Article Text

Abstract
Cardiac disease is now the leading cause of death in Duchenne muscular dystrophy (DMD). Clinical evaluations over time have demonstrated asymptomatic cardiac troponin elevations and acute elevations are associated with symptoms and cardiac dysfunction in DMD. Clinicians require a better understanding of the relationship of symptoms, troponin levels and progression of cardiac disease in DMD. As clinical trials begin to assess novel cardiac therapeutics in DMD, troponin levels in DMD are important for safety monitoring and outcome measures. The Parent Project Muscular Dystrophy convened an expert panel of cardiologists, scientists, and regulatory and industry specialists on 16 December 2019 in Silver Spring, Maryland and reviewed published and unpublished data from their institutions. The panel recommended retrospective troponin data analyses, prospective longitudinal troponin collection using high-sensitivity cardiac troponin I assays, inclusion of troponin in future clinical trial outcomes and future development of clinical guidelines for monitoring and treating troponin elevations in DMD.
- biomarkers
- genetic diseases
- inborn
- cardiomyopathy
- dilated
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Cardiac troponin I (cTnI) and T (cTnT) are components of the contractile apparatus of myocardial cells expressed almost exclusively in the heart and are the preferred biomarkers for the evaluation of myocardial injury.1 Other biomarkers including creatine kinase MB (CK-MB) isoform are less sensitive and less specific, especially with associated skeletal muscle disease.2 Various causes lead to cardiac troponin release, including myocardial ischaemia often related to atherosclerotic coronary obstruction. Other non-ischaemic cardiac causes include heart failure, myocarditis and cardiomyopathies. Some systemic illnesses are also associated with troponin release, including pulmonary embolism, chronic kidney disease, sepsis and cardiotoxic agents. Troponin release can be acute or chronic and related to multisystem involvement.2 3
Cardiomyopathy has become the leading cause of death in Duchenne muscular dystrophy (DMD).4 In DMD, case studies of acute-onset myocardial injury measured by troponin release are well documented dating back to the 1960s, including a boy 10 years of age.5 6 More recently, Hor et al7 described additional cases of acutely elevated troponin levels in subjects with DMD. Elevated troponin levels have been described in asymptomatic patients with DMD long before the development of the typical well-defined cardiac disease known to associate with DMD.8
Despite these historical reports, troponin elevations in patients with DMD are poorly understood and have unclear significance. With the support of the Parent Project Muscular Dystrophy (PPMD), a panel of experts in neuromuscular disease, adult and paediatric cardiology, Food and Drug Administration and industry convened to discuss the role of troponin in DMD clinical care and its use both as a safety and efficacy biomarker in DMD clinical trials.
Troponin and neuromuscular diseases
As noted, cardiac troponin elevations have been described in DMD since the 1960s. However, cTnT is considered less specific for myocardial injury as it is elevated in multiple neuromuscular disease conditions, likely reflecting a skeletal muscle source.9 10 Chronic skeletal muscle disease can represent a potential cause of cTnT elevation, particularly when high-sensitivity (hs-cTnT) assay is used.11 12 cTnT was demonstrated to correlate better with creatine kinase and myoglobin levels than with cTnI, and assays showed cross-reactivity of cTnT antibodies with skeletal muscle TnT. These factors limit the use of cTnT and CK-MB for assessment of myocardial injury in DMD as cTnI is more specific.13 cTnI is not expressed in human skeletal muscle during development or during regenerative muscle disease processes such as seen in DMD.14
The clinical significance of elevated cTnI in DMD and neuromuscular diseases continues to evolve. A recent study of 117 patients with DMD, Becker muscular dystrophy (BMD), DMD/BMD carrier, limb-girdle muscular dystrophy (LGMD), facioscapulohumeral dystrophy (FSHD) and myotonic dystrophy (DM) type I found a threefold increased risk of cardiac disease in subjects with an hs-cTnI level greater than 7.6 ng/L (Access High Sensitivity Troponin I Assay, Beckman-Coulter; normal <2.3 ng/L).15 In a study of 53 subjects with dystrophic myopathies (including DMD, DMD carrier, BMD, LGMD 2A, FSHD), DM types I and II, and Becker/Thomsen myotonias, only three subjects, two with DMD and one with DM, had elevated cTnI levels and all three had evidence of cardiac disease.13 Other studies have also demonstrated increases in cTnI levels in DMD and BMD.16–18 However, other studies found normal cTnI levels in DMD.19–21 Elevated cTnT and cTnI levels were also detected in DMD/BMD carriers who are at risk of developing cardiomyopathy later in life.22–24 hs-cTnI levels in DM type I were highly elevated in ambulatory subjects and predictive of cardiac dysfunction (Architect Stat Troponin Assay, Abbott).25 Elevated cTnI levels were observed in patients with Friedreich’s ataxia.26 Elevated troponin levels also occur in patients with spinal muscular atrophy (SMA), and transient increases in cTnI levels (up to 0.176 µg/L; assay and normal limit not reported) of unclear significance were observed following Zolgensma infusion in clinical trials. This is an example of uncertainty regarding whether troponin levels are related to SMA or whether these reflect the clinical intervention.27
Preclinical data on troponin in dystrophin-deficient animal models
Troponin serum levels were assessed in animal models of dystrophin deficiency, including the dystrophin-deficient mdx mouse and related genetic models. cTnI was shown to be cardiac-specific and not present in the regenerating skeletal muscle of mdx mice.28 Martindale and Metzger29 measured decreased cTnI after membrane-stabilising poloxamer 188 therapy in mdx mice. Buyse et al30 found elevated cTnI levels in mdx mice that were decreased after idebenone therapy. In the dystrophin-utrophin double knockout mouse, Lopez et al31 showed decreased serum cTnT after whole body periodic acceleration.
The dystrophin-deficient golden retriever muscular dystrophy (GRMD) large animal model recapitulates some aspects of the human cardiomyopathy course better than the mdx model. Townsend et al32 administered a chronic infusion of a membrane-sealing agent to severely affected GRMD dogs and found decreased troponin I levels and reduced myocardial fibrosis. A case report by Schneider et al33 described a GRMD dog exhibiting acute cardiac disease including tachyarrhythmia associated with significant increase in troponin I, NT-pro-brain natriuretic peptide and progression over a 3-year period to severe dilated cardiomyopathy. In ongoing experiments, monthly troponin I values obtained from dystrophin-deficient dogs revealed periodic spikes in troponin levels and an increase in the number of spikes with age correlated with cardiac involvement. Lower troponin levels were obtained in older dogs with loss of cardiac mass (Sweeney, unpublished data, 2020). The preclinical data support a role for monitoring troponin levels during therapeutic trials, but further recommendations for preclinical studies were not the focus of the expert panel.
Clinical data on troponin in DMD
Troponin levels are used less clinically in paediatrics due to low prevalence of ischaemic cardiac disease. In order to understand the relevance of troponin levels in DMD, it is important to determine troponin levels in healthy children. In 2009, the CALIPER (Canadian Laboratory Initiative on Pediatric Reference Intervals) study of healthy children and adolescents published reference laboratory values for paediatric subjects including cTnI using the Abbott Architect ci8200.34 cTnI levels had maximal measures of 0.176 μg/L in subjects less than 1 year old, 0.112 μg/L in subjects 1–5 years old, 0.018 μg/L in subjects 6–10 years old, 0.663 μg/L in subjects 11–14 years old, and 0.401 μg/L in subjects 15–20 years old. Due to these low levels in normal paediatric patients, Caselli et al35 used hs-cTnI testing (Architect Stat High-Sensitivity TnI, Architect i1000SR platform, Abbott Diagnostics) and found approximately 13% of all subjects aged <1 month to <18 years had non-detectable levels. hs-cTnI levels were highest in the first month of life (mean 37.5 ng/L) and decreased with age (infants: mean 19.4 ng/L; children 1–10 years: mean 6.5 ng/L; adolescents: mean 3.1 ng/L). Males showed significantly higher hs-cTnI levels than females. An earlier study using a similar hs-cTnI assay (precommercial Architect Stat hs-cTnI Assay, Abbott Diagnostics) demonstrated physiological variability in healthy subjects aged 8–12 years old with multiple measures in the range of 0%–136%, with a median of 33%.36 These studies support the presence of cTnI release in the healthy paediatric population likely related to physiological myocardial growth and demonstrate the need for assay-specific norms related to gender and age. Thus, standardisation of troponin assays and development of normal values are important foundations for the evaluation of myocardial injury in DMD.
In a recent publication, Voleti et al8 described cTnI levels and the relationship to cardiac magnetic resonance (CMR) imaging results in DMD. Data from this observation cohort of asymptomatic participants with DMD were obtained at the time of CMR, and the cTnI levels from participants with a single measure are shown in table 1, ranging from 0.02 ng/mL to 0.88 ng/mL (ELISA assay; Siemens Dimension Analyzer; normal range <0.04 ng/mL).
Cross-sectional cTnI levels, per cent ejection fraction and cystatin C levels of asymptomatic subjects with DMD demonstrating elevations from normal level of 0.02 ng/mL (ELISA assay; Siemens Dimension Analyzer, Siemens Laboratory Diagnostics, Tarrytown, New York) and no relation to age, systolic function or kidney function
This study also showed that subjects with DMD with mild late gadolinium enhancement (LGE) on CMR had significantly increased troponin levels (0.28±0.38 ng/mL) compared with those with no LGE (0.05±0.08 ng/mL).8 Interestingly, the troponin levels decreased in subjects with DMD with moderate to severe LGE (0.11±0.14 ng/mL). This may be related to a loss of susceptible myocardium to damage over time. Additional cohort data are provided in table 2, showing participants with DMD with longitudinal cTnI levels studied at Children’s National Hospital (NCT02921321). These data demonstrate the heterogeneity of troponin levels in DMD, noting that levels may increase, decrease or remain unchanged over time. Based on these findings, it is necessary to more systematically collect data across all ages and DMD clinical courses.
Longitudinal cTnI levels and per cent ejection fraction in asymptomatic subjects with DMD over a 3-year follow-up period demonstrating variable changes in troponin levels and systolic function over time
While these data begin to elucidate the chronic cTnI levels in asymptomatic patients with DMD, recent reports focused on acute elevations of cTnI in DMD associated with symptoms including chest pain. An important case series described eight subjects with DMD, aged 9–23 years, who presented with episodes of acute chest pain and transient elevations of cTnI.7 The subjects had normal baseline ECGs that evolved to show ST segment elevations in leads II, III and aVF in seven subjects, with additional elevations in V4–V6 in two subjects and V1–V4 in one subject. However, these elevations were not consistent with any specific coronary distributions. Troponin levels ranged from 31 ng/mL to 62 ng/mL (assay not reported; normal <0.03 ng/mL) and normalised over 4 days. All subjects demonstrated a decrease in systolic function during the acute episode. Two subjects had a cardiac CT scan and two subjects underwent cardiac catheterisation with no coronary abnormalities identified. Importantly, the pattern of delayed enhancement on CMR in all subjects was not consistent with ischaemia. All subjects received supportive care with traditional cardiac medications and follow-up continues.
Another case report described an 18-year-old subject with DMD who presented with chest pain, abnormal ECG with significant ST segment elevations in leads I, II, III, aVF and V6, and acutely elevated cTnI level of 39 ng/dL that later peaked at 73 ng/dL (assay not reported; normal range <0.4 ng/dL).37 The subject had global hypokinesis and normal coronary angiography, and LGE was evident on CMR. The onset of symptoms temporally correlated with a shift in glucocorticoid dosing and, potentially, an acute inflammatory reaction. His symptoms resolved with restarting steroids and supportive care. A second case report of an 11-year-old boy with DMD presenting with chest pain, decreased cardiac function, elevated cTnT and normal coronary angiography also improved after increasing his steroid dose.38 Two more 13-year-old boys with DMD were described with ST segment elevations and troponin changes.39 40 A similar clinical picture was also noted after an episode of respiratory failure in a patient with DMD.41 These reports demonstrate a unique presentation of acutely elevated troponin levels with abnormal ECGs in DMD and no evidence of coronary artery disease. The limited utility of invasive diagnostic cardiac catheterisation should only be considered in specific cases where a known cause of ischaemia is under consideration.
Clinical monitoring of troponin in DMD
Current recommendations for cardiac care of patients with DMD include a cardiac evaluation at the time of diagnosis, including physical examination, ECG and echocardiogram.42–46 Similar evaluations should occur every 1–2 years in asymptomatic children until age 10, when yearly evaluations are recommended. Symptomatic children should be evaluated more frequently as determined by the provider. Periodic use of advanced imaging including CMR and ambulatory monitoring is also recommended.
There are no current recommendations for the routine monitoring of cTnI levels in DMD. Therefore, the distribution of troponin elevations in the DMD population is difficult to determine, in part because there is clinical ascertainment bias towards testing only those who are symptomatic. However, there are also those with asymptomatic chronic lower level elevations and older individuals with abnormal left ventricular function and acute changes in the setting of other illness (eg, sepsis, pneumonia, fracture). Patients with chronic kidney disease can demonstrate increased levels of hs-cTnI and hs-cTnT at baseline and kidney disease can develop in DMD.47 Creatinine as a marker of renal function has limited value in DMD because of reduced muscle mass. However, cystatin C, a non-glycosylated protein unaffected by muscle mass, is an additional biomarker of nephrotoxicity in the DMD population and elevated levels were demonstrated in a subject with DMD in renal failure.48 Cystatin C levels are included in table 1, demonstrating normal kidney function associated with variable cTnI elevations. The diagnostic value of cTnI may be more difficult to discern in patients with DMD with kidney failure, and treating physicians would need to consider changes from baseline and use higher cut-off values.47 This demonstrates another scenario where it is important to collect longitudinal baseline data and consider cystatin C levels to correlate troponin with kidney function.
hs-cTnI levels are commonly used in clinical evaluations of acute coronary syndrome and chest pain in adult patients. The Atherosclerosis Risk In Communities Study concluded that elevated hs-cTnI is strongly associated with increased global cardiovascular disease incidence in the general population, independent of traditional risk factors.49 Since many patients with DMD will present to adult and community hospitals, hs-cTnI levels have replaced traditional troponin assays and are recommended in the Fourth Universal Definition of Myocardial Infarction (2018).1 This will provide new data to physicians to help with clinical decisions and potential risk stratification even in asymptomatic subjects with DMD. So while it is not yet known how the improved analytical sensitivity will impact clinical care in DMD, it will be paramount to include hs-cTnI analyses in future evaluations.50
Increases in cTnI levels could signal changes in therapeutic approaches. While standard of care now includes consideration of ACE inhibitors around age 10, initiation of this medication could begin sooner if elevated troponin levels are identified.43 In addition, mineralocorticoid receptor antagonists showed benefits in slowing the loss of myocardial strain in subjects with DMD and could be useful.51–53 Some of these benefits are related to membrane stabilisation properties that could also slow troponin release from myocardial cells.54–56 Increased steroid dosing showed benefits in two case reports.37 38 A new steroid derivative therapeutic also demonstrated membrane stabilisation properties and could provide an alternative to steroid therapy in subjects with elevated cTnI levels.57 58 One agent or a strategic combination of these therapeutics could provide new benefits to children with DMD with elevated troponin levels.
In order to best direct clinical care, it will be important to understand how these transient spikes or chronic elevations may change with age, cardiac mass, respiratory disease and/or skeletal muscle function. Further research is needed to determine the potential mechanism(s) including coronary spasm, inflammation, arrhythmia, volume overload, elevated heart rate and/or elevated blood pressure behind troponin elevations, and the potential impact of the interplay with skeletal and respiratory muscle function is critical to elucidate. Once better understood, incorporating the related basic science will be essential in determining appropriate therapies.
Troponin monitoring as a DMD clinical trial biomarker
The role of cardiac troponin as an appropriate clinical trial biomarker in DMD is unclear at this time. Monitoring of cardiac troponin levels as a safety marker may be important. The use of troponin as a safety outcome marker would require determining normal values and thresholds for normal and acceptable fluctuations for both cardiac and non-cardiac (skeletal muscle) directed therapies. In a trial involving a single baseline intracoronary injection of allogeneic cardiosphere-derived cells, the authors noted periprocedural elevations in cTnI, but also noted two subjects in both the usual care and treatment groups that demonstrated elevated cTnI levels during the 12-month follow-up period, described as ‘greater than ×5 composite 99th percentile or at least 20% elevated beyond baseline’. Once recovered from the intervention, these asymptomatic elevations were not regarded as adverse events.59
In a clinical trial of a monoclonal antimyostatin antibody domagrozumab (NCT02310763), cTnI was measured as a clinical laboratory biomarker in 120 participants with DMD. Approximately 20% of participants had cTnI values above 0.3 ng/mL at baseline (assay not reported; normal ≤0.03 ng/mL); elevations were seen at all timepoints measured in the trial and elevations were not sustained or associated with clinical symptoms. The highest value seen was approximately 3.5 ng/mL. Increased cTnI levels regarded as adverse events were seen in two subjects who received placebo and one subject who received treatment.60 61 Additional analysis is ongoing and the role of troponin as a biomarker for safety, treatment outcome, susceptibility to risk or response predictiveness needs further study.
Future directions
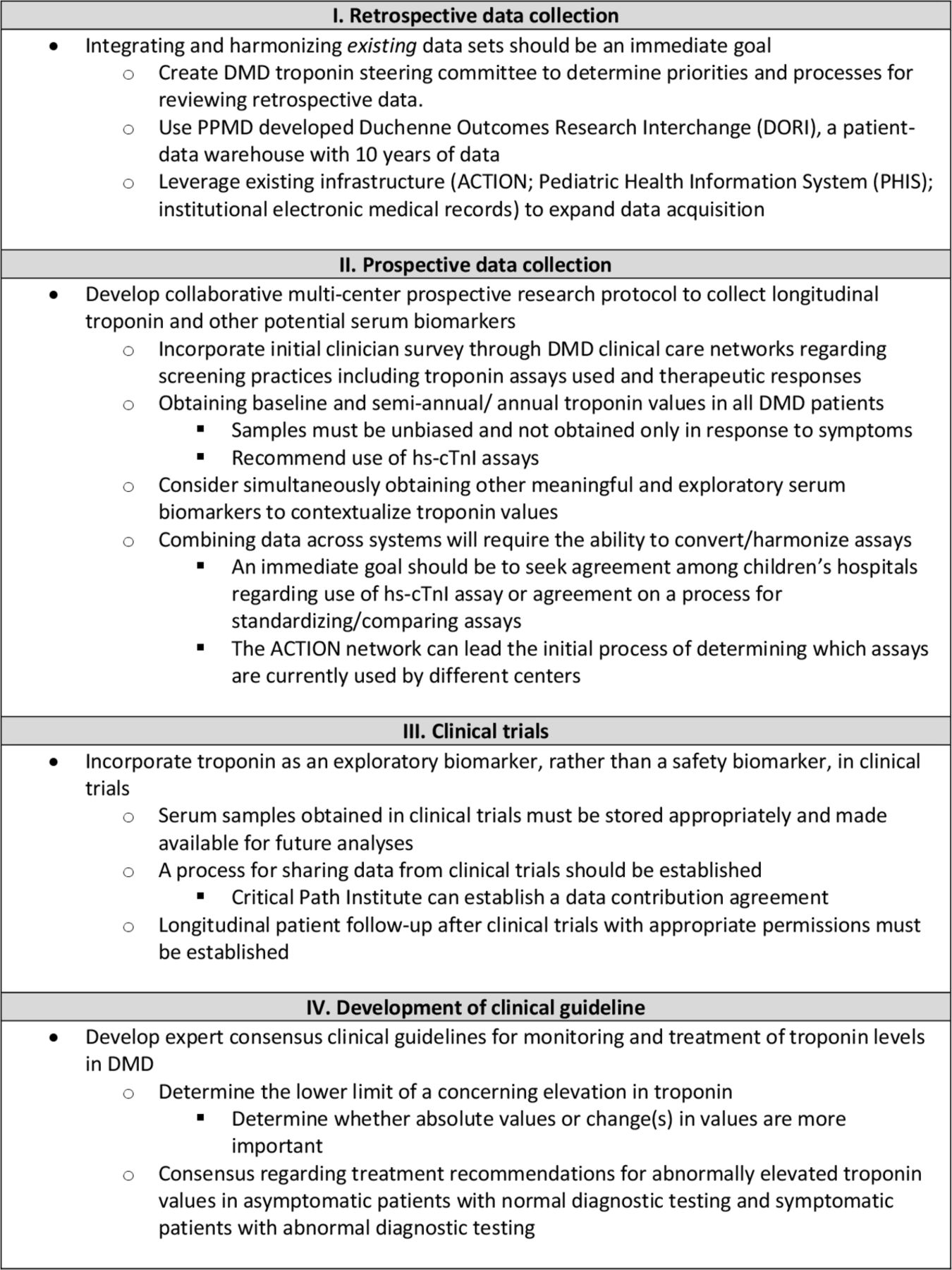
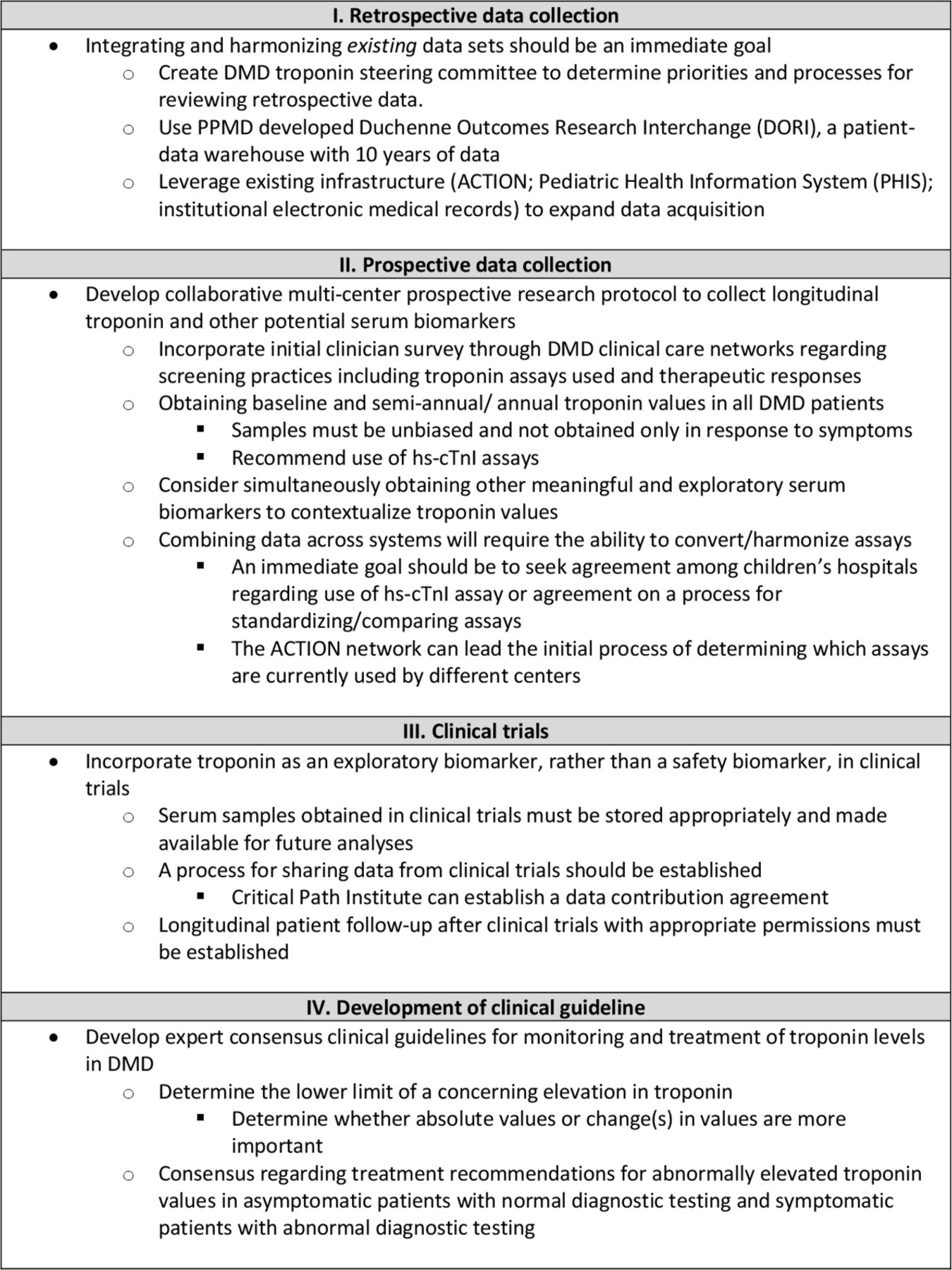
The expert panel noted several areas to focus efforts to further develop an understanding of cTnI in DMD (figure 1) - Figure 1 seems blurry, any way to improve?. The first area identified was to leverage existing data sets to perform new data analyses. Current data from different studies including clinical trials, longitudinal observational studies and registries can be used to create a consistent data structure for analysis with the goal of developing an actionable drug development tool and a clinically meaningful screening tool. This approach would need to use existing infrastructure to involve these different entities. The Advanced Cardiac Therapies Improving Outcomes Network may illustrate such a path forward for DMD. The network’s goal is to improve critical outcomes for children and adult congenital heart disease patients with heart failure by developing an international collaborative learning health system that unites all key stakeholders (patients, families, clinicians, researchers and industry). While initially addressing heart failure, the approach of transforming an unstandardised clinical paradigm can provide the infrastructure to rapidly disseminate critical information to families and clinicians. This is quite similar to the current state of cTnI monitoring in DMD. The network has the expertise to determine the availability of cTnI data or samples from previous clinical trials, contact individual trial sites to obtain necessary consent, leverage social media networks within the DMD community and involve principal investigators.
{kind=link}
Recommendations from the expert panel for the further study of the natural history of cardiac troponin I testing in DMD. ACTION, Advanced Cardiac Therapies Improving Outcomes Network; DMD, Duchenne muscular dystrophy; hs-CTnI, high-sensitivity cardiac troponin I; PPMD, Parent Project Muscular Dystrophy.
The panel recognises the importance of prospective data collection. This approach may begin with a survey of centres involved with DMD cardiac care regarding the use of cTnI monitoring in both asymptomatic and symptomatic subjects with DMD. The panel recommended a multicentre collaborative research protocol-based assessment for monitoring cTnI levels on a consistent time frame, such as at the time of cardiac imaging, but not more frequently than every 6 months, and focusing on hs-cTnI testing as feasible. The expert panel felt this information would be clinically useful as it could help provide context for interpretation of troponin levels monitored during an acute event, should it occur. Further discussion should focus on other serum or imaging biomarkers that may prove important tools to monitor cardiac function in DMD. Serum ST2 levels were increased in subjects with DMD with cardiomyopathy and matrix metallopeptidase (MMP) 9 was elevated in subjects with DMD compared with normal controls.62 Serum MMP7 was increased in subjects with DMD with evidence of fibrosis compared with normal subjects with DMD and controls.63 Novel imaging biomarkers using CMR T1 and T2 imaging should provide further meaningful context for cTnI levels.64
The optimal approach should also incorporate cTnI levels in developing clinical trials. In fact, consideration should be given to including cTnI as an exploratory outcome rather than a safety biomarker. Information obtained in clinical trials may ultimately have great value, but questions remain regarding how to interpret values obtained in clinical trials for safety monitoring. For example, until the natural history of the disease is well understood, it would be difficult to determine whether an elevated level obtained in a clinical trial represents an adverse event or just natural variation. Based on an accumulation of data, future clinical trials will be better informed on how to determine a critical level at which an elevated troponin level becomes a safety concern. A process for sharing real-time cTnI results from clinical trials should be established incorporating existing infrastructure such as the Critical Path Institute.
The above approaches will ultimately inform clinical guidelines. Based on the current knowledge base, the expert panel recommends clinical monitoring and supportive care of patients with DMD with elevated troponin levels. Consideration should be given to optimising medical management with ACE inhibitors, beta-blockers and/or mineralocorticoid receptor antagonists based on cardiac function, degree of myocardial fibrosis and cardiomyopathy trajectory. These patients are at low risk of atherosclerotic disease or coronary thrombosis and urgent coronary angiography is not recommended. By establishing standardised timing and methods for routine cTnI monitoring, clinicians will gain further insight into the progression of myocardial disease in DMD. Guidelines would include a cTnI threshold and the appropriate response to above threshold levels, minimising the use of coronary angiography in these patients. These guidelines would inform the entire medical community outside of academic centres and improve quality of care in community hospitals where children with DMD may present with chest pain episodes. These guidelines would also inform the DMD parent community and reassure parents by clarifying the appropriate evaluation and treatment during these stressful events. This mutual understanding of presentation and treatment will improve care and family support and optimise outcomes for this vulnerable population.
Based on this meeting summary and the reference literature, there remain limitations. Cardiac disease is an important feature in DMD; however, it is not clear if cardiac troponins are a reliable biomarker for monitoring cardiac health in patients with associated chronic skeletal muscle disease. Potential cross-reactivity in assays for cTnI and cTnT must be improved to differentiate from skeletal muscle damage. There is not a universal standard for cTnI monitoring and paediatric hospitals use both traditional and high-sensitivity troponin assays less frequently, limiting data comparison across centres. Lastly, a more comprehensive understanding and characterisation of myocardial injury that is occurring in DMD is necessary to comprehend its relation to cTnI release.
In conclusion, further understanding of cTnI levels in DMD is necessary to best monitor and treat the cardiomyopathy associated with DMD. Limited data and case reports have demonstrated both chronic asymptomatic mild cTnI elevations and acute symptomatic often striking cTnI elevations in DMD. The cTnI levels usually normalise, but the lasting effects of the associated myocardial injury are not well understood. As cardiac disease is now the leading cause of death in DMD, this expert panel strongly encourages retrospective troponin data analyses, prospective longitudinal troponin collection using high-sensitivity cTnI assays, inclusion of troponin in future clinical trial outcomes and future development of clinical guidelines for monitoring and treating troponin elevations in DMD.
References
Footnotes
Contributors CS was responsible for data regarding troponin levels, clinical evaluation of troponin levels and imaging biomarkers, and wrote and revised the manuscript. DA was responsible for development of future recommendations and revised the manuscript. LCh was responsible for data regarding troponin levels in clinical trials and revised the manuscript. LCr was responsible for evaluation of troponin levels in clinical and research subjects and revised the manuscript. KH was responsible for imaging biomarkers in relation to troponin and clinical evaluation of troponin and revised the manuscript. NK and JM-S were responsible for developing future recommendations regarding analysis of existing data and prospective data collection and revised the manuscript. KK was responsible for foundation involvement in clinical care guidelines and trial design and revised the manuscript. EM was responsible for troponin assay analysis and clinical evaluation of troponin levels and revised the manuscript. LS was responsible for analysis of troponin levels in preclinical models of dystrophin deficiency. CV was responsible for clinical evaluation of troponin levels and development of future recommendations and revised the manuscript. LWM was responsible for clinical evaluation of troponin levels and recommendations for clinical guidelines and revised the manuscript.
Funding Funding for this meeting was provided by the Parent Project Muscular Dystrophy (PPMD).
Competing interests DA: consultant to PPMD/I-ACT for Children, no relevant conflicts. LC: employee and shareholder of Pfizer, Inc. NK and J-MS: Critical Path Institute is supported by the Food and Drug Administration (FDA) of the US Department of Health and Human Services (HHS) and is 62% funded by FDA/HHS totalling $14 448 917 and 28% funded by non-government source(s) totalling $8 669 646. The contents are those of the author(s) and do not necessarily represent the official views of, nor an endorsement, by FDA/HHS, or the US Government. EM: consultant to AstraZeneca, Amgen, Avidity, 4D Molecular Therapeutics, Pfizer, Janssen, Cytokinetics, Exonics and Invitae; grant support from NIH and Department of Defense.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information.