Article Text

Abstract
Background Point of care viscoelastic measures with thromboelastography (TEG; Haemonetics Corporation, Switzerland) and thromboelastometry (ROTEM, Tem Innovations GmbH, Germany) now supersede laboratory assays in the perioperative assessment and management of coagulation. To the best of our knowledge, this sophisticated coagulation assessment has not been performed to characterise thrombotic changes in the transcatheter aortic valve implantation (TAVI) setting, nor have the two latest iteration cartridge-based systems been directly compared in the elective perioperative period.
Methods Patients undergoing TAVI were prospectively recruited. Samples (n=44) were obtained at four timepoints (postinduction of anaesthesia, postheparin (100 IU/kg), postprotamine (1 mg/100 IU heparin) and 6 hours postoperatively). Each sample was concurrently assessed with standard laboratory tests (prothrombin time/international normalised ratio, activated partial thromboplastin time, thrombin clotting time, platelet count and direct fibrinogen, ROTEMSigma and TEG6s).
Results Clot strength showed a statistically significant increase postheparin/TAVI deployment. When considering the subgroup of samples taken following the administration heparin, the heparinase channel of the TEG6s did not yield clotting strength results in 55% of samples and clotting time exceeded the upper limit of normal in 70% of samples. It was retrospectively recognised that the arachidonic acid channel of the TEG6s Platelet Mapping Cartridge had been decommissioned prohibiting assessment of aspirin effect.
Conclusions This study demonstrated a small intraprocedural prothrombotic change of uncertain clinical importance during the transcatheter aortic valve procedure. Further comparison with percutaneous coronary intervention and aortic valve replacement cohorts are needed to assess the merits of current antithrombotic guidelines, which are extrapolated from the PCI setting. The heparin effect was more consistently quantified by ROTEM.
- transcatheter aortic valve replacement
- aortic valve stenosis
- heart valve prosthesis
- drug monitoring
Data availability statement
Data are available on reasonable request. Deidentified patient data are available on reasonable request from the corresponding author.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known about this subject?
Current intraoperative antithrombotic regimes for patients undergoing transcatheter aortic valve implantation (TAVI) are based on data and strategies extrapolated from percutaneous coronary intervention.
What does this study add?
This study assesses the prothrombotic changes that occur during the TAVI procedure using whole blood viscoelastic strategies and, to the best of our knowledge, provides the first comparison between the latest iteration viscoelastic haemostatic assays in an elective perioperative setting.
How might this impact on clinical practice?
A statistically significant intraprocedural prothrombotic signal was identified associated with TAVI. This requires comparison with percutaneous coronary intervention and aortic valve replacement to determine the suitability of current antithrombotic regimens. Findings also mandate further validation of the TEG6s in setting of both heparin and antiplatelet medications.
Introduction
Widespread acceptance of the cell-based model of coagulation and the ease and rapidity of use have increasingly emphasised testing whole blood with point-of-care viscoelastic haemostatic assays.1 The two most commonly used systems, thromboelastography or TEG (Haemonetics Corporation, Switzerland) and rotational thromboelastometry or ROTEM (Tem International GmbH, Munich, Germany) now supersede laboratory measures for the perioperative assessment of coagulation at many centres.2 Both devices have experienced recent iterations (TEG6 s and ROTEMSigma) composed of preprepared cartridges to which patient blood samples are added and automatically processed. Perioperatively, the information obtained allows for: sophisticated characterisation of coagulation (both coagulopathic and prothrombotic) and managing intraoperative bleeding and clotting issues.3–6
To our knowledge, the latest cartridge-based iterations of the two systems have not been directly compared in any elective perioperative setting. Additionally, the underlying temporal coagulation changes that occur due to the TAVI procedure itself have not been characterised—a necessary first step to determining the optimal antithrombotic regime.
Methods
Between March and May 2018, patients undergoing transcatheter aortic valve implantation (TAVI) at St. Andrew’s War Memorial Hospital, Australia, were recruited prospectively. Study methods were performed accordingly. Informed written consent was obtained from all eligible patients prior to enrolment.
Patients were consecutively screened for inclusion. All comers were considered, and key exclusion criteria were included: emergency procedures; haemoglobin <100 g/L; platelet count <100×109; known/suspected bleeding or clotting disorder (not including dual antiplatelet therapy or intraoperative heparin); ejection fraction <50%; severe liver, renal, respiratory or psychiatric disease; unable/unwilling to consent; or enrolment in another study with a non-standard therapeutic intervention.
Clinical management and assessment
Suitability for TAVI was determined by a multidisciplinary ‘heart team’. All procedures were performed transfemorally using the SAPIEN-3 (Edwards LifeSciences, Irvine, California, USA) prosthesis and under general anaesthesia. All patients received dual antiplatelet loading with 300 mg each of aspirin and clopidogrel within the preceding 24 hours and intravenous heparin (100 IU/kg) prior to valve deployment, which was reversed with protamine (1 mg/100 IU heparin).
A detailed preprocedure questionnaire and in-hospital preprocedure and postprocedure assessments sought to identify risk factors for and clinically apparent complications associated with bleeding and clotting. Bleeding/thrombosis relevant clinical events (including mortality, myocardial infarction, stroke, bleeding complications, vascular complications, conduction disturbances/arrhythmias and requirement for cardiac reintervention) were adjudicated by medical specialists independent of the treating team using the Valve Academic Research Consortium-2 consensus criteria.7
Coagulation assessment
Blood samples were collected at four timepoints: T0: postanaesthesia induction/preheparin; T1: postheparin (100 IU/kg) and TAVI deployment; T2: postprotamine (1 mg/100 IU heparin); and T3: 6 hours postprocedure (see figure 1). At each time point, blood was analysed with the ROTEMSigma analyser using a ‘complete+hep’ cartridge (with four channels: INTEM, EXTEM, FIBTEM and HEPTEM) and the TEG6s analyser with a citrated cartridge (with four channels: kaolin (CK), RapidTEG (CRT), kaolin/heparinase (CKH) and functional fibrinogen (CFF). Baseline platelet function was assessed using the TEG6s Platelet Mapping Cartridge (with four channels: kaolin/heparinase, reptilase/factorXIIIa/abciximab (ActivatorF or ActF), adenosine-5′-diphsophate/ActivatorF (ADP) and Arachdonic acid/ActivatorF (AA). Key study parameters were: time for clot initiation (clotting time (CT; s) for ROTEM, and reaction time (R; min) for TEG) and clot strength (maximum clot firmness (MCF; mm) for ROTEM, and maximum amplitude (MA; mm) for TEG). Standard laboratory tests of coagulation included prothrombin time (PT)/international normalised ratio, activated partial thromboplastin time (aPTT), thrombin clotting time and direct (Clauss) fibrinogen (Sysmex CS-5100) and full blood count (Sysmex SP-10, Sysmex Corporation, Kobe, Japan). All equipment was used and maintained according to manufacturer recommendations.
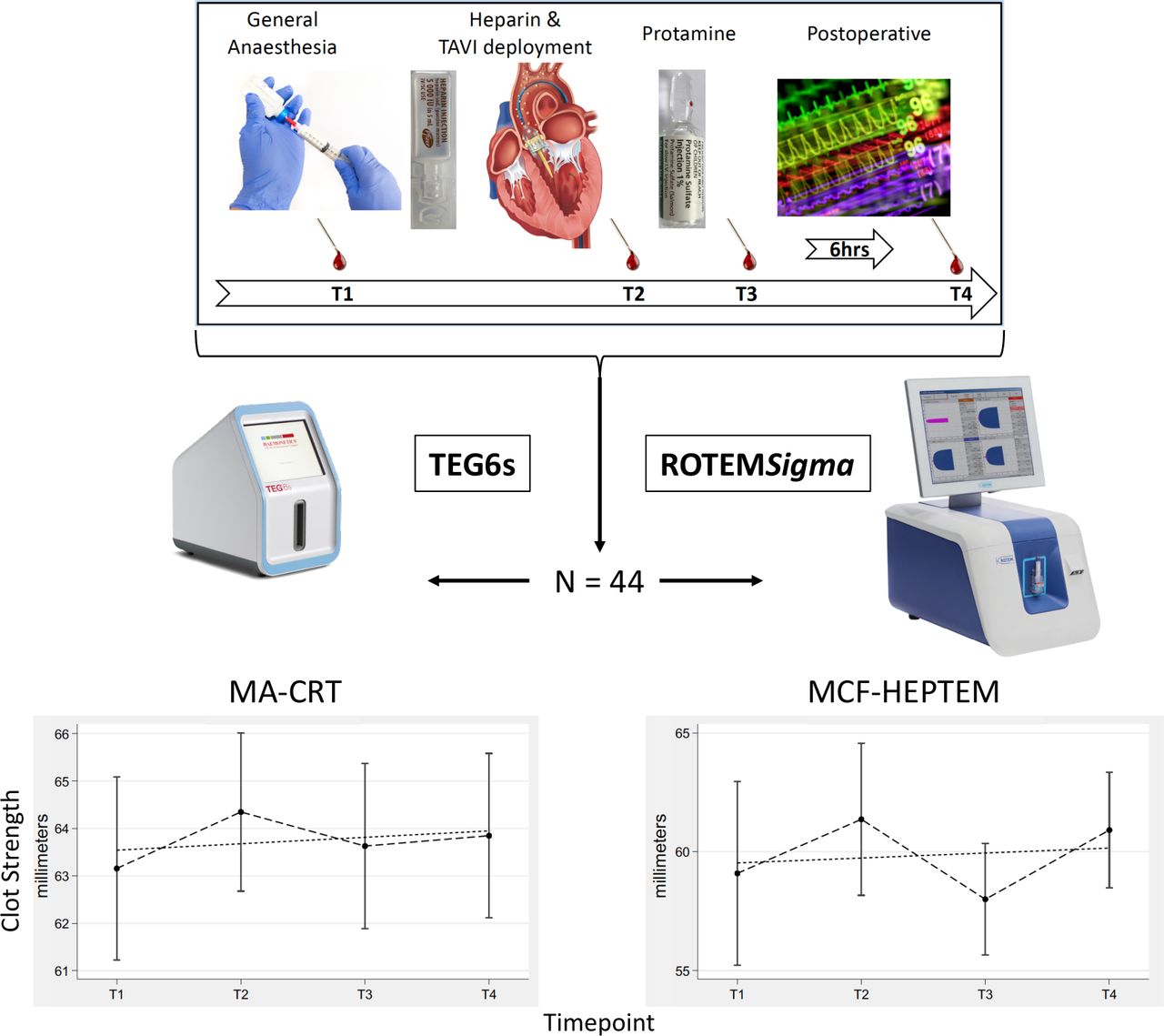
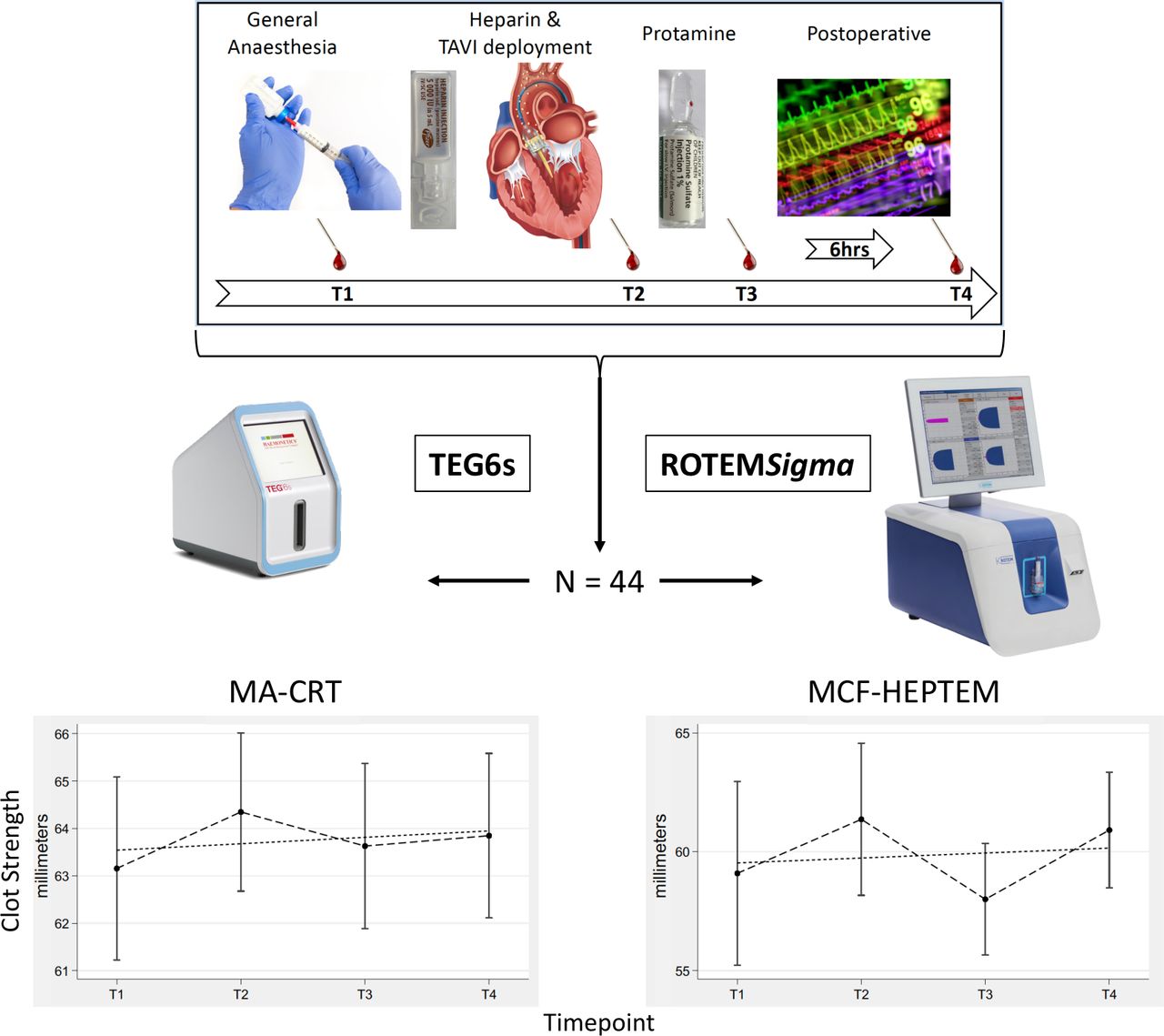{kind=link}
Clot strength measured using maximum amplitude of the citrated rapid TEG (MA-CRT) cartridge (left) and maximum clot firmness of the ROTEMSigma HEPTEM (MCF-HEPTEM) cartridge (right) both demonstrating a statistically significant prothrombotic effect following TAVI deployment, which is of uncertain clinical significance. TAVI, transcatheter aortic valve implantation.
Statistical analysis
Summary statistics are reported as: simple percentages (%); group means±SD compared via paired t-tests for normally distributed data; or medians±IQR compared using Wilcoxon paired sign-rank test. For each measure, changes from baseline were plotted over time as a categorical variable. Student’s t-tests were performed to identify any statistically significant changes from baseline. Corresponding TEG, ROTEM and laboratory measures were correlated by Pearson’s correlation. Highly correlated variables were then assessed for agreement using Bland-Altman plots. Univariate cross-sectional time-based random effects models were developed for each viscoelastic measure using the laboratory clotting indices, in turn, as the dependent variable. Both paired comparisons between timepoints and univariate time series regression were analysed for each variable. Changes over time were compared via paired comparisons between timepoints of each variable with baseline. Times were analysed as regular intervals despite being irregularly spaced. Analyses were performed using STATA V.13 (StataCorp, Texas, USA).
Results and discussion
Baseline characteristics
Forty-four samples were obtained from 11 patients undergoing TAVI. Their baseline characteristics are reported in table 1. Patients were a mean 84±5.9 years old, predominantly male (66%) and all had severe aortic stenosis (aortic valve area of 0.9±0.1 with mean aortic valve gradient of 36±8.5). The average TAVI procedure time was 26.6±3.9 min; no procedure required postimplantation manoeuvres. Serial clinical assessments revealed no clinically apparent bleeding or thrombotic events.
Clinically relevant patient and procedure characteristics
Binary comparisons between assays
Direct comparisons between complementary laboratory and viscoelastic clotting indices are summarised in table 2. Regarding clotting time, both PT and aPTT showed significant associations with the independent variables CT-activation of intrinsic pathway (INTEM) and R-CRT and an association was significant for CT-activation of extrinsic pathway (EXTEM) versus R-CRT. Regarding clot strength, significant associations with at least moderate correlations was evident for MCF-INTEM versus MA-CK, MCF-EXTEM versus MA-CRT and MCF-activation of extrinsic pathway and in vitro blocking of thrombocytes (FIBTEM) versus MA-CFF but not for the platelet function surrogate measure ΔMCF (MCF-EXTEM – MCF-FIBTEM) versus ΔMA (MA-CRT – MA-CFF).
Binary comparisons between corresponding assays
Platelet inhibition
Analysis of the ADP channel of the TEG6s Platelet Mapping Cartridge demonstrated that clopidogrel resulted in 32.2%±8.5% platelet inhibition with one non-responder (<10%) and three semiresponders (10%–30%). Over the course of the study, it became apparent that the AA channel was non-functional; consequently, results regarding the aspirin component of platelet inhibition are unavailable. Other assays of aspirin inhibition of platelet function, such as optical aggregometry (considered the gold standard assessment), electrode impedance aggregometry and flow cytometry also have well-recognised limitations for measuring the antiplatelet effects of aspirin. Alternative point of care testing systems were not logistically feasible at the time of recruitment.8–10
Characterising the changes that occur during TAVR
Temporal changes for each of the indices are summarised in table 3, and for clot strength, this is also demonstrated in the figure 1. As expected, CT was prolonged at T1 versus baseline and normalised by T2 for all measures. Fibrinogen was significantly lower than baseline at T1 but significantly higher at T3. MA-CRT showed a statistically-significant increase at T1, providing evidence of a prothrombotic change.
Temporal changes in coagulation assays over time
Quantifying and neutralising the heparin effect
When considering those samples taken at T1, TEG6s MA-CKH yielded no results in 55% of samples and R-CKH exceeded the upper limit of normal in 8/11 heparinised samples (median: 588 s; IQR 366–738) versus ROTEMSigma, where MCF-HEPTEM was determined in 100% of samples and both CT-HEPTEM (223 s; 212–229) and MCF-HEPTEM (60 mm; 58–66) were within the normal range for all samples. Thus, in our cohort, the CKH appeared insufficient to reverse the heparin effect. This occurred despite maximum activated clotting times (ACTs) <450 s, equivalent to heparin levels of <2 IU/mL, far below the 6 IU/mL capacity purported for the CKH channel.
Conclusions
This study demonstrated a small intraprocedural prothrombotic change of uncertain clinical importance during the TAVI procedure, and further comparison with PCI and AVR cohorts are needed to assess the merits of current antithrombotic guidelines, which are extrapolated from the PCI setting and basedon expert consensus.11 12 Baseline platelet mapping revealed that the aspirin contribution currently cannot be assessed with the TEG6s Platelet Mapping Cartridge, and alternative platelet function testing should be employed until manufacturing issues are sorted. Similarly, the TEG6s heparinase channel appeared unable to reverse the heparin effect despite modest ACTs, and this channel should not be relied on in any setting involving heparin until further investigated/validated.
Data availability statement
Data are available on reasonable request. Deidentified patient data are available on reasonable request from the corresponding author.
Ethics statements
Ethics approval
The study protocol received institutional ethics review board approval (EC00374, 2016.33.213).
Acknowledgments
The investigators would like to thank: the Heart Valve Programme at St Andrew’s War Memorial Hospital, Queensland; and, The Prince Charles Hospital Foundation for logistical assistance.
References
Footnotes
Contributors JPF conceived, designed, obtained funding, interpreted data and drafted original manuscript. SR, MM, KP, AI, SN and JF contributed to the design, acquired and interpreted data and critically reviewed manuscript. CA performed statistical analysis, interpreted data and critically reviewed manuscript.
Funding Project funding was obtained from the Wesley Medical Research Limited, Level 8 East Wing, 451 Coronation Drive, Auchenflower, QLD 4066, Australia (Ref: 2016–56). JPF was supported by a Fellowship from the Health Innovation Investment and Research Office (HIIRO) within the office of the Director-General, Department of Health, Queensland Government, Level 13, 33 Charlotte Street, Brisbane, QLD 4001, Australia.
Competing interests KP and AI have 'significant relationships' with Edwards LifeSciences and Abbott Vascular including consulting/proctoring fees and an unrestricted institutional grant.
Provenance and peer review Not commissioned; externally peer reviewed.