Article Text

Abstract
Backgrounds Earlier studies showed that in patients with heart failure (HF), circulating levels of B-type natriuretic peptide (BNP) at hospital discharge (BNPdis) are more predictive of prognosis than BNP levels on admission (BNPad). However, the mechanism underlying that difference has not been fully elucidated. We examined the association between confounding factors during hospitalisation and BNPdis in patients with HF.
Methods We identified patients admitted to our hospital for HF (BNPad ≥100 pg/mL). Estimated left ventricular end-diastolic pressure (eLVEDP) was calculated using echocardiographic data. To identify the factors associated with the relation between BNPad and BNPdis, we performed a stepwise regression analysis of retrospective data. To validate that analysis, we performed a prospective study.
Results Through stepwise regression of the patient data (n=688, New York Heart Association 3–4, 88%), we found age, blood urea nitrogen and eLVEDP to be significantly (p<0.05) associated with BNPdis. Through multivariate analysis after accounting for these factors, we created a formula for predicting BNP levels at discharge (predicted-BNPdis) from BNPad and other parameters measured at admission (p<0.05). By statistically adjusting for these factors, the prognostic power of BNPad was significantly improved (p<0.001). The prospective study also confirmed the strong correlation between predicted-BNPdis and BNPdis (n=104, r=0.625, p<0.05).
Conclusion This study showed that statistically accounting for confounding factors affecting BNP levels improves the predictive power of BNP levels measured at the time of hospital admission, suggesting that these confounding factors are associated with lowering predictive power of BNP on admission.
Trial registration number UMIN 000034409, 00035428.
- heart failure
- biomarkers
- heart failure
- diastolic
- heart failure
- systolic Pl
Data availability statement
No data are available.
This is an open access article distributed in accordance with the Creative Commons Attribution 4.0 Unported (CC BY 4.0) license, which permits others to copy, redistribute, remix, transform and build upon this work for any purpose, provided the original work is properly cited, a link to the licence is given, and indication of whether changes were made. See: https://creativecommons.org/licenses/by/4.0/.
Statistics from Altmetric.com
Key questions
What is already known about this subject?
Predictive power of B-type natriuretic peptide (BNP) levels at hospital admission (BNPad) is inferior to that of BNP levels at discharge (BNPdis) in patients with acute heart failure (HF). However, the mechanism underlying these differences has not been fully elucidated.
What does this study add?
Through multivariate analysis after accounting for known confounding factors related to circulating BNP levels, we created a formula for predicting BNP levels at discharge (predicted-BNPdis) from BNPad and other parameters measured at admission.
This study showed that statistically accounting for confounding factors affecting BNP levels improves the predictive power of BNP levels measured at the time of hospital admission.
How might this impact on clinical practice?
This predicted-BNPdis has superior predictive power for clinical outcomes to BNPad. This may contribute to the risk stratification of acute HF and primary intensive care management in acute vulnerable phases of HF.
Introduction
B-type natriuretic peptide (BNP) is widely used as a predictive biomarker in patients with heart failure (HF).1 However, earlier studies showed that in patients with acute HF, the predictiveness of BNP levels measured at hospital admission (BNPad) for clinical outcomes is inferior to BNP levels measured at discharge (BNPdis).2 3 Although the reason for the insufficient predictive power of BNPad compared with BNPdis in these patients has not been fully elucidated, several confounding factors are well known to influence circulating BNP levels (eg, left ventricular end-diastolic pressure (LVEDP) and renal function).4–7 However, how these parameters influence the lower predictability of BNPad than that of BNPdis remains uncertain.
Given the importance of clinical risk stratification for hospitalised patients with heterogeneous clinical syndromes, this study aimed to identify the confounding factors affecting BNPad that are associated with BNPdis. We also tested the hypothesis: whether statistical adjustments of these confounding factors are related to predictive power of BNPad improvements in patients with acute HF.
Methods
Study design
This was a cross-sectional study of patients with HF admitted to the National Cerebral and Cardiovascular Center of Japan.
Study population
Retrospective study
Included in the retrospective study were 688 patients hospitalised for HF between January 2013 and March 2016 (BNP on admission: ≥100 pg/mL). We excluded patients who did not undergo a blood test and echocardiography, who underwent implantation of a left ventricular (LV) assist device (n=3), or who died in the hospital (n=24) during the corresponding hospitalisation. We also excluded patients who underwent mitral valve surgery (n=85) due to its influence on transmitral flow and septal mitral annular velocity.
Diagnosis of HF was based on the Framingham criteria.8 Whether or not a HF episode met the Framingham criteria was determined by each attending physician and an investigator (H Takahama) via medical record review. We excluded patients who did not meet the criteria, as judged by the investigator and the attending physician for each patient. According to the guidelines of the Japanese Circulation Society,9 we defined the cut-off value of plasma BNP level for diagnosis of HF as 100 pg/mL.
Prospective study
We prospectively collected data from 104 patients between January and June in 2019 based on the same criteria used for the retrospective study.
Echocardiography
Through medical chart review, we retrospectively reviewed the echocardiography data collected during the hospitalisation. LV dimensions were measured according to the American Society of Echocardiography guidelines.10 LV ejection fraction (EF) was measured using the modified Simpson method or the semiquantitative two-dimensional visual estimate method, as described previously.11 Transmitral inflow was measured with pulsed-wave Doppler using standard methods as described previously.12 The septal mitral annular early diastolic velocity (e′) was determined with spectral tissue Doppler imaging. LVEDP was calculated as 11.96+0.596 × early diastolic transmitral flow velocity (E)/e′, as previously reported.13
Measurement of plasma BNP concentration
All biochemical analyses were performed as routine clinical examinations. BNP were measured by human brain natriuretic peptide kit (TOSOH corporation, Tokyo, Japan).
Clinical outcomes
After the admission date, we investigated through medical chart review or a letter all causes of death and rehospitalisation for HF. Combined clinical events were defined as all-cause death or rehospitalisation for HF.
Ethics
The study was designed to be carried out without obtaining individual informed consent according to the ‘opt-out’ principle. Instead, we publicised a summary of the study protocol with the contact information for our office on the institution website, which provided patients with the ability to refuse enrolment to the study. This study protocol was also registered in the Japanese University Hospital Medical Information Network Clinical Trials Registration.
Statistical analyses
Results are expressed as the median and IQR. Fisher’s exact test or the χ2 test was used to compare categorical variables, as appropriate. With regard to baseline patient characteristics, Wilcoxon’s rank-sum test was used for comparison of continuous variables between two groups. HRs with 95% CIs and probability (p) values determined using the likelihood ratio test are presented. The area under the receiver operating characteristics (ROC) curve (AUC) and C-statistics were also calculated. AUCs were compared using an algorithm developed by DeLong et al.14 Pairwise comparisons of the areas under multiple ROC curves were made using the roccomp command in Stata. Multivariate analysis/regression was used to test multiple covariates. All tests were two tailed, and values of p<0.05 were considered significant. All statistical analyses were performed using JMP V.9 statistical analysis software (SAS Institute Japan, Inc, Tokyo, Japan) and Stata V.15 (Stata Corporation LLC, College Station, Texas, USA).
Results
Retrospective data analysis
Using the inclusion and exclusion criteria described in the Methods section, we identified 688 patients with HF from our database. The patient characteristics on admission were as follows (table 1): New York Heart Association class III and IV on admission, 43% and 45%, respectively; median LVEF: 35% (IQR: 24%–55%); median LV end-diastolic diameter (LVEDD), 56 mm (IQR: 48–64 mm); and median plasma BNP levels, 671 pg/mL (IQR: 370–1170 pg/mL). Median hospitalisation length was 19.5 days (IQR: 14–27 days). The patients treated without beta-blockers were often observed in those with valvular regurgitation and with HF with preserved EF. Based on earlier studies, we selected the following clinical parameters known to influence circulating BNP levels for analysis: age, sex,4 LVEDP,5 15 blood pressure,16 heart rate,7 body mass index (BMI),6 LVEF,17 18 end-diastolic volume,17 LVEDD,18 cholesterol levels,19 anaemia,20 renal function,7 20 atrial fibrillation21 and diabetes mellitus.22 The results of univariate analyses of the association between BNPdis and the selected parameters are shown in table 2. Age, BMI, systolic blood pressure, diastolic blood pressure, LVEDD, LVEF, estimated LVEDP (eLVEDP), estimated glomerular filtration, blood urea nitrogen (BUN), haemoglobin, hematocrit, total cholesterol and low-density lipoprotein cholesterol on admission were all associated with BNPdis after adjusting for BNPad. Stepwise analysis identified the following parameters as significantly associated with BNPdis after accounting for BNPad levels: age, systolic blood pressure, LVEF, eLVEDP and BUN levels (table 3). Subsequent multivariate analysis revealed the parameter estimates of the above factors to be: 3.81 (age), −1.09 (systolic blood pressure), −0.87 (LVEF), 6.72 (eLVEDP), 3.48 (BUN) and 0.21 (BNPad). Using those data, we developed the following formula to predict BNPdis from BNPad: the ‘predicted-BNPdis’=3.81 × age – 1.09 × systolic blood pressure – 0.87×LVEF + 6.72 × eLVEDP + 3.48 × BUN + 0.21 × BNPad – 184.5. Next, the analysis of association non-pharmacological intervention on the relation between the parameters used for estimation of the predicted-BNPdis and BNPdis were performed because the therapeutic intervention might influence the discharge levels of BNP. As shown in online supplemental table 1, no statistical significance was found. In addition, there was significant differences in both BNPad and BNPdis in patients with initial admission and rehospitalisation for HF. As shown in online supplemental table 2, both BNP levels were higher in patients with readmission than those in initial admission. The correlation of the predicted-BNPdis with BNPdis was similar between the patients with initial admission and readmission (p<0.05).
Supplemental material
Supplemental material
Baseline patient characteristics
Association of discharge levels of BNP with clinical parameters on admission (univariate analysis)
Stepwise regression analysis for association of BNPdis with variables on admission
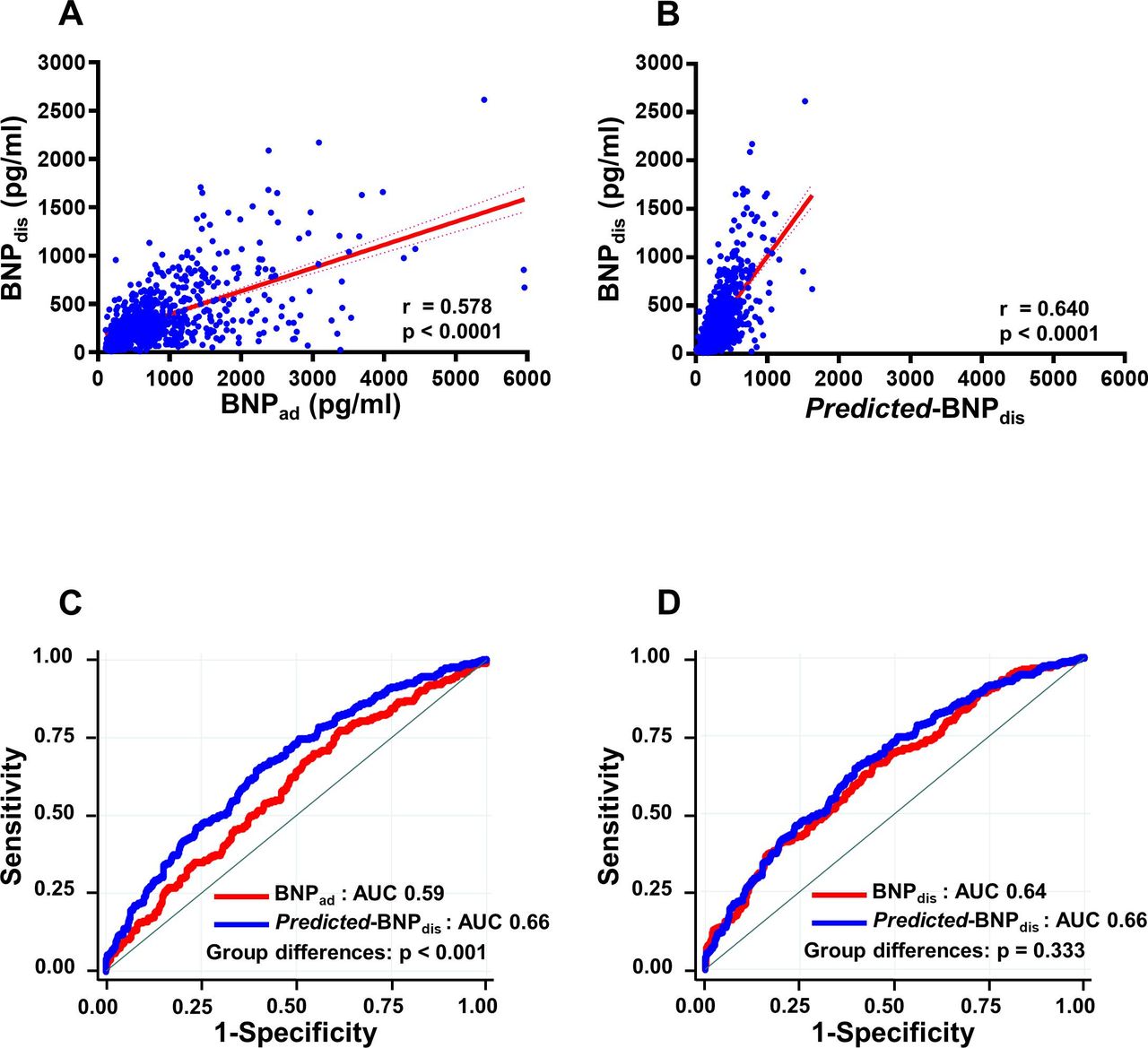
During the follow-up period (median: 623 days, IQR: 188–730 days), combined clinical events occurred in 295 (43%) patients: all causes of death (n=68, 10%) and rehospitalisation for HF (n=227, 33%). Figure 1 shows the correlation between BNPdis and BNPad (figure 1A) and between BNPdis and predicted-BNPdis (figure 1B). However, AUC analysis showed that predicted-BNPdis was significantly more predictive of outcome than BNPad (p<0.001) and was comparable with the predictiveness of BNPdis (figure 1C,D).

Association between BNP levels at hospital discharge and levels on admission or predicted BNP levels at discharge (predicted-BNPdis) and their prognostic power. (A) Correlation between circulating BNP levels at hospital discharge (BNPdis) and BNP on admission (BNPad). (B) Correlation between BNPdis and predicted BNP levels at discharge (predicted-BNPdis).(C) Area under the receiver operating characteristics curve (AUC) analysis of the occurrence of the combined clinical events. AUC for the predicted BNP levels at discharge (predicted-BNPdis: blue) was superior to BNP levels on admission (BNPad: red) (p<0.001). (D) There was no significant difference in the AUC for the predicted-BNPdis (blue) and BNP levels at discharge (BNPdis: red). BNPad, B-type natriuretic peptide on hospital admission; BNPdis, B-type natriuretic peptide at discharge.
Prospective data analysis
The prospective study revealed similar relationships between BNPad or predicted-BNPdis and BNPdis (figure 2A,B).

{kind=link}
{kind=link}
Association between BNP levels at hospital discharge and levels on admission or predicted BNP levels at discharge (predicted-BNPdis) in a prospective study. (A) Correlation between circulating BNP levels at hospital discharge (BNPdis) and BNP levels on admission (BNPad). (B) Correlation between BNPdis and predicted BNP levels at discharge (predicted-BNPdis). Note the similarity between the results of the prospective and retrospective studies. BNPad, B-type natriuretic peptide on hospital admission; BNPdis, B-type natriuretic peptide at discharge.
Discussion
Circulating BNP levels are affected by a number of confounding factors during the acute phase of HF and are associated with fluctuations in measured BNP levels during the initial few days after hospital admission or intensive treatments.23 24 These fluctuations are mainly due to changes in ventricular preload and the systemic fluid overload state. Our retrospective study confirmed known confounding factors affecting BNP levels and showed that these factors statistically were associated with lowering the predictive power of BNPad levels for patient outcomes. This study also showed that after statistically accounting for these confounding factors, the predictive power of the resultant BNP value (predicted-BNPdis) did not significantly differ from that of BNPdis. Moreover, the finding of the correlation of predicted-BNPdis with BNPdis was validated by obtaining similar results in a prospective study.
Several earlier studies reported on the factors influencing circulating BNP levels. For example, Iwanaga et al5 measured LVEDP using a LV catheter system and clearly demonstrated that LV wall stress strongly correlated with plasma BNP levels. In addition, factors such as increased cardiac preload likely due to excess body fluid, which may stretch ventricular cardiomyocytes, sharply increases circulating BNP levels in patients with HF. By the time BNPdis levels are measured, however, the patient has reached an appropriate volume state through removal of the excess body fluid. Consequently, BNPdis levels may more closely reflect myocardial quality per se or a ‘true ventricular trait’. This may explain why BNPad levels measured during the acute phase of HF have less predictive power than BNPdis levels. In the present study, we observed that after accounting for several factors, including LVEDP and LVEF, as well as blood pressure and renal function, the predicted BNP levels, which we termed predicted-BNPdis, strongly correlated with BNPdis levels and were equally predictive of patient outcome.
Thus, by determining the impact of factors responsible for the difference in predictive power between BNPad and BNPdis, we were able to shed light on the relationship between these factors and BNPdis. These findings may further our understanding of BNP levels, which are influenced by various factors in patients with acute HF.
Limitation
The present study has several limitations. First, this was a single-centre investigation with a limited number of patients. Nevertheless, we were able to confirm a formula that predicts BNP levels at discharge from clinical parameters at the time of admission. Second, several patients did not undergo a blood test for BNP and E/e′; we excluded these patients from our analysis. Next, it is widely known that the therapeutic intervention might influence the discharge levels of BNP. These therapeutic interventions might also influence the relationship between the clinical parameters on admission with the BNPdis, although no statistical association were found in online supplemental table 1. Furthermore, this study enrolled the patients between 2013 and 2016, and at that time, sacubtrilvarsartan was not approved in Japan, which is known to influence circulating BNP levels. Further investigation will be necessary to confirm the effects of sacubtrilvarsartan on the predicted BNP levels at discharge. The association of the predicted-BNPdis with BNPdis is statistically significant, but the degree of correlation was modest; we could not exclude the possibility that the other unknown factor or therapeutic effects, which are not included for the estimation of BNPdis in this study, might be also associated with the regulation of BNP. Taken together, this study was not designed to investigate the effects of the prospectively controlled pharmacological or non-pharamacological intervention on BNPdis. Further prospective study will be necessary to address these problems.
In addition, there was no discharge criteria for the research in this study, and in general, discharges were determined by the attending physician. Although the discharge levels are determined by clinical findings including BNP levels in stable phases of HF, the variation of HF severity at discharge exists among the attending physicians, which might create the further variation of the discharge levels of BNP.
Conclusion
We have shown the confounding factors affecting measured BNP levels and demonstrated BNP prediction at discharge in hospitalised patients with HF. This predicted BNP values have superior predictive power for clinical outcomes to raw BNP values on admission. This may contribute to the risk stratification of acute HF and primary intensive care management in acute vulnerable phases of HF.
Data availability statement
No data are available.
Ethics statements
Ethics approval
The study protocol was approved by the institutional review bord of the National Cerebral and Cardiovascular Centre (M26-127 and M30-155).
Acknowledgments
The authors would like to thank the research coordinator and assistants in our institute for the data collection.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors HT, EA, TN, KK, SY and CI contribute to design of the work; HT, EA, DO, KN contribute to the acquisition and analysis of data for the work; HT, EA, HK, SY, YI, AO, MA, MA, KM and CI contributed to drafting the work or revising it critically for important intellectual content; final approval was done by HT.
Funding This work was supported by the Intramural Research Fund of the National Cerebral and Cardiovascular Centre of Japan (grants 30-1-3 to CI).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.