Article Text

Abstract
Objective We assessed the influence of the ischaemic burden (IB) as derived from vasodilator stress cardiovascular magnetic resonance (CMR) on the risk of death and the effect of revascularisation across sex.
Methods We evaluated 6237 consecutive patients with known or suspected chronic coronary syndrome (CCS). Extensive ischaemia was defined as >5 segments with perfusion deficit. Multivariate Cox proportional hazard regression models were used.
Results A total of 2371 (38.0%) patients were women and 583 (9.3%) underwent CMR-related revascularisation. During a median follow-up of 5.13 years, 687 (11.0%) deaths were reported. We found an adjusted differential effect of CMR-derived IB across sex (p value for interaction=0.039). Women exhibited an adjusted lower risk of death and only equaled men’s risk when extensive ischaemia was present. Likewise, CMR-related revascularisation was shown to be differentially associated with the risk of mortality across sex (p value for interaction=0.025). In patients with non-extensive ischaemia, revascularisation was associated with a higher risk of death, with a greater extent in women. At higher IB, revascularisation was associated with a lower risk in men, with more uncertain results in women.
Conclusions CMR-derived IB allows predicting the risk of death and gives insight into the potential effect of revascularisation in men and women with CCS. Compared with men, women with non-extensive ischaemia displayed a lower risk and a similar risk with a higher IB. The impact of CMR-related revascularisation on mortality risk was also significantly different according to IB and sex. Further research will be needed to confirm these hypothesis-generating findings.
- MRI
- chest pain
- percutaneous coronary intervention
- coronary artery bypass
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known about this subject?
The benefit of coronary revascularisation in patients with chronic coronary syndrome (CCS) and the role of myocardial ischaemia in the decision-making process are matters of constant debate.
In this same cohort of patients with CCS, our group recently reported that ischaemic burden (IB) as derived from vasodilator stress cardiovascular magnetic resonance (CMR) predicted long-term all-cause mortality, and revascularisation exerted a protective effect only in those with extensive ischaemia.
What does this study add?
In this historical cohort of patients with known or suspected CCS, women had a lower risk of death along most of the IB spectrum. In those with extensive ischaemia, the risk in women equalled the risk of men.
The risk attributable to CMR-related revascularisation was less favourable in women. At lower IB, revascularisation showed a higher risk of death in women, while at greater IB, revascularisation effect was more uncertain in women.
How might this impact on clinical practice?
Our results, although should be considered hypothesis-generating, suggest a more conservative attitude in patients with CCS with non-extensive IB, especially in women, as the benefit of revascularisation is less clear in women, even for higher degrees of ischaemia.
Introduction
Vasodilator stress cardiovascular magnetic resonance (CMR) has become a pivotal tool for diagnosis in chronic coronary syndrome (CCS). Moreover, since it allows a comprehensive evaluation of patients with stable ischaemic heart disease (IHD), its value for risk stratification has been well documented, and its potential in decision-making has been suggested.1–3
In the same cohort of patients with CCS used for the present analysis, our group recently reported that ischaemic burden (IB) as derived from vasodilator stress CMR predicted long-term all-cause mortality revascularisation exerted a protective effect only in those with extensive ischaemia.4 However, in this clinical scenario, little is known about the possible differential prognostic impact of IB and the effect of subsequent revascularisation across sex. It is particularly relevant given the well-established pathophysiological sex differences in IHD.5–7
In this substudy, we retrospectively evaluated, in a large registry of unselected patients with known or suspected CCS referred for vasodilator stress CMR, sex differences in: (a) the effect of the IB on long-term all-cause mortality and (b) the effect of revascularisation along the continuum of the IB on long-term all-cause mortality.
Methods
Study population
This study was based on a large registry that included 6700 consecutive patients referred for vasodilator stress CMR for known or suspected CCS in our health department from 2001 to 2016.1 2 4 Baseline characteristics and CMR data were prospectively recorded and immediately entered into the predefined database. To avoid missing values and maximise data collection’s robustness, only the limited number of variables shown in table 1 was defined in the database. The referring cardiologists indicated CMR as part of routine medical practice, had full access to all CMR parameters, and patients’ management was left to their discretion. After excluding the cases with incomplete baseline data, lost follow-up, cardiomyopathy, incomplete or insufficient CMR image quality, the final study group was made up of 6237 patients (see flow-chart in online supplemental figure 1).
Supplemental material
Baseline characteristics
Reasons for vasodilator stress CMR referral were as follows: evaluation of ischaemia and myocardial viability (29%), follow-up of previous revascularisation (23%), the first option in the workup of patients (19%), inconclusive exercise ECG test (13%), inability to exercise (13%), evaluation of intermediate coronary lesions (2%) and altered baseline ECG (1%).4
CMR data analysis
Technical aspects related to CMR studies are depicted in online supplemental file 1 and elsewhere.1 3 8 Images were examined using customised software (Syngo, Siemens, Erlangen, Germany).
Supplemental material
Left ventricular end-diastolic and end-systolic volume indexes and left ventricular ejection fraction (LVEF) were quantified in cine images. Ischaemia was visually defined, using the 17-segment model,9 as the presence of a segmental perfusion deficit (PD), determined as a persistent delay (in at least three consecutive temporal images, in comparison with other segments in the same slice) during the first pass of contrast through the myocardium after vasodilator infusion. IB was defined as the number of segments that showed post-stress PD. The presence of stress-induced PD was ruled out in segments exhibiting transmural late gadolinium enhancement (LGE) and segments with simultaneous PD and non-transmural LGE in which the extent of PD did not clearly exceed the extent of LGE. The IB was also analysed as a continuous variable and dichotomised in non-extensive (≤5 segments) and extensive (>5 segments with PD). This cut-off value was derived from this same series of patients based on predicting all-cause death in the entire population.4 LGE extent was visually defined as the number of segments with LGE. The ischaemic cascade was categorised into three groups defined, according to the sequential occurrence of PD and abnormal wall motion (AWM), in a three-category variable: IC1 (no evidence of ischaemia, normal perfusion study and no inducible AWM), IC2 (PD but no inducible AWM) and IC3 (inducible AWM regardless of PD).10
Interobserver and intraobserver variability for all parameters used in the present registry is <5% and have been previously reported.4
CMR-related revascularisation
CMR-related revascularisation was defined as those procedures (either coronary artery bypass grafting or percutaneous coronary intervention) performed within 3 months following the index vasodilator stress CMR study, as long as no hospital admission for cardiovascular indications occurred during that period (in this case, patients were censored after readmission).
Endpoint and follow-up
The clinical endpoint was all-cause mortality. Follow-up was centrally carried-out from October 2018 to November 2018 by four cardiologists authorised by the local ethics committee using the unified electronic regional health system registry.
Statistical analysis
Continuous variables are presented as mean (±SD) or median (IQR), as appropriate. Categorical variables are expressed as percentages. Baseline continuous variables were compared according to sex using the Student’s t-test or Wilcoxon rank-sum test, as appropriate. Discrete variables were compared using the χ2 test.
The association of variables with time to all-cause mortality was assessed using multivariate Cox proportional hazard regression models. HRs with the corresponding 95% CIs were computed. The proportional hazards assumption based on Schoenfeld’s residuals was considered accomplished if the p value was >0.05. The cumulative risk for death during follow‐up was estimated using the Kaplan‐Meier method and tested with the log-rank test. The IB was analysed as a continuous variable and dichotomised in non-extensive (≤5 segments) and extensive (>5 segments with inducible PD). This cut-off value was recently validated in this same series of patients based on its ability to predict all-cause death in the entire population.4 In this previous work, we used the Youden index applied to the receiver operating curve analysis to predict all-cause mortality; >5 ischaemic segments was the best cut-off value to predict the occurrence of all-cause mortality and the effect of CMR-related revascularisation on this event.
All variables listed in table 1 were tested based on prior knowledge/biological plausibility in the multivariate models, independent of the p value. We simultaneously tested the linearity assumption for all continuous variables, and the variables were transformed with fractional polynomials when appropriate. Next, we derived a reduced and parsimonious model by using backward step-down selection. The covariates included in the final models were age, hypertension, dyslipidaemia, diabetes, smoking, family history of IHD, CMR-assessed LVEF and previous revascularisation. Harrell’s C-statistics of the model, including the interaction sex×IB as the exposure was 0.745. The model, including the interaction revascularisation×sex and the IB showed a Harrell’s C-statistics of 0.746.
A two-tailed p value of <0.05 was statistically significant in all analyses. All survival analyses were performed using STATA V.15.1 (StataCorp, 2017: Release 15).
Results
The mean age of the sample was 65±11 years, 2371 (38.0%) patients were women, 2357 (37.8%) had previous IHD and 1481 (23.7%) were previously revascularised. The IB was severe in 1006 (16.1%) patients (table 1).
Baseline characteristics according to gender
Table 1 presents the baseline characteristics according to sex. Overall, women were older, with a higher prevalence of traditional cardiovascular risk factors (hypertension and dyslipidaemia). Conversely, men were more often smokers and presented a higher prevalence of previous IHD, including a higher percentage of myocardial infarction and revascularisation procedures. Regarding CMR parameters, men had lower LVEF values, higher left ventricle volumes and a greater IB, with more segments with PD and LGE (table 1). In those in which angiography data were available (N=1066 patients), the greater number of vessels with severe CAD identified patients with a greater IB in both sexes (p<0.001 for all comparisons), but without differences between sexes (table 1). Online supplemental table 1 shows the baseline characteristics according to IB and sex. Briefly, in those with non-extensive ischaemia, women had more frequently hypercholesterolaemia and hypertension. At the same time, there were no differences in those with extensive ischaemia.
Supplemental material
IB and risk of mortality: the role of sex
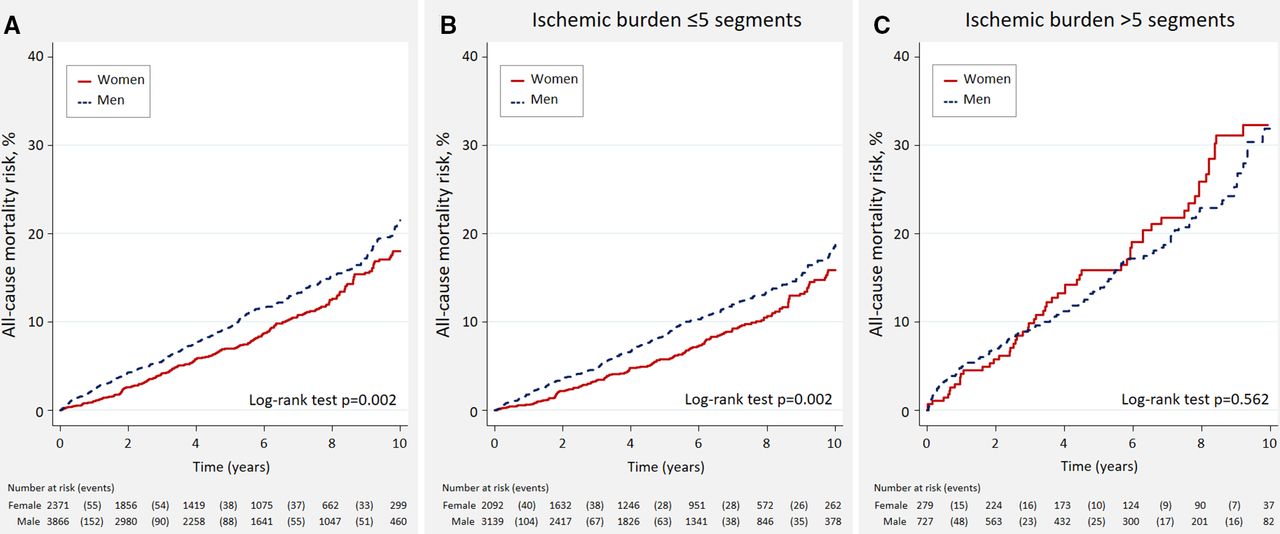
During a median follow-up of 5.13 (2.26–8.29) years, 687 (11.0%) deaths were ascertained. The death rates were higher in men versus women (2.21 vs 1.73 per 100 person/years, p=0.002), with differences found during the entire follow-up (figure 1A). When the results were stratified by the IB (non-extensive vs extensive), women showed lower mortality rates when ischaemia was non-extensive (1.92 vs 1.44 per 100 person/years, p=0.002). When extensive ischaemia was present, the rates were not significantly different between men and women (3.48 vs 3.84 per 100 person/years, p=0.562). Kaplan-Meier curves confirmed that these prognostic differences were present during the whole follow-up in both sexes (figure 1B,C).
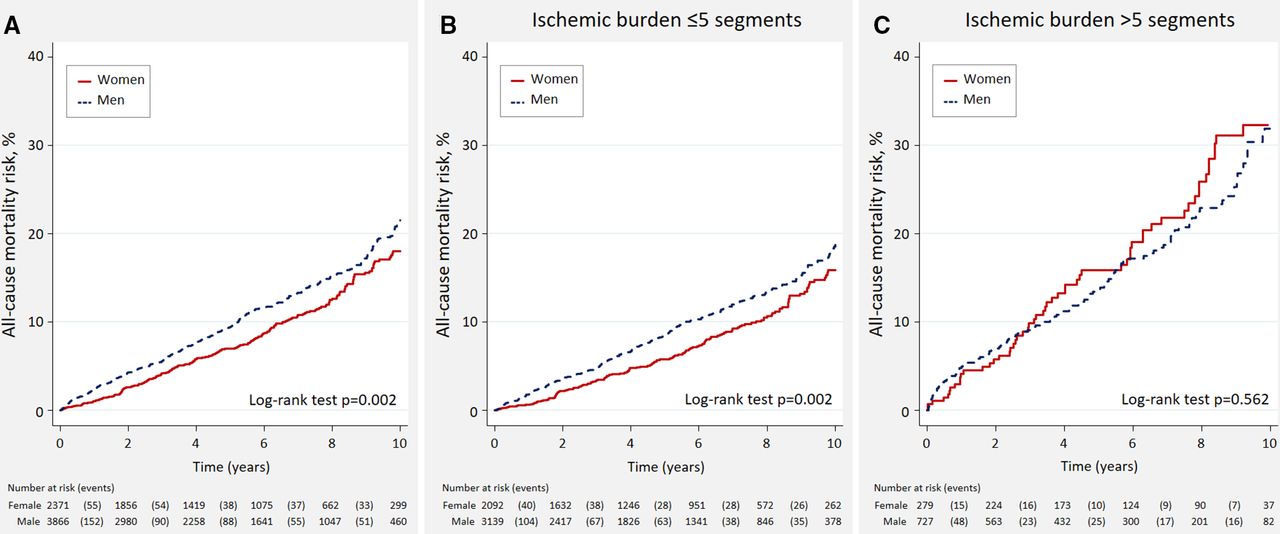
All-cause mortality risk across ischaemic burden (IB) and sex. (A) All patients. (B) Patients with CMR-derived non-extensive IB. (C) Patients with CMR-derived extensive IB. CMR, cardiovascular magnetic resonance.
Multivariate analysis confirmed a significantly lower mortality risk in women along the continuum of IB except for those with the most extensive ischaemia, in which the risk of mortality was similar in both sexes (p value for interaction=0.039). The corresponding HRs for women versus men along the continuum of IB are presented in figure 2. This differential adjusted effect also persisted when the IB was classified as extensive and non-extensive (p value for interaction=0.022). Women with non-extensive IB showed a lower risk of all-cause mortality (HR=0.66, 95% CI 0.54 to 0.80; p<0.001), with no significant differences between men and women in those with an extensive IB (HR=1.00, 95% CI0.74 to 1.36; p=0.987).

Excess of mortality risk in men versus women across cardiac magnetic resonance ischaemic burden. Compared with women, men showed a higher risk of death when non-extensive ischaemia was present. In patients with extensive ischaemia, women had the same risk as men. CMR, cardiovascular magnetic resonance.
Mortality risk associated with revascularisation across sex and IB
CMR-related coronary angiography and revascularisation procedures were performed in 1113 (17.8%) and 583 (9.3%) patients. CMR-related coronary angiographies were more frequent in men without ischaemia or low IB (0–1 segments). On the contrary, it was performed more frequently in women with 2–5 ischaemic segments, without differences were >5 segments (online supplemental figure 2). Likewise, related revascularisation procedures were more frequent in men with 0–1 PD segments, without differences between sexes at greater IB (online supplemental figure 3).
Supplemental material
Supplemental material
In patients with non-extensive ischaemia, mortality rates were higher in those revascularised (3.12 vs 1.64 per 100 person/years, p<0.001). Conversely, revascularisation was associated with lower mortality rates in patients with extensive ischaemia (2.79 vs 3.87 per 100 person/years, p=0.036). However, mortality risk related to CMR-related revascularisation status differed across sex and IB (figure 3). Kaplan-Meier curves showed that revascularisation was associated with worse outcomes in both sexes in patients with non-extensive ischaemia (figure 3A,B). In those with extensive ischaemia, revascularisation was associated with a lower risk in men but not in women (figure 3C,D).

All-cause mortality risk across ischaemic burden (IB) and sex. (A) Men with non-extensive IB. (B) Women with non-extensive IB. (C) Men with extensive IB. (D) Women with extensive IB. CMR, cardiovascular magnetic resonance; Rev, cardiovascular magnetic resonance-derived revascularisation.
Under the multivariate setting, the sex-differential prognostic impact of related revascularisation along the IB was also confirmed (p value for interaction=0.019). In women, revascularisation was associated with a higher risk of mortality in those with ≤5 segments with PD. With a greater IB, the effect was neutral (figure 4A). In men, the deleterious effect of revascularisation was mainly found when the IB was ≤2 segments and a trend to positive impact with greater ischaemia (figure 4B).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Related coronary angiography and revascularisation procedures. (A) Related coronary angiography procedures. (B) Related revascularisation procedures. CMR, cardiovascular magnetic resonance.
When ischaemia was categorised in extensive versus extensive (<5 vs ≥5 segments), this differential association was also confirmed (p value for interaction=0.025). In patients with non-extensive ischaemia, revascularisation was associated with a higher risk of death in women (HR=2.20, 95% CI 1.25 to 3.89; p=0.007) and men (HR=1.60, 95% CI 1.12 to 2.27; p=0.009). When extensive ischaemia was present, revascularisation was associated with a statistical trend to lower risk in men (HR=0.67, 95% CI 0.43 to 1.03; p=0.072) but a neutral effect in women (HR=1.03, 95% CI 0.58 to 1.83; p=0.913).
Adjusted analyses also revealed a sex-differential impact of revascularisation in the three categories of the ischaemic cascade (p value for interaction=0.007). In patients in C1 revascularisation was associated with a greater risk in women (HR=3.67, 95% CI 0.91 to 14.9) than men (HR=2.08, 95% CI 1.12 to 3.87). On the contrary, in those belonging to C3 revascularisation was neutrally associated with the risk of death in women (HR=1.36, 95% CI 0.95 to 1.95) but protective in men (HR=0.53, 95% CI 0.30 to 0.91).
Discussion
In this large registry, including 6237 subjects with known or suspected CCS who underwent vasodilator stress CMR, significant sex-related prognostic differences were found. Overall, the risk of death was lower in women along most of the IB spectrum, except for patients with extensive ischaemia, in which women equalled the risk of men. We also found a sex-differential prognostic association along the continuum of IB. Overall, at lower IB, revascularisation was associated with a higher risk in women than men. At greater IB, revascularisation identified a subset of men with lower risk and more uncertain effect in women (online supplemental graphical abstract).
Supplemental material
Sex differences in stable IHD
There are well-known sex-related pathophysiological differences in IHD.5–7 11 Women are affected by IHD, on average, 7–10 years later than men, which has mainly been attributed to the protective effects of oestrogens during reproductive years.5 Non-coronary acute chest pain, non-obstructive coronary artery disease (CAD) and non-atherosclerotic disease are more frequent in women with acute chest pain.6 7 In fact, almost two-thirds of women with persistent symptoms and clinical signs of ischaemia have no significant obstructive CAD (INOCA) on angiography, versus only one-third in men.6 7
In a substudy of the Bypass Angioplasty Revascularization Investigation 2 Diabetes (BARI-2D) trial, which included patients with CCS and diabetes, women, compared with men, had more symptoms and less anatomic CAD at baseline, with persistent higher rates of angina after 5 years of medical therapy with or without prompt revascularisation.12 More recently, Reynolds et al reported, in a substudy of the ISCHEMIA trial, that women had more frequent angina, independent of less extensive CAD and less severe ischaemia than men, reflecting inherent sex differences in the complex relationships between angina, atherosclerosis and ischaemia.13
Differential prognostic implications of ischaemia in women with CCS
The predictive value of CMR-derived ischaemia in patients with known or suspected CAD has been well-established.1–4 However, the evidence of different prognostic implications across gender is still scarce. In this regard, Coelho-Filho et al14 found that CMR-derived myocardial ischaemia was strongly associated with the risk of major adverse cardiovascular events regardless of sex in 405 patients (41.5% women) referred for ischaemia assessment. However, the number of patients (168 women) and events (21 cardiac deaths and 15 acute myocardial infarctions) was low to test potential sex-differential findings robustly. As expected, our results show that a more extensive stress-CMR-derived ischaemia is associated with a higher risk of death in both sexes. However, sex maybe modifies this risk. In general, women had a lower risk when non-extensive ischaemia was present. However, the risk was similar with a greater IB. We speculate there might be some mechanisms behind these findings.
(a) First, men and women had different cardiovascular risk profiles. Although women exhibited a worse ‘baseline clinical profile’ in terms of older age and a greater burden of traditional cardiovascular risk factors, men showed a poorer ‘structural profile’ including more frequent previous IHD and more severe structural heart disease (including a lower LVEF, larger left ventricular volumes and more extensive ischaemic and necrotic burden), which may explain in part the worse prognosis of men in the whole sample. However, in patients with extensive (>5 segments) ischaemia, the baseline clinical differences among men and women almost vanished, and, in this setting, the structural profile of women was more deteriorated. This observation is in line with the results recently published by Peters et al,15 showing in a large series of insurance beneficiaries with suspected IHD in the USA that the lower mortality observed in women was attenuated in those cases with previous myocardial infarction. Thus, it can be speculated that in women without or with non-extensive IB, despite their worse baseline profile, the absence of severe structural damage exerts some degree of protective effect. (b) Second, the pathophysiology of CCS is different in women and men.5–7 Unlike men, in which atherosclerotic epicardial CAD is the most frequent anatomic form of CCS, the incidence of non-obstructive CAD (INOCA), including microvascular dysfunction,6 7 is higher in women. Although INOCA-related conditions are associated with an increased risk of complications, this is lower than reported for those with epicardial CAD. Thus, we postulate that the higher prevalence of microvascular dysfunction and other non-typical atherosclerotic diseases may explain the lower risk shown by women along most of the continuum of IB. Probably, severe ischaemia in women identified a subgroup with a higher odds of proximal or multivessel obstructive CAD.
Sex-mortality differences across revascularisation in CCS
Current evidence does not support a survival benefit of revascularisation in CCS.8 16 17 However, whether some subgroups benefit from an intensive revascularisation strategy remains controversial.18–20
In this study, we observed that revascularisation procedures in men without extensive ischaemia almost doubled the rate detected in women. A perception regarding a higher risk of IHD and cardiac events in men and a tendency to not trust negative stress CMR in male patients might partially underly these differences in management. Indeed, we recently reported, in the same cohort, that CMR-related revascularisation in patients with non-extensive ischaemia associates with a higher risk of all-cause mortality.4 Thus, gender bias towards more revascularisation in men without ischaemia could contribute to the excess of mortality (in absolute terms) in men in this setting.
At lower IB, the potentially harmful effect of revascularisation was also present in women and, in relative terms, was even more evident than in men. Microvascular angina,21 22 and intermediate CAD23 24 are more prevalent in women. In this setting, unnecessary coronary revascularisation may lead to a higher probability of adverse events.
On the other hand, at a greater IB, the beneficial association between revascularisation and mortality observed in men could not be confirmed in women. Even though we cannot unravel these findings’ underlying mechanism, we may speculate on some explanations. First, women with severe ischaemia were older and showed a worse clinical profile trend than men, which might diminish the potential beneficial effect of revascularisation. On the other side, some anatomic characteristics of obstructive CAD in women (small vessels, distal disease, etc) might confer worse revascularisation outcomes and a higher risk of side effects.25 26
Clinical implications
We envisioned potential clinical implications derived from these findings. First, in stable outpatients with known or suspected CCS, we found a lower risk of mortality in women regardless of the IB. Stress CMR yields an accurate and individualised diagnosis and risk stratification. This information may be provided to patients to mitigate the harmful psychological consequences (anxiety, depression) related to the uncertainty about the symptoms’ clinical and prognostic implications. Second, in this setting, our results suggest that more conservative decision-making approaches should be considered in patients with non-extensive ischaemia, especially in women, avoiding inappropriate revascularisation, especially in cases with a low IB and some uncertainties about the severity of CAD.
Limitations
Some limitations are worth mentioning. First, this is a retrospective single-centre study in which several unmeasured confounders might play a crucial role. For instance, we did not assess the characteristics or severity of symptoms, anatomic data from coronary angiography, or medical treatment. Due to the limitations of the design of this study, the results obtained should be considered as hypothesis-generating findings. Second, the cut-off point used to define extensive IB was previously validated by our group to predict all-cause mortality and the effect of CMR-related revascularisation on this endpoint.4 This value would represent >30% of ischaemic myocardium if crudely transformed in percentage of left ventricle mass. Nevertheless, this percentage should be interpreted with caution: the transmural extent of PD was not quantified and, consequently, the correct interpretation of the presented data must adhere to the units used for quantifying the extent of ischaemic myocardium, namely number of segments with inducible PD. Third, we did not evaluate other adverse outcomes such as the cause of death, symptom relief, unplanned revascularisation procedures or the occurrence of acute coronary syndromes. The evaluation of these endpoints is likely to contribute to a more holistic vision of the potential sex-differential clinical implication of the IB and revascularisation in CCS. This study was designed to include many cases over a long period and, for the sake of simplicity, the database was designed with a limited number of variables to minimise missing values and guarantee inclusion. Therefore, a variety of relevant collateral analyses are now unfeasible. Finally, the low proportion of patients analysed at greater IB, especially in women, may explain the uncertainty about the role of revascularisation in this subgroup of patients.
Conclusions
In this unselected cohort of patients with known or suspected CCS, women showed a lower risk of long-term all-cause mortality with a lower IB and no differences when extensive ischaemia was present. Revascularisation was associated with a higher risk of long-term mortality with a lower IB, this association being in relative terms more robust in women. With a greater IB, revascularisation was associated with a trend to decrease the risk in men but with a more uncertain effect in women. Further research is warranted to confirm these hypothesis-generating findings.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Ethics approval
This registry was carried out in accordance with the Declaration of Helsinki. In September 2018, the local ethics committee (Comité Ético de Investigación Clínica del Hospital Clínico Universitario de Valencia) authorised a retrospective update of the occurrence of all-cause mortality. More details about this registry can be consulted elsewhere.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @gema_minana, @vic__marcos
GM and JN contributed equally.
Contributors GM and JN: conceptualisation; formal analysis; funding acquisition; investigation; methodology; project administration; validation; visualisation and writing - original draft. VB: funding acquisition; investigation; methodology; project administration; validation; visualisation; project administration; resources; software and writing - review and editing. JVM, MPL-L, JG, VM-G, CR-N, NP, EdD and AF-C: data curation; investigation; methodology; resources; software and writing - review and editing. EN: data curation; formal analysis; investigation; methodology; software; validation; visualisation and writing - review and editing. FJC and JS: funding acquisition; investigation; resources; software; validation; visualisation and writing - review and editing.
Funding This study was supported by the Instituto de Salud Carlos III and co-funded by the European Regional Development Fund (ERDF) (grant numbers PI20/00637, CIBERCV16/11/00486).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.