integral and essential component of the FITT-STEMI study design.
In summary, our findings demonstrate that timely revascularisation by means of PCI therapy within the guideline-recommended 90 min from first medical contact is a critical component of improvement of outcomes in myocardial infarction, irrespective of the time from symptom onset. In order to improve outcome, minimising system delay should be followed in all patients across a wide range of S2C time intervals up to 24 hours.
Data availability statement
All data relevant to the study are included in the article and are available on reasonable request from the last author (TF).
Ethics statements
Patient consent for publication
Ethics approval
The study was approved by the ethics committee of the Medical Faculty at the University of Göttingen and the local ethics committees of all participating PCI centres (GAU1/10//07).
Acknowledgments
We thank Hans-Joachim Radtke and Michael Jur (UniPro Software corporation, Halberstadt, Germany) providing web-based data acquisition and delivery of raw data, as well as Phillip Scholz and Nikos Tirilomis (Universitätsklinikum Göttingen) preparing regular feedback analyses for each single participating hospital. Hospitals participating in the FITT STEMI consortium and list of contributors: St. Bernward-Krankenhaus Hildesheim (Karl Heinrich Scholz; Barbara Bartels; Christina Planke); Universitätsklinikum Würzburg (Björn Lengenfelder; Verena Grünewald; Sebastian K.G. Maier); Klinikum Worms (Jens Jung; Birgit Nicklas); Klinikum Darmstadt (Hiller Moehlis; Gerald S. Werner); Klinikum Wolfsburg (Claus Fleischmann; Rüdiger Becker; Rolf Engberding); Universitätsklinikum Göttingen (Tim Seidler; Claudius Jacobshagen; Kristina Schröder; Svetlana Hartmann; Nadine Heydrich; Lars S. Maier); Asklepios Klinikum Langen (Marcus Mittag; Melanie Hauff; Ralf Lehmann; Hans G. Olbrich; Kerstin Eck); Klinikum Oldenburg (Susanne Grafmüller; Albrecht Elsässer; Annette Schütz); Städtisches Klinikum München Neuperlach (Anamaria Stote; Michael Danner; Stefan Sack; Martin Hug; Harald Mudra); Helios Klinikum Krefeld (Rainer Ott; Ursula Jansen; Heinrich G. Klues; Alexander Bufe); Krankenhaus Rothenburg ob der Tauber (Christian Wacker); Marienkrankenhaus Soest (Roland Bürger; Markus Flesch); Kreiskrankenhaus Eschwege (Peter Schott; Marco Lubitz; Tobias-Richard Meinel); Krankenhaus Landshut-Achdorf (Ute Zrenner; Bernhard Zrenner; Josef Haimerl); Klinik am Eichert Göppingen (Stephen Schröder; Marion Steindl; Josef Steindl; Sophia Atseles); Klinikum Ingolstadt (Silke Gläser; Katrin Thiele; Karlheinz Seidl); Universitätsklinikum Jena (Corinna Schneider; P. Christian Schulze; Daniel Kretzschmar); Klinikverbund Kempten-Oberallgäu (Carsten Bauer; Wulf Ito); Robert-Bosch-Krankenhaus Stuttgart (Stephan Hill; Andrea Bullinger; Udo Sechtem); Klinikum Lüneburg (Jan Priesack; Christian Weiss; Claus H. Müller); Krankenhaus Buchholz (Werner Raut; Klaus Hertting; Liana Hertting); Regio Klinikum Pinneberg (Konrad Gorski; Thomas Hofmann); Klinikum Lippe-Detmold (Melanie Kriete; Dirk Haertel; Ulrich Tebbe); Klinikum Region Hannover-Siloah (Andreas Franke; Jan Fürste; Rania Jebrini; Fred Aumüller); Klinikum Deggendorf (Martina Silova; Rainer Burckhard; Martin Giesler); Klinikum Leer (Christian Vahlhaus; Ralf Pretzsch); Asklepios Harzklinik Goslar (Gaby Lehnert; Thomas Wittlinger; Tobias Steffen; Arnd B. Buchwald; Christoph Engelhardt); Kliniken Ostallgäu-Kaufbeuren Füssen (Simon Delladio; Martin Hinterseer; Myriam Parvanov); Klinikum St. Elisabeth Straubing (Sebastian K.G. Maier; Elke Grassl; Florian Brattinger; Stilla Jacobs); Klinikum Neumarkt (Christian Schmidt; Melina Dykczak; Veronika Lingg); Universitätsklinikum Augsburg (Georg Waidhauser; Christian Thilo; Wolfgang von Scheidt); Klinikum Ludwigsburg (Stefan Stefanow; Ralf Berroth; Joachim Geiger; Friederike Wunsch; Christian Wolpert); Sana Kliniken Lübeck (Hans-Martin Grusnick; Joachim Weil); Allgemeines Krankenhaus Viersen (Nicolas von Beckerath; Barbara Vogel; Birger Horn); Medizinische Hochschule Hannover (Jörn Tongers; Cicek Yarcu; Ulrike Flierl; Benedikta Ritter; Johann Bauersachs); Klinikum REGIOMED-Kliniken Coburg (Steffen Schnupp; Andrea Scharmentke; Karoline Kleinecke; Andrea Linss; Kerstin Truthan; Hans-Joachim Goller; Johannes Brachmann); Kreiskrankenhaus Dormagen (Benjamin Orth; Georg Haltern); Hermann-Josef-Krankenhaus Erkelenz (Vera Schiwietz; Christina Ridt; Klaus Dieter Winter); Klinikum Landkreis Erding (Lorenz Bott-Flügel); Krankenhaus Henriettenstift Hannover (Thomas Weiss; Lisa Landsmann; Thorsten Grundmann); SLK Kliniken Heilbronn (Marcus Hennersdorf; Jens Martin Maier; Eva Schropp); Kliniken Maria Hilf Mönchengladbach (Jürgen vom Dahl; Gregor Nothofer; Dierk Rulands); Vinzenzkrankenhaus Hannover (Beate Bugdoll; Arno Lutz; Christian Zellerhoff; Petra Wucherpfennig; Jan-Bernd Schüttert); Universitätsklinikum Regensburg (Stefan Neef; Bailey-Marie Johnson; Christina Strack; Dierk Endemann; Lars S. Maier); SLK Kliniken Am Plattenwald Bad Friedrichshall (Thomas Dengler; Christine Lindner); Evangelisches Krankenhaus Bethesda Mönchengladbach (Thomas Lickfeld); Krankenhaus Bethanien Moers (Alexander Donath; Stefan Möhlenkamp); DRK-Krankenhaus Clementinenhaus Hannover (Heinz-Peter Remmlinger; Constanze Behne); Johanna-Etienne-Krankenhaus Neuss (Till Falke); Rems-Murr Kliniken Winnenden (Andreas Jeron; Michaela Schorer); Universitätsklinikum Aachen (Jörg Schröder; Gabriele Heuer; Stefan Beckers); St. Antonius Hospital Eschweiler (Andrea Wings; Andreas Niedeggen; Johannes Nußbaum; Uwe Janssens); Städtische Kliniken Mönchengladbach (Dierk Rulands; Katharina Grün-Himmelmann); Universitätsklinikum Münster (Lena-Maria Makowski; Marion Pohl; Christian Pogoda; Georg Haltern); Krankenhaus Reinbek St. Adolf Stift (Claudia Zeiler-Reich; Ali Aydin)
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors KHS was responsible for conception, design of the study and obtaining funding. KHS, BL, CV, JT, SS, RB, NvB, HMG, AJ, KDW, SM, MD, JvD, SN and SS contributed to subject recruitment and data acquisition. KHS, TM and TF analysed the clinical data. TF performed the statistical analysis. All authors made substantial contributions to analysis and interpretation of data. KHS, TM and TF drafted the manuscript. All authors critically revised and reviewed the manuscript. All authors read and approved the final manuscript. KHS, TM and TF agreed to be responsible for the overall content as guarantors.
Funding This study was supported by a grant from the Deutsche Herzstiftung e.V. and the Arbeitsgemeinschaft Leitender Kardiologischer Krankenhausärzte to KHS.
Competing interests TF reports personal fees for consultancies (including data monitoring committees) from Novartis, Bayer, Biogen, AstraZeneca, Janssen, Grünenthal, Pharmalog, SGS, Boehringer Ingelheim, Daiichi-Sankyo, Mediconomics and Roche, all outside the submitted work. Furthermore, he has received research funding by the European Commission for statistical analyses on the EUTrigTreat (NCT01209494) and EU-CERT-ICD (NCT02064192) clinical studies. All relationships declared are modest.
Provenance and peer review Not commissioned; externally and internally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.