Article Text

Abstract
Objective In a proof-of-concept study, to quantify myocardial viability in patients with acute myocardial infarction using manganese-enhanced MRI (MEMRI), a measure of intracellular calcium handling.
Methods Healthy volunteers (n=20) and patients with ST-elevation myocardial infarction (n=20) underwent late gadolinium enhancement (LGE) using gadobutrol and MEMRI using manganese dipyridoxyl diphosphate. Patients were scanned ≤7 days after reperfusion and rescanned after 3 months. Differential manganese uptake was described using a two-compartment model.
Results After manganese administration, healthy control and remote non-infarcted myocardium showed a sustained 25% reduction in T1 values (mean reductions, 288±34 and 281±12 ms). Infarcted myocardium demonstrated less T1 shortening than healthy control or remote myocardium (1157±74 vs 859±36 and 835±28 ms; both p<0.0001) with intermediate T1 values (1007±31 ms) in peri-infarct regions. Compared with LGE, MEMRI was more sensitive in detecting dysfunctional myocardium (dysfunctional fraction 40.5±11.9 vs 34.9%±13.9%; p=0.02) and tracked more closely with abnormal wall motion (r2=0.72 vs 0.55; p<0.0001). Kinetic modelling showed reduced myocardial manganese influx between remote, peri-infarct and infarct regions, enabling absolute discrimination of infarcted myocardium. After 3 months, manganese uptake increased in peri-infarct regions (16.5±3.5 vs 22.8±3.5 mL/100 g/min, p<0.0001), but not the remote (23.3±2.8 vs 23.0±3.2 mL/100 g/min, p=0.8) or infarcted (11.5±3.7 vs 14.0±1.2 mL/100 g/min, p>0.1) myocardium.
Conclusions Through visualisation of intracellular calcium handling, MEMRI accurately differentiates infarcted, stunned and viable myocardium, and correlates with myocardial dysfunction better than LGE. MEMRI holds major promise in directly assessing myocardial viability, function and calcium handling across a range of cardiac diseases.
Trial registration numbers NCT03607669; EudraCT number 2016-003782-25.
- magnetic resonance imaging
- myocardial infarction
- heart failure
Data availability statement
All data relevant to the study are included in the article or uploaded as online supplemental information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known about this subject?
The ability to define viability following an acute myocardial infarction is invaluable in guiding management.
What does this study add?
This study has demonstrated that manganese-enhanced MRI not only more accurately quantifies areas of myocardial dysfunction following ischaemic injury but can directly identify viable as well as recovering stunned myocardium.
How might this impact on clinical practice?
We believe that manganese-enhanced imaging holds major promise for early detection and quantification of myocardial stunning and viability, with the potential for improved patient selection for revascularisation and novel therapeutic interventions for myocardial recovery.
Introduction
Coronary heart disease is a leading cause of morbidity and mortality worldwide1 2 and the subsequent development of heart failure is associated with major healthcare costs.3 Patients with ischaemic or dysfunctional myocardium benefit from pharmaceutical and revascularisation therapies4 but optimal patient selection is an ongoing and complex clinical challenge.
In MRI, late gadolinium enhancement (LGE) identifies areas of infarction and is an established measure of myocardial viability5 through its ability to define the scar burden6 and indirectly infer viability.7 However, accurate quantification of infarction in the acute setting can be challenging and infarct size is often overestimated, due to tissue oedema.8 9 18F-fluorodeoxyglucose (18F-FDG) is a radiolabelled glucose analogue which is used in cardiac positron emission tomography (PET) to detect glucose metabolism in functional viable myocardium.10 This is considered gold standard for quantifying myocardial viability.11 12 However, its widespread use is limited by accessibility, radiation exposure and expertise. This highlights the lack of alternative contrast media and our dependence on gadolinium-enhanced imaging.
Preclinical studies have demonstrated that manganese-enhanced MRI (MEMRI) accurately quantifies myocardial infarction, both at acute and chronic time points.13 14 Manganese, a calcium analogue, has comparable paramagnetic properties to gadolinium but is taken up by functional myocardium through cardiomyocyte calcium channels.15 Preclinical work has demonstrated excellent agreement between MEMRI and 18F-FDG PET in the quantification of myocardial viability.10 16 17 In this proof-of-concept study of patients with acute myocardial infarction, we aimed to assess the ability of MEMRI to discriminate viable from infarcted myocardium, to identify stunned but viable myocardium, and to provide a quantitative measure of myocardial calcium handling.
Methods
This was a single-centre open-label observational cohort study.
Patients
Adult patients (≥18 years of age) with acute myocardial infarction were recruited from the Edinburgh Heart Centre between May 2018 and July 2019. Inclusion criteria were the diagnosis of ST-segment elevation myocardial infarction according to the universal definition of myocardial infarction18 and angiographically proven left main stem, left anterior descending or multivessel vessel disease. Patients were required to be clinically stable with reduced left ventricular ejection fraction (≤50% by echocardiography) secondary to one or more acute ischaemic events. Healthy volunteers were recruited as a control population and had no known pre-existing medical conditions. Exclusion criteria for all participants were any contraindication to MRI, contraindications to manganese dipyridoxyl diphosphate (MnDPDP) administration (high degree atrioventricular block, history of torsades de pointes or prolonged QTc interval, obstructive liver disease, maintenance on calcium-channel blockade or digoxin therapy), renal failure (estimated glomerular filtration rate <30 mL/min/1.73 m2), New York Heart Association class IV heart failure and women of childbearing potential without a negative pregnancy test.
MRI
MRI was performed using a Siemens MAGNETOM Skyrafit 3T scanner (Siemens Healthineers, Erlangen, Germany), combining elements of spine and body array coils. All study participants underwent scanning with both LGE and MEMRI, 48 hours apart and in random order. Images were acquired with ECG-gating and during held expiration. Cine imaging was acquired with standard steady-state free precession sequences in long and short-axis orientations. T2 mapping was used to quantify T2, with T2 prepared steady-state free precession acquisition. T1 was quantified for each voxel using T1 mapping with Shortened Modified Look-Locker Inversion recovery (ShMOLLI, WIP #1048 Siemens Healthineers).19 Quantitative estimation of native T1 was performed in a full short-axis stack from mitral valve annulus to apex and standard long-axis slices, with additional slices positioned appropriately to characterise pathology. T1 relaxation times were measured before and after administration of contrast media. After completion of the acute phase imaging protocol, patients were invited to return for repeat scanning with an identical protocol after 3 months (online supplemental methods).
Supplemental material
Late gadolinium enhancement
LGE images were acquired from 7 min following intravenous administration of gadobutrol (0.1 mmol/kg; Gadovist, Bayer, Germany) using a single breath held phase-sensitive inversion recovery short-axis stack, and long axis orientations. A standardised inversion time of 400 ms was used and adjusted as required for optimal myocardial nulling. Postcontrast T1 mapping was performed with short-axis ShMOLLI stack 20 min after contrast administration (online supplemental methods).
Manganese-enhanced MRI
MEMRI was achieved using intravenous infusion of MnDPDP (5 μmol/kg, 1 mL/min; maximum dose of 10 mL/patient; Exova SL Pharma, Wilmington, Delaware, USA), imaging every 2.5 min following administration for 40 min, as described previously13 20 (online supplemental methods).
Image analysis
All analyses of T1 maps, LGE and cine-derived volumetric and functional sequences were performed using Circle Cardiovascular Imaging (CVI), CVI 42 V5.6.9, Calgary Canada, online supplemental methods).
Kinetic modelling
To derive quantitative estimates and to assess differential manganese uptake, a compartmental model analysis was performed based on the Patlak formulation (online supplemental methods and figure S2).21 Contrast kinetic modelling was performed using in-house software22 developed in Matlab (MathWorks, V.R2016a, Natick, Massachusetts, USA).
Statistical analysis
All statistical analyses were performed with GraphPad Prism (GraphPad Software V.8.0.2, San Diego, California, USA). Continuous data were assessed for normality using the D’Agostino-Pearson test. Categorical baseline variables were compared using Fisher’s exact test. To compare cardiac function and change in myocardial manganese uptake in patients and healthy volunteers, volumetric assessment and parametric mapping values were compared using paired or unpaired t-tests, Wilcoxon or Mann-Whitney tests, and analysis of variance (ANOVA) or Kruskal-Wallis tests as appropriate. Statistical significance was taken as two-sided p<0.05.
Results
Twenty healthy volunteers and 20 patients following acute ST-segment elevation myocardial infarction underwent LGE and MEMRI scanning 48 hours apart. All patients were treated with primary percutaneous coronary intervention and underwent their first MRI at 3.2±1.8 days. The majority (n=13) of patients had peak high-sensitivity cardiac troponin I concentration >50 000 ng/L with the remaining seven patients having mean concentration of 36 621±13 574 ng/L (normal reference ranges: <34 ng/L for men and <16 ng/L for women). Fourteen patients agreed to return 3 months following myocardial infarction for repeat imaging with an identical protocol.
The patient group was older with more cardiovascular risk factors than healthy control subjects (table 1). Patients had lower ejection fraction and higher left ventricular mass index and extracellular volume fraction (p<0.0001 for all, table 2) with most presenting with anterior territory myocardial infarction (anterior, n=14, (70%); inferior, n=4, (20%), lateral, n=2 (10%)). Infarct size was similar between patients allocated to delayed-enhancement MRI or MEMRI first (35.2±12.9 vs 34.6%±15.6%, p=0.93).
Baseline characteristics
Cardiac magnetic resonance characteristics
Manganese infusion
Fifty-four infusions of MnDPDP were completed during the course of the study (mean duration 10 mins). There were no changes in the ECG, heart rate or blood pressure (online supplemental figures S3 and S4) following MnDPDP administration (p>0.1 for all). One healthy volunteer experienced mild transient nausea for <10 s after commencing MnDPDP infusion, spontaneously resolving without intervention. Otherwise, administration of MnDPDP was well tolerated with no adverse reactions reported during or immediately after administration or at follow-up at 7 days.
MEMRI in healthy volunteers
In healthy volunteers, MnDPDP rapidly reduced blood pool T1 during the infusion (mean reduction 453±96 ms or 25.8%), followed by normalisation to baseline by 40 min (figure 1). Myocardial T1 also demonstrated a rapid initial descent (infusion phase) but this was followed by a slower, more gradual reduction which continued throughout the 40-minute imaging period (mean reduction 288±34 ms or 25.7%).
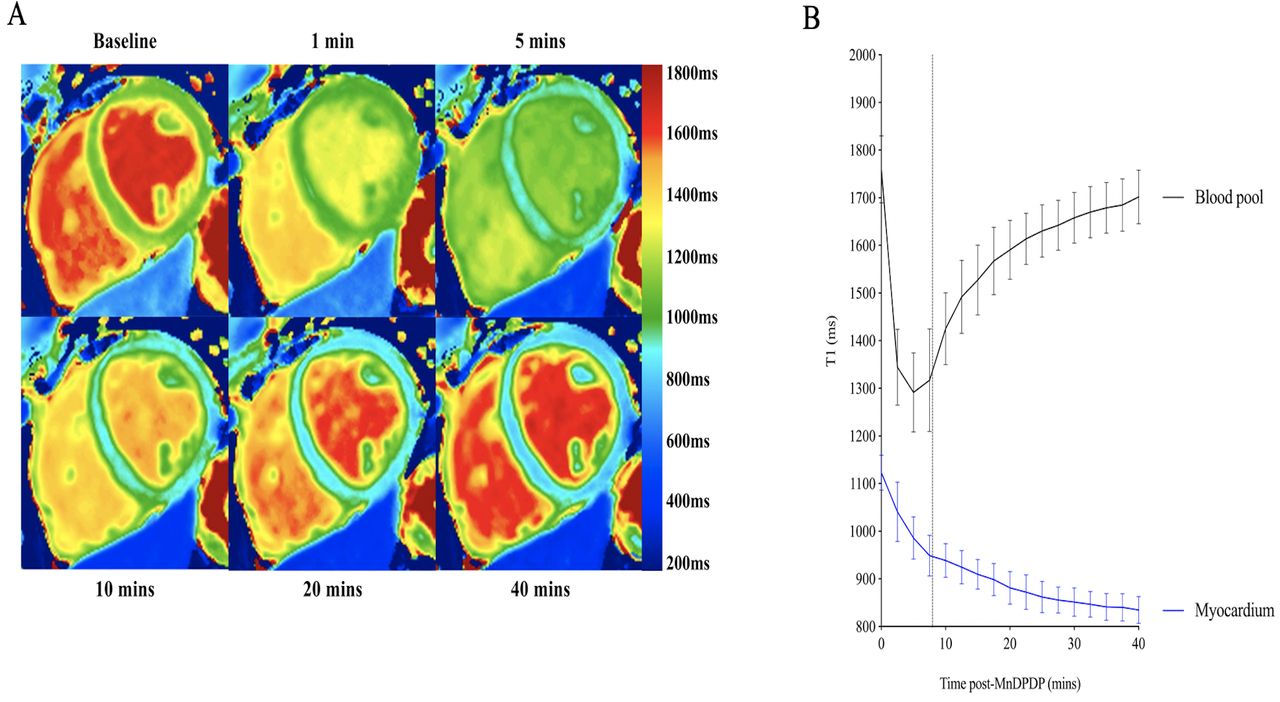
Manganese-enhanced MRI in healthy volunteers. Representative T1 colour maps (A) and T1 over time (B, n=20) following manganese dipyridoxyl diphosphate (MnDPDP). Dashed line represents mean end of infusion, SD of the mean.
MEMRI in acute myocardial infarction
In patients with acute myocardial infarction, the T1 profile in areas of remote non-infarcted myocardium was similar to normal myocardium in the healthy volunteers (mean reduction 281±12 ms or 24.6%; compared with healthy volunteers, p=0.5). However, the T1 profile following MnDPDP in regions of myocardial infarction differed substantially. In particular, areas of transmural infarction demonstrated a partial recovery of T1 values similar to that of the profile observed in the blood pool (figure 2A,C), whereas in areas of less extensive subendocardial myocardial injury, T1 values plateaued after the infusion phase (figure 2B,D).
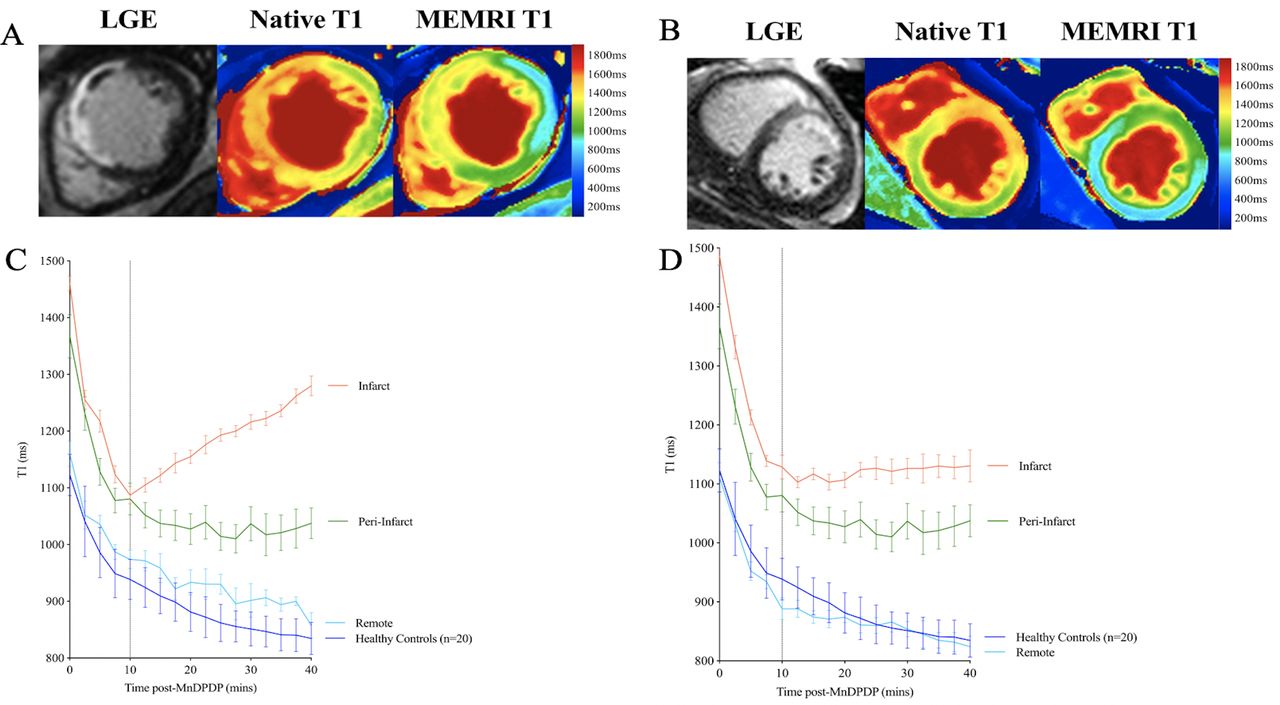
Manganese-enhanced MRI (MEMRI) in patients with myocardial infarction. Representative late gadolinium enhancement (LGE), native and MEMRI T1 mapping (A) and T1 profiles of myocardial regions of interest over time following manganese dipyridoxyl diphosphate (MnDPDP) (C) in a patient with extensive anterior myocardial infarction, compared with healthy control myocardium (n=20). Comparative representative LGE, native and MEMRI T1 mapping (B) and T1 profiles of myocardial regions of interest over time following MnDPDP (D) in a patient with subendocardial myocardial infarction, compared with healthy control myocardium (n=20). Dashed line represents end of infusion, error bars are SD of the mean.
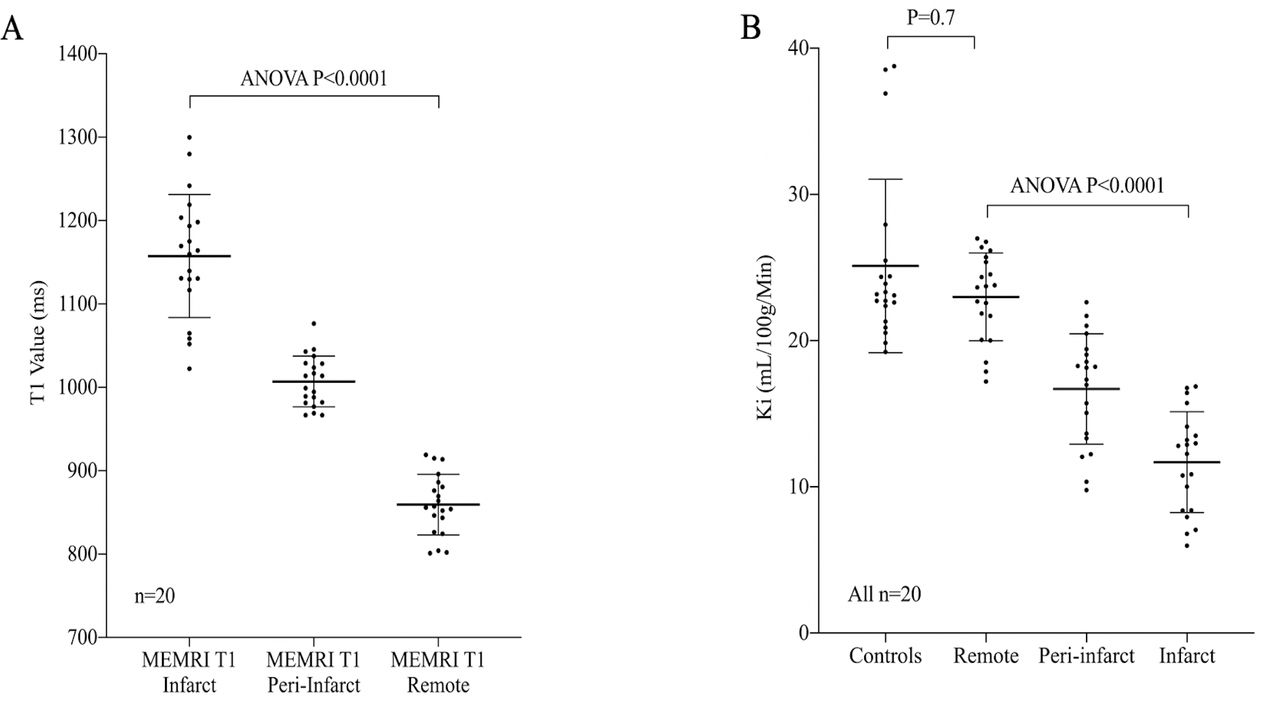
Across the entire cohort, MEMRI T1 values at 40 min were higher in regions of infarction compared with remote and healthy myocardium (1157±74 vs 859±36 and 835±28 ms; both p<0.0001). All infarct regions had MEMRI T1 >1000 ms, whereas remote and healthy myocardium had T1 <950 ms. An intermediate recovery profile and 40-minute MEMRI T1 value were demonstrated in peri-infarct regions (1007±31 ms), distinct from regions of infarction (1157±74 ms) and remote non-infarcted myocardium (859±36 ms; ANOVA p<0.0001, figure 3A).

Manganese-enhanced MRI (MEMRI) in myocardial regions of interest. MEMRI T1 values in patients with myocardial infarction (A) and influx constant (Ki), (B) in patients with myocardial infarction; infarct core, peri-infarct and remote myocardial regions of interest, compared with healthy control myocardium. ANOVA, analysis of variance.
Kinetic modelling of manganese uptake demonstrated stepwise reductions across remote, peri-infarct and infarcted myocardial regions, with absolute discrimination between the remote and infarcted myocardium (mean Ki 23.0±3.0, 16.7±3.8 and 11.7±3.5 mL/100 g/min; ANOVA p<0.0001, figure 3B). Rate of uptake between healthy control and remote non-infarcted myocardium was similar (23.1±3.6 and 23.0±3.0 mL/100 g/min; p=0.16), but uptake was slower in peri-infarct regions than remote myocardium (16.7±3.8 and 23.0±3.0 mL/100 g/min; p<0.0001).
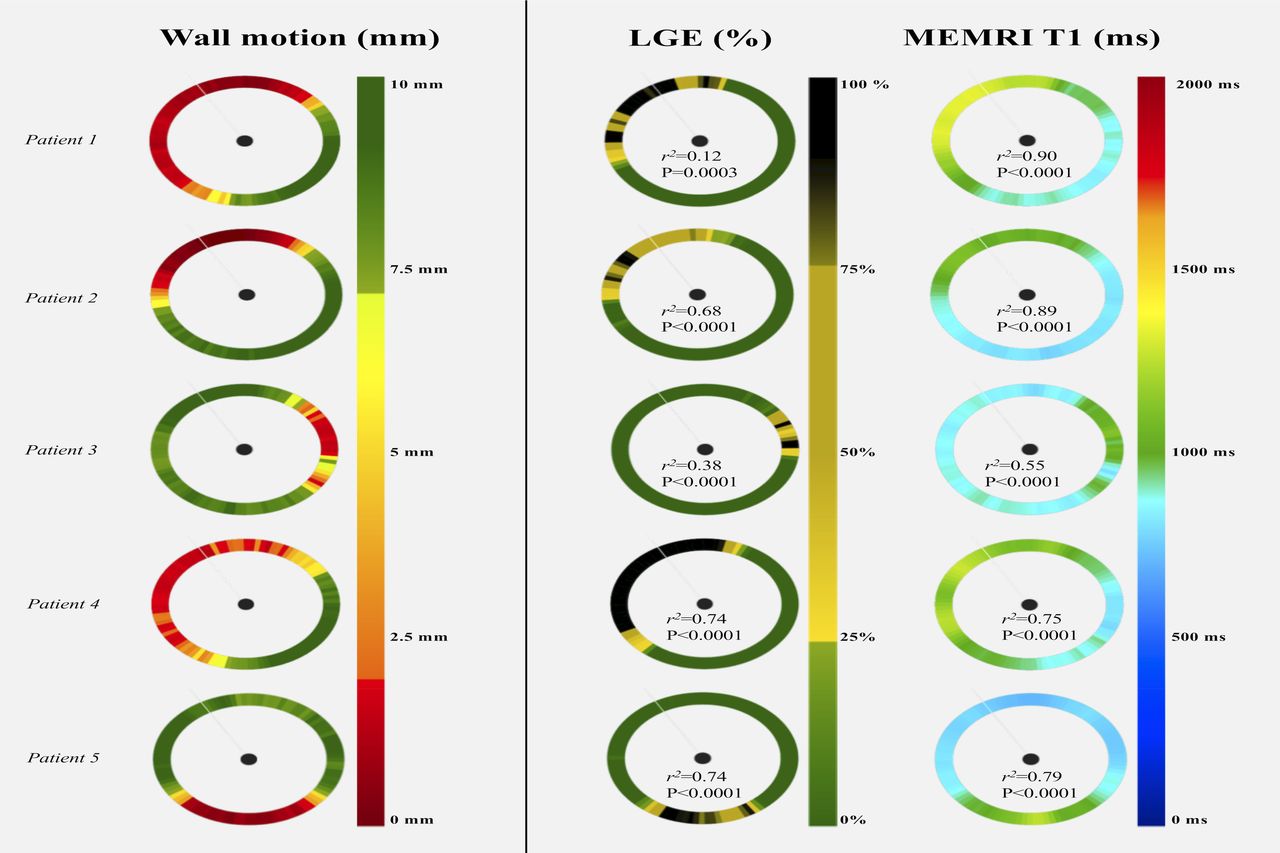
Compared with LGE, MEMRI was more sensitive than LGE in detecting dysfunctional myocardium (dysfunctional fraction 40.5±11.9 vs infarct size 34.9%±13.9%; p=0.02) but these two measures of myocardial injury correlated closely (r2=0.51, p=0.0004). When compared with wall motion, MEMRI T1 tracked more closely with abnormal wall motion, demonstrating superior correlation than LGE (mean r2=0.72 vs 0.55, p<0.0001; figure 4 and online supplemental figure S5).
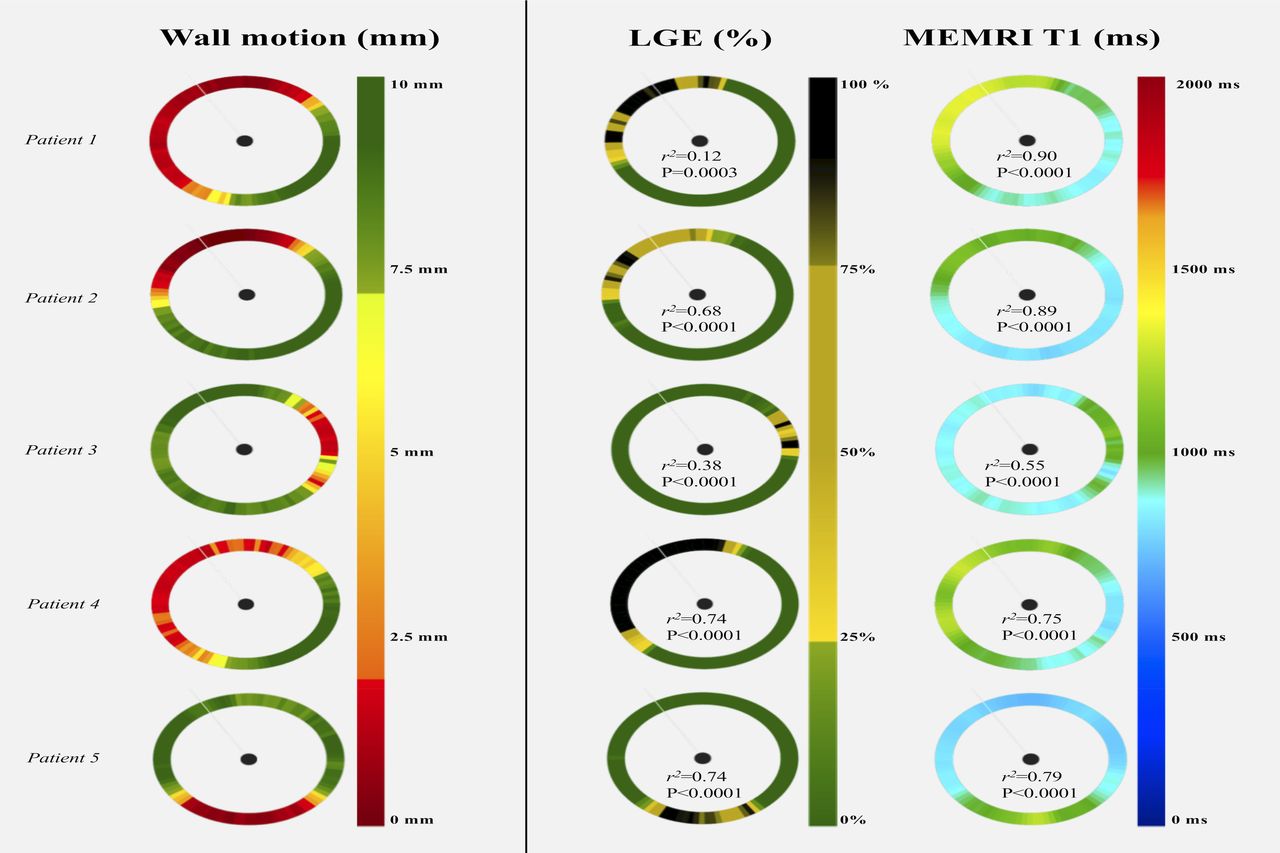
Wall motion, late gadolinium enhancement (LGE) and manganese-enhanced MRI (MEMRI) T1 mapping colour maps at the core infarct slice in five patients, represented as 100-chord plots (anterior right ventricle insertion as reference point). Values demonstrate stronger correlation between MEMRI T1 than LGE with reduced wall motion in every patient.
MEMRI in recovery phase following myocardial infarction
In the cohort of patients (n=14) who underwent repeat imaging 3 months after myocardial infarction, average ejection fraction had increased by 6.0% (p=0.0004) and LGE infarct size had decreased by 11.2% (p<0.0001). At the core infarct slice, functionally impaired myocardium by MEMRI was on average 13.4% lower at 3 months than baseline (p<0.0001) and was similar to LGE quantification (26.9±11.0 and 24.2%±6.5%; p=0.2). Both native and MEMRI T1 in the remote non-infarcted myocardium remained unchanged between acute and recovery phase imaging (both p>0.1).
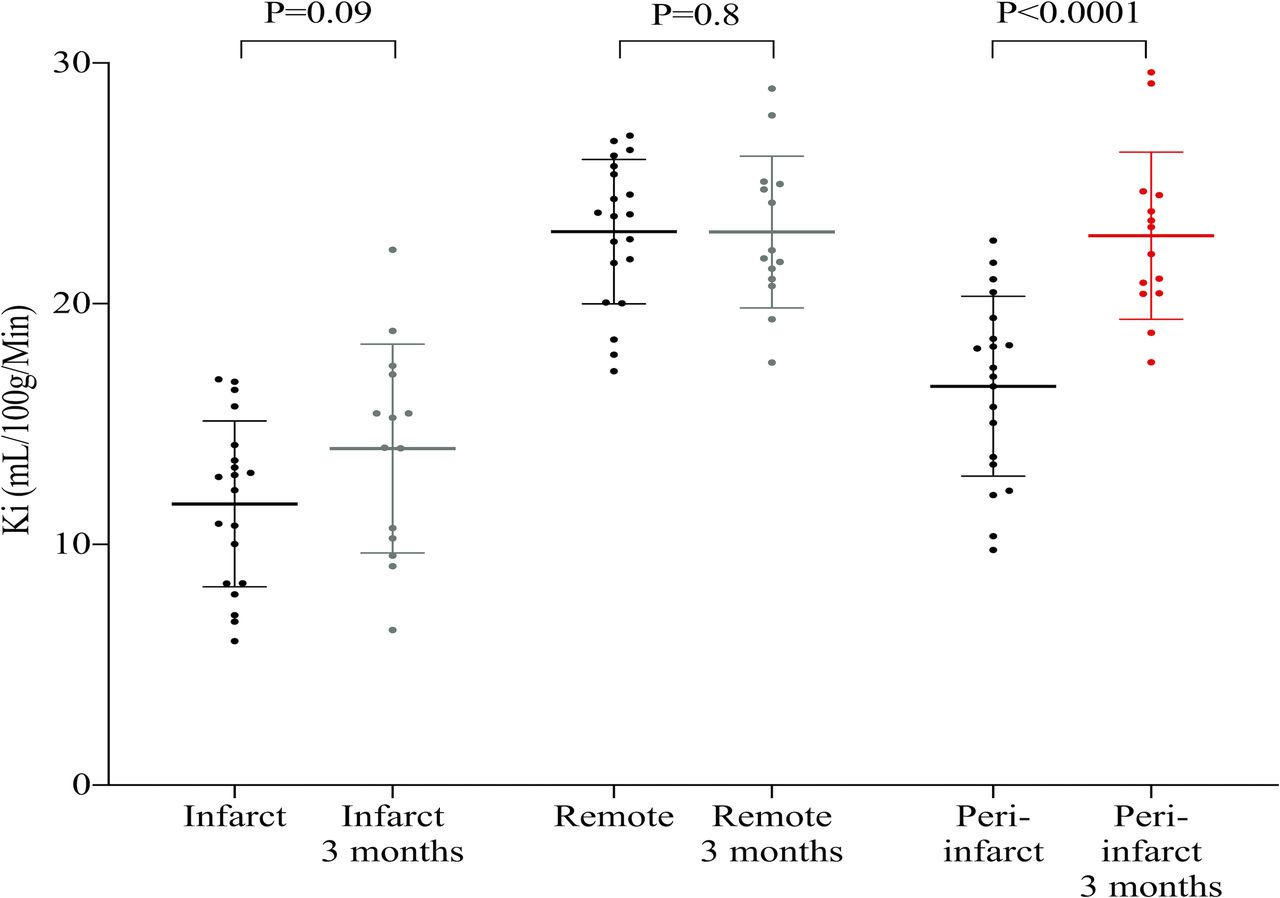
Using kinetic modelling, mean rate of manganese uptake was unchanged between early and late time points in both infarcted (11.5±3.7 vs 14.0±1.2 mL/100 g/min, p=0.1) and remote non-infarcted (23.3±2.8 vs 23.0±3.2 mL/100 g/min, p=0.8) myocardium. In peri-infarct regions, the rate of manganese uptake was increased (16.5±3.5 vs 22.8±3.5 mL/100 g/min, p=<0.0001; figure 5 and figure 6A,B) suggesting recovery in myocyte calcium handling. In contrast to acute phase imaging, peri-infarct regions and remote myocardium demonstrated similar manganese uptake rates after 3 months (22.8±3.5 and 23.0±3.2 mL/100 g/min; p=0.9; figure 6C).

Differential manganese uptake over time. Kinetic modelling of manganese uptake (Ki, influx constant) in patients with myocardial infarction; infarct core, peri-infarct and remote myocardial regions of interest, at acute (n=20) and 3-month (n=14) imaging time points.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Differential manganese uptake after myocardial infarction. Representative late gadolinium enhancement (LGE) and manganese-enhanced MRI (MEMRI) T1 mapping images (A) and Patlak plots (B) in a patient with myocardial infarction, demonstrating differential Ki (influx constant) between myocardial regions of interest over time. Grouped comparison T1 profiles for all patients and healthy control subjects (C). Dashed line represents end of infusion, error bars are SD of the mean. MnDPDP, manganese dipyridoxyl diphosphate.
Discussion
In this proof-of-concept study, we provide the first description of MEMRI T1 mapping to define viable and stunned myocardium in patients with acute myocardial infarction. Our study suggests that MEMRI can characterise and directly quantify viable myocardium, enabling it to be differentiated from infarcted and stunned myocardium. Furthermore, the kinetics of manganese uptake may provide a direct measure calcium handling within the myocardium. This latter property holds major promise for the future assessment of myocardial recovery as well as its potential application to other cardiac conditions associated with myocardial dysfunction and dysregulated calcium handling.
Manganese can be used to image tissues with calcium-dependent processes on account of its biophysical and kinetic properties as a paramagnetic calcium analogue.23 Following intravenous administration of MnDPDP, rapid biotransformation of the chelate occurs via dephosphorylation and transmetallation with zinc, enabling manganese to circulate as a bioavailable protein-bound complex that is readily accessible for intracellular uptake.23 24 Previous studies have demonstrated that manganese uptake is reduced in patients with ischaemic and non-ischaemic dilated cardiomyopathy.13 25 Furthermore, it correlates with left ventricular ejection fraction.20
As anticipated, MEMRI detected clear differences in T1 values of the myocardium following acute infarction compared with peri-infarct and remote regions. Altered kinetics of manganese enhancement exceeded the region of infarction defined by LGE but correlated more closely with abnormalities in wall motion. This is an extremely important distinction as this suggests that MEMRI is more specifically tracking myocardial dysfunction where LGE only defines the pathological extracellular space of infarcted or oedematous tissue. Furthermore, the changes in MEMRI T1 over 3 months after infarction may be attributable to alterations in calcium handling and uptake due to myocardial remodelling and recovery of cardiomyocyte function and contractility.
Within regions of extensive transmural myocardial infarction, the recovery of T1 values following infusion was similar to those seen in the blood pool. This recovery of T1 values suggests an absence of manganese uptake due to the presence of infarcted and non-viable tissue. The recovery of the T1 values was slower than the blood pool suggesting delayed clearance from the pathological extracellular space, similar to the mechanism by which gadolinium provides delayed enhancement. However, the plateau of T1 profile seen in patients with less extensive subendocardial myocardial infarction signifies that more complex contrast dynamics are at play. The plateau phase implies that some residual cardiomyocytes with viable calcium handling are present and is likely to represent a combined signal from both viable and non-viable cells within the wider infarct zone. Existing data suggest myocardial T1 shortening due to MnDPDP may persist several hours after administration25 and therefore as a proof-of-concept study, it was important to image at later time points to yield better discrimination between myocardial regions according to functional impairment.
The extent of T1 shortening in the remote myocardium of patients with acute infarction was similar to that seen in healthy volunteers. This indicates there are no major alterations in remote myocardial calcium-channel handling detectable with MEMRI in the early stages following myocardial infarction. In contrast, peri-infarct regions demonstrated reduced rates of manganese uptake, indicative of reduced function in stunned but non-infarcted regions. Indeed, kinetic modelling demonstrated a stepwise reduction in calcium-channel activity between remote, peri-infarct and infarct regions. Importantly, this reduction in manganese uptake in peri-infarct regions normalised after 3 months suggesting recovery of calcium handling by the stunned myocardium; a novel finding indicating MEMRI may be a sensitive tool in detecting myocardial viability. In this cohort of patients who underwent revascularisation for acute myocardial infarction, this ability to define viability by rate of calcium handling through the direct marker of manganese uptake could enable more accurate delineation of viable territories.
What are the clinical implications of MEMRI? In this study, we have undertaken the first T1 mapping investigation of MEMRI and have shown that it can identify viable myocardium and delineate it from infarcted as well as dysfunctional myocardium. Furthermore, for the first time, we have demonstrated that MEMRI can detect recovery of stunned myocardium within the peri-infarct zone following reperfusion. We, therefore, suggest that this technique has potential utility in detecting hibernating myocardium, which could prove an invaluable tool in patient selection for revascularisation therapies. Moreover, it holds particular promise as a biomarker of treatment efficacy for interventional strategies targeting ischaemia-reperfusion injury. With further study and optimisation of imaging time points, shorter imaging protocols will mean cardiac MEMRI assessment may offer a novel practical assessment of myocardial viability in clinical setting.
Historically, there have been concerns that manganese-based contrast media could cause acute myocardial suppressant effects. Early animal studies used unchelated manganese chloride which caused negative inotropy and cardiovascular instability. In contrast, dipyridoxyl diphosphate chelates manganese and thereby markedly reduces free unbound manganese ions. To date, MnDPDP is the only manganese-based contrast agent which has been approved for clinical use as a liver-specific contrast agent.22 It was marketed as Teslascan but was removed from the US market in 200326 and subsequently from the European Union market in 201027 because it was not commercially viable. In the present study which included patients with acute myocardial infarction and the previous study by Skjold et al,16 20 25 MnDPDP was well tolerated in all subjects with no adverse events reported. This manganese-based contrast medium, therefore, appears safe and well tolerated. Given the resurgence of interest in this area, various companies are actively exploring re-marketing MnDPDP for clinical use.
Our study has some limitations. First, patients were recruited following primary percutaneous coronary intervention for acute myocardial infarction, which enabled the first evaluation of MEMRI in acute infarction. However, we did not exclusively recruit patients with single vessel disease or those with a first event. The presence of old infarction could have influenced the extent of recovery and our findings are therefore likely to be conservative. Second, LGE and MEMRI scans were performed 48 hours apart and, due to the dynamic nature of the infarct characteristics during the first week postrevascularisation, this may mean that the extent of contrast enhancement may have changed. To account for this, we randomised the order of scans which should eliminate any systematic bias in infarct size between LGE and MEMRI and measured oedema and LGE at the same time point in keeping with current consensus.7 A recent consensus suggested optimal imaging at 5±2 days after myocardial infarction.28 Due to the need to stagger MEMRI and LGE scans by 48 hours, we selected 3±2 days in order to achieve this. Third, MnDPDP is currently not readily or widely available for clinical use although we anticipate that this is likely to change following the demonstration of its clinical and research utility. For the present study, we sourced a formulation of clinical grade MnDPDP. Fourth, our current MEMRI protocol lasts over 40 min which in a clinical setting may be challenging. However, this was a proof-of-concept study and we are currently exploring more rapid protocols to improve practical implementation. Fifth, we cannot rule out that calcium handling deteriorates with age and, because control subjects were younger, this could explain some of the observed reductions in manganese uptake. However, we found no correlation between age and manganese uptake in the healthy volunteers or our patient cohort (data not shown, R2=0.006, p=0.74) and this would not explain the temporal changes in uptake seen in patients recovering from myocardial infarction. Finally, the small sample size of this pilot study warrants large scale translation.
In conclusion, we have described the first proof-of-concept T1 mapping study of MEMRI in healthy volunteers and patients with acute and recovering myocardial infarction. Using kinetic modelling, we have shown that MEMRI not only more accurately quantifies areas of myocardial dysfunction following ischaemic injury but can directly identify viable as well as recovering stunned myocardium. We believe that MEMRI holds major promise for early detection and quantification of myocardial stunning and viability, with the potential for improved patient selection for revascularisation and novel therapeutic interventions for myocardial recovery. Finally, its application to other areas of disorders of myocardial calcium handling warrants further investigation.
Data availability statement
All data relevant to the study are included in the article or uploaded as online supplemental information.
Ethics statements
Ethics approval
The study was carried out in accordance with the Declaration of Helsinki, the approval of the local Research Ethics Committee (17/SS/0055) and the written informed consent of all participants.
Acknowledgments
Grateful acknowledgements are made to Siemens Healthineers for provision of the ShMOLLI WIP used in this study.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors NBS, DEN and SS conceived and designed the study; NBS recruited and scanned all patients, analysed the data, performed kinetic modelling and compiled the original manuscript; GP wrote and validated the code for kinetic modelling; TS, DEN, GPM, MRD, AB, RJJ, LK and SS contributed to revision and critical appraisal of the final manuscript for important intellectual content. All authors approved the final manuscript submitted.
Funding This work and NBS, TS, AB, MRD and DEN are supported by the British Heart Foundation (FS/17/19/32641, FS/14/78/31020, CH/09/002, RG/16/10/32375, RE/18/5/34216, RG/20/5/34796). DEN is the recipient of a Wellcome Trust Senior Investigator Award (WT103782AIA). The Edinburgh Clinical Research Facilities and Edinburgh Imaging facility is supported by the National Health Service Research Scotland (NRS) through National Health Service Lothian Health Board.
Competing interests SIS has a consultancy agreement with GSK. DEN and SIS hold unrestricted educational grants from Siemens Healthineers.
Provenance and peer review Not commissioned; externally peer reviewed.