Article Text

Abstract
Transcatheter aortic valve implantation (TAVI) is a proven treatment for life-threatening aortic valve disease, predominantly severe aortic stenosis. However, even among developed nations, access to TAVI is not uniform. The Valve for Life initiative was launched by the European Association of Percutaneous Cardiovascular Interventions in 2015 with the objective of improving access to transcatheter valve interventions across Europe. The UK has been identified as a country with low penetration of these procedures and has been selected as the fourth nation to be included in the initiative. Specifically, the number of TAVI procedures carried out in the UK is significantly lower than almost all other European nations. Furthermore, there is substantial geographical inequity in access to TAVI within the UK. As a consequence of this underprovision, waiting times for TAVI are long, and mortality among those waiting intervention is significant. This article reviews these issues, reports new data on access to TAVI in the UK and presents the proposals of the UK Valve for Life team to address the current problems in association with the British Cardiovascular Intervention Society.
- heart valve prosthesis implantation
- transcatheter aortic valve replacement
- delivery of health care
- aortic valve stenosis
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- heart valve prosthesis implantation
- transcatheter aortic valve replacement
- delivery of health care
- aortic valve stenosis
Introduction
The Valve for Life initiative was launched by the European Association of Percutaneous Cardiovascular Interventions (EAPCI) in 2015 with the objective of improving access to transcatheter valve interventions across Europe. The approach has been founded on four tenets: to raise awareness of the importance of valvular heart disease in the general population, to facilitate access to transcatheter heart valve interventions, to raise educational standards and thereby reduce obstacles to therapy implementation and to diminish age and gender discrimination in the access to care.1
The objectives of Valve for Life are ambitious, requiring improved delivery of transcatheter valve interventions within countries as well as reducing disparities between them. Countries selected are those where penetration of transcatheter procedures is low; the Valve for Life programme is an opportunity to identify the obstacles that contribute to this and engage change. The inaugural Valve for Life initiative was launched in Poland and quickly made its mark, with the Polish Ministry of Health allocating sufficient funds to increase the number of transcatheter valve interventions by 20% for the following year.1 Subsequent projects in France and Portugal have been well received and successful, and the UK has been selected as the fourth country to be included in the programme. This article, focussing exclusively on transcatheter aortic valve implantation (TAVI) as the dominant established transcatheter valve therapy (TVT), will outline the nature and scale of the problem to be tackled in the UK and will describe the proposals of the UK Valve for Life team to overcome them.
The UK Valve for Life initiative
The UK Valve for Life initiative has been awarded a substantial grant (Appendix 1) by the EAPCI with the aim of supporting a comprehensive national project to improve delivery of TVTs. This grant has been collectively provided by all major transcatheter heart valve manufacturers. The initiative is spearheaded by a team of eight clinicians from different regions of the UK, each with an interest and expertise in valvular heart disease and working under the umbrella of the British Cardiovascular Intervention Society (BCIS). In order to increase patient access to transcatheter heart therapies, the team will lobby NHS England and the Department of Health and Social Care in order to promote the agenda of increasing provision for the management of valvular heart disease.
The team will also interact directly with trusts, through designated ‘local champions’ who work at regional heart valve centres, with the intention of implementing pathways designed to improve service provision. Finally, there will be an emphasis placed on increasing awareness among clinicians and the public through educational programmes and media activities.
The UK deficit in TAVI
National underprovision
The number of TAVI procedures performed in the UK per head of population is currently significantly lower than almost all other European nations (figure 1A). In 2019, for example, 78 TAVI procedures per million population (pmp) were undertaken, compared with a European average of 141 pmp and as high as 292 pmp in Germany.

(A) Comparison of number of TAVI procedures carried out per million population in different European countries. (B) Comparison of number of TAVI centres per million population in different European countries. TAVI, transcatheter aortic valve implantation.
Multiple factors are likely to explain the low relative number of TAVI procedures carried out in the UK. First, the number of TAVI centres in the UK is small, with only 0.53 centres per million population, around one-third the average in Western Europe (figure 1B). Second, capacity in existing centres is limited. In a survey conducted of UK TAVI centres, inadequate cardiac catheterisation laboratory capacity and bed numbers were most frequently identified as the factors limiting the expansion of TAVI numbers (stated to be the main factor or a significant factor in 74% and 56% of respondents, respectively). Access to cardiac CT was also a common problem, with 45% of respondents citing this as the main factor or a significant factor. Finally, limitations on TAVI numbers imposed by commissioners also impact on procedure volume in many centres; 35% of respondents identified this as the main factor or a significant factor preventing expansion of TAVI numbers.
Inequity of access within the UK
In addition to underprovision of TAVI in the UK as a whole, there is also substantial geographic inequity within the NHS. We analysed the rate of TAVI procedures per million according to NHS England Clinical Commissioning Group, NHS Wales Health Board and nationally in Scotland and Northern Ireland, using data obtained from the National Institute for Cardiovascular Outcomes Research (figure 2). This analysis shows an 11-fold variation in TAVI numbers pmp, ranging from 194 to 17.2. In total, 39 areas had fewer than 50 TAVIs pmp, and 48 over 100, a remarkable disparity. Although a degree of geographical variation is inevitable and may be driven by differences in the local population, in particular, with respect to age, such profound regional differences cannot be explained solely by demographics.

An illustrative representation of the geographical variation in TAVI procedures carried out in the UK in 2019. TAVI, transcatheter aortic valve implantation.
Transcatheter Aortic Valve implantation (TAVI)
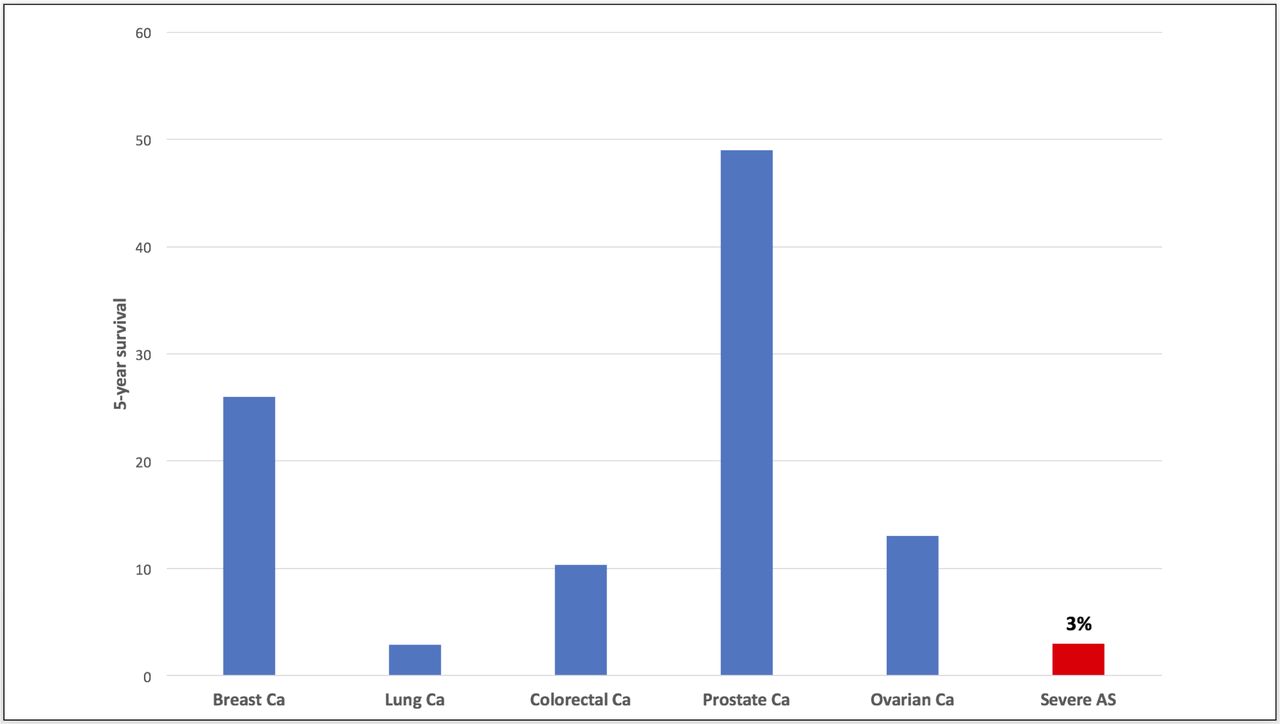
Aortic stenosis (AS) is one of the most common forms of valvular heart disease, with approximately 5% of adults over the age of 65 affected,2 and is invariably progressive. Once stenosis is severe, symptoms of breathlessness, angina and syncope follow. Quality of life (QOL) declines and the prognosis is poor, with 50% of patients dead within 2 years of symptom onset and a mortality rate at 5 years of 97%.3 As illustrated in figure 3, this is worse than the mortality associated with metastatic breast, colorectal, prostate or ovarian cancers and is comparable to metastatic lung cancer.4

A comparison of the prognosis of untreated severe AS to the most common metastatic cancers in the UK. Figures for cancer survival obtained from the Office of National Statistics (ONS). AS, aortic stenosis; Ca, carcinoma.
Until the early 2000s, surgical aortic valve replacement (SAVR) was the only treatment for severe, symptomatic AS that had been demonstrated to improve mortality.5 However, open heart surgery is a major procedure with significant inherent risks, particularly in an elderly patient cohort. As such, a substantial proportion of patients (30%–40%) with severe, symptomatic AS is turned down for SAVR due to advanced age and/or comorbidity.6 TAVI is a minimally invasive procedure that allows transcatheter deployment of a replacement valve using arterial access and avoiding any major surgical intervention. The first TAVI was carried out in 2002 and the subsequent adoption and expansion of TAVI within routine clinical practice have revolutionised the treatment of severe, symptomatic AS. The success of TAVI has been built on evidence from landmark studies; the PARTNER (Placement of AoRtic TraNscathetER Valve) 1B trial demonstrated that TAVI was associated with a 50% reduction in mortality compared with medical therapy among inoperable patients with severe, symptomatic AS,7 while PARTNER 1A showed TAVI to be noninferior to SAVR in high surgical risk patients.8 9 Subsequent to this, use of TAVI has expanded into lower risk patient cohorts, and a number of studies have demonstrated outcomes following TAVI to be at least equivalent to SAVR in intermediate and low surgical-risk patients.10–14
In addition to excellent clinical outcomes in comparison to SAVR, TAVI is much less invasive, with a significantly reduced hospital stay, more rapid recovery and far less consumption of hospital resources. TAVI is percutaneous and performed under local anaesthetic in >95% of patients in the UK. In the UK TAVI randomised trial, median hospital stay was 3 days for TAVI compared with 8 days for SAVR, median intensive care unit (ICU) bed day use was zero in the TAVI group, and QOL was improved after only 2 weeks in comparison to 6 months after SAVR.14 Minimisation of hospital stay, avoidance of ventilation and use of ICU, and more rapid recovery with TAVI in contrast to SAVR may be of particular merit in the era of the COVID-19 pandemic, when the premium placed on preserving healthcare resources and minimising hospital contact is even more profound.
The impact of underprovision of TAVI in the UK
Waiting lists
Across the NHS, demand for TAVI far outstrips capacity, and as a result, patients with this debilitating and life-threatening condition face long waits for treatment. We performed an analysis of waiting times for TAVI in the NHS in 2019. Among 23 centres from which data were obtained, the median waiting time from referral to TAVI was 141 days—over 20 weeks (table 1). Geographical inequity in waiting times is also evident, with the median time from referral to TAVI varying from 9 weeks to 35 weeks. Furthermore, these times do not take into account the delay from the onset of symptoms to assessment by a general practicioner, followed by referral to a local hospital, and then eventual referral to the TAVI centre.
Data from a survey of UK TAVI centres demonstrating the average waiting time from referral to TAVI during 2019
Mortality
Since the median survival of severe symptomatic AS is worse than almost any metastatic cancer, it is not unexpected that inadequate capacity and long waiting lists translate to mortality. A study published in 2014 showed that a delay to TAVI of 6 months led to almost a quarter of patients (23.3%) dying on the waiting list.15 In our survey of 23 UK TAVI centres, there were 299 deaths among patients awaiting TAVI in 2019. If extended to all 35 centres performing TAVI in the UK, this would translate to over 500 avoidable deaths annually. Again, there was significant geographical variation, with the number of deaths per centre for patients awaiting TAVI ranging from 1 to 40.
Hospitalisation
As well as death, a long wait for TAVI often leads to clinical deterioration and acute hospital admission. In our analysis from 23 UK TAVI centres, 22% of TAVI procedures were in hospitalised patients. The median hospital stay was 33 days among in- patients, compared with 3 days for those treated from home. A focused analysis in one large centre revealed that 39% of urgent in-patient procedures were in subjects who had already been accepted for TAVI and were on a waiting list but had decompensated. It is clear, therefore, that the long waits for TAVI seen in the NHS not only result in unnecessary deaths but also in the avoidable consumption of hospital beds.
Valve for Life TAVI proposals
Introduction of a fast-track TAVI pathway
There is currently no specific treatment time target for TAVI in the UK. NHS policy mandates a maximum waiting time for non-urgent, consultant-led treatments of 18 weeks and this is used as a target from time of referral to treatment in the case of SAVR. However, this is not consistently applied to TAVI, and as our survey shows, is not being achieved across UK centres; fewer than half of the 23 centres which provided data reported a median time from referral to TAVI of ≤18 weeks (11/23; 47.8%).
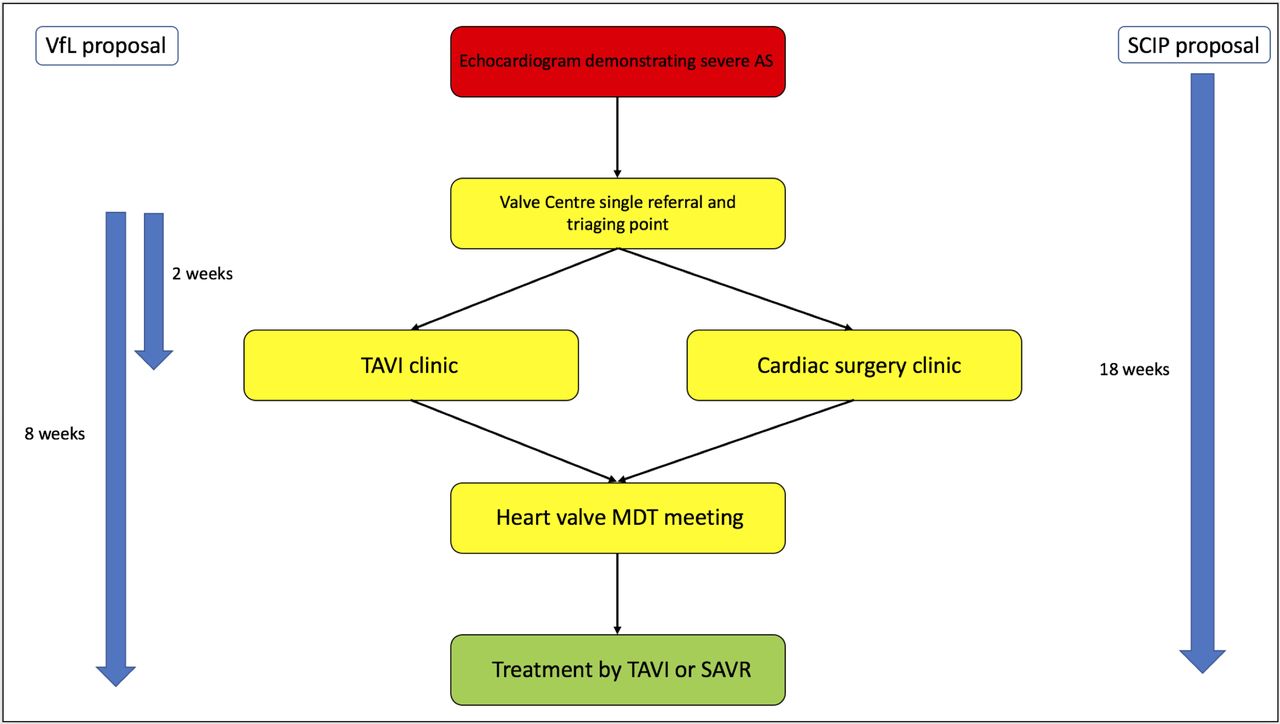
Since severe symptomatic AS has a prognosis similar to or worse than metastatic cancer, Valve for Life proposes that an analogous fast-track pathway template used for the investigation and treatment of suspected cancer is applied to the management of AS, whether by TAVI or SAVR (figure 4). The cancer pathway targets are 14 days from referral to being seen in a specialist clinic, 31 days from decision to treat to definitive treatment and 62 days in total from time of referral to start of treatment. We propose that centres offer a single common pathway for AS, incorporating surgical or TAVI clinic appointment within 2 weeks. Following outpatient assessment, patients would be discussed at the heart valve multidisciplinary team (MDT) meeting and undergo valve intervention, if appropriate, with a target of 8 weeks in total from referral to treatment.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Proposal for a new fast-track TAVI pathway showing valve for life targets as well as the NHS England Specialised Cardiac Improvement Programme (SCIP) 18 week target from diagnosis to treatment. AS, aortic stenosis; MDT, multidisciplinary team; SAVR, surgical aortic valve replacement; SCIP, Specialised Cardiac Improvement Programme; TAVI, transcatheter aortic valve intervention.
The Valve for Life fast-track pathway for TAVI is consistent with proposals from the NHS England Specialised Cardiac Improvement Programme (SCIP). SCIP is yet to report its final recommendations but is proposing a similar accelerated pathway for AS, which is likely to include a recommendation for a maximum 18-week wait for treatment of severe symptomatic AS from the time of diagnosis. If implemented, this would address the delays patients often face before referral to the Valve centre is made. The 8-week target from referral to treatment proposed by Valve for Life would fit into this overall 18-week pathway.
Delivering a fast-track pathway
The 8-week treatment target will be a mandatory requirement against which individual providers are measured. Such a centrally mandated NHS pathway will require hospitals to prioritise allocation of resources to valve services in order to meet the targets. Nevertheless, we recognise that delivering definitive treatment by TAVI or SAVR within 8 weeks of referral would represent a major challenge for centres across the NHS. Valve for Life will propose a number of measures to help meet this ambitious but essential target.
Single referral point
All referrals for treatment of AS would be received through a single referral point. The Valve team would assign each patient a priority rating based on clinical urgency, triage patients to SAVR, TAVI or a joint clinic as appropriate, and ensure all required investigations had been performed or were planned.
Streamlining referral and investigation
Invasive coronary angiography would no longer be mandated prior to referral, with CT coronary angiography used both for the exclusion of significant coronary artery disease and for assessment of vascular access and aortic valve anatomy prior to TAVI or SAVR. In cases where invasive angiography was felt to be necessary, this would be arranged at the point of triage. CT would be performed in the referring centre where possible, or otherwise at a one-stop visit to coincide with the outpatient appointment at the specialist Valve centre. All other assessments, including consultant review, appraisal by the valve nurse specialist including frailty assessment, ECG and transthoracic echocardiography, would be performed at the one-stop clinic.
Maximising capacity in existing TAVI centres
Advances in technology, as well as refinement of technique, have led to streamlining of the TAVI procedure, enabling a minimalist TAVI approach. This allows a shorter procedure time, and, hence, more patients to be treated on a list as well as more rapid recovery and reduced hospital stay. However, adoption of minimalist TAVI in the UK is highly variable. While many centres now perform four or more fully percutaneous procedures per day without general anaesthesia, with postoperative care in a level 1 bed, and with discharge 1–2 days postprocedure, this is by no means universal. Valve for Life proposes a series of benchmarking standards, described in table 2, that would be audited nationally and would require all centres to deliver the TAVI procedural pathway as efficiently as possible. The Valve for Life team will work with the identified local champions in each heart valve centre to streamline the local TAVI service, in order to optimise capacity and enable the fast-track pathway to be delivered.
Proposed valve for life benchmarking standards for TAVI
Achieving a fast-track TAVI pathway may also require an increase in capacity, particularly, in those areas where procedural numbers are low and waiting lists long. The data obtained and described in detail above would be used to target those TAVI centres where these problems are most marked, and where increasing as well as optimising capacity may be needed. This aspect of our proposals is currently being formulated in a combined initiative between BCIS and Valve for Life and will be presented in detail in a formal report. It is important to recognise that increasing the number of TAVIs that centres can undertake will also require greater capacity for pre-TAVI workup. Specifically, availability of pre-TAVI clinic appointments, CT scans and MDT meetings would need to be increased. Such measures will require a collaborative effort between departments as well as meaningful financial investment.
Expanding the number of UK TAVI centres
The number of TAVI centres in the UK is the lowest in Europe by population (figure 1B). The current arrangement in the UK is that only cardiac surgical centres offer TAVI, leading to a hub-and-spoke model, whereby district general hospitals refer patients to surgical centres. At present, every cardiac surgical centre in the UK provides a TAVI service. Therefore, increasing the number of TAVI centres would require expansion into hospitals without on-site cardiac surgery. Such a strategy may prove challenging due to concern that a lack of on-site surgical back up in the event of a complication could compromise procedural safety. Furthermore, the absence of surgical colleagues may pose challenges for the MDT approach that underpins TAVI. However, it is worth noting that existing data show that the need for emergency surgery is low, and that the number of patients saved as a result is very small. A study published in 2018 including 27 760 patients who underwent TAVI between 2013 and 2016 examined the incidence and outcomes of emergency cardiac surgery following complications related to transfemoral TAVI.16 The authors found that only 0.76% of patients who underwent TAVI required emergency cardiac surgery, and that this was associated with a high mortality as 78% of these patients died within 12 months. When looking at the study population as a whole, only 0.16% of patients had emergency surgery and then survived for 12 months. Applying this to the UK TAVI population, if we use the number of TAVIs performed between 2018 and 2019, the provision of emergency cardiac surgery would have allowed nine patients to survive 1 year or more; significantly fewer than died while waiting for TAVI.
It is acknowledged that expansion into smaller nonsurgical centres with potentially lower procedural volume may compromise patient outcomes. Data from the US TVT registry of almost 100 000 patients who underwent TAVI at over 500 sites showed reduced mortality in the highest volume centres (86–371 TAVI/year) when compared with the lowest volume centres (5–36 TAVI/year).17 However, the difference in 30-day mortality (2.66% vs 3.19%) was small, particularly when set in the context of the 2%–3% mortality per month for patients on a TAVI waiting list. Expansion in centre numbers may, therefore, have a significant net benefit even if accompanied by a small but measurable increase in procedural mortality.
Clearly, developing TAVI programmes at nonsurgical centres would require careful planning. Robust definitions of the necessary processes and services for such programmes to be run safely would be required. Close collaboration with the neighbouring surgical TAVI centre would be essential: cardiac surgical involvement in the MDT process would be a prerequisite; prospective TAVI operators would need to be trained and mentored; careful collaborative patient selection, with referral of complex cases to the surgical centre, would be required and provision for transfer for emergency cardiac surgery in the rare event of catastrophic procedural complications would need to be in place.
At present, we believe that optimisation and maximisation of capacity in existing surgical centres should be the priority. Valve for Life plans are to focus on delivery of the fast-track pathway and expansion of TAVI numbers in the UK by supporting growth in existing surgical centres, with particular attention to those centres in areas where access to TAVI is most constrained. However, if this strategy proves ineffective, we believe that expansion into new centres is an option that should be considered, particularly in areas where access to TAVI continues to be limited. Under such circumstances, Valve for Life would plan to work with BCIS to define the service specification for a TAVI centre without on-site cardiac surgery, so that this option may be explored.
Conclusions
Transcatheter valve interventions have revolutionised the management of valvular disease, providing evidence-based treatments for patients with no other definitive therapy options as well as offering a minimally invasive alternative to traditional surgery. TAVI is a proven and highly effective treatment for a disease whose impact on both patients and healthcare systems is profound. Regrettably, the UK lags behind the majority of European countries with regard to TAVI, and we have shown that this underprovision is associated with inequity of access to treatment, long waiting lists, avoidable and wasteful use of hospital resources and significant numbers of deaths among untreated patients.
The Valve for Life programme offers a hugely valuable opportunity to address these issues. We believe that the proposed measures have the potential to substantially improve the care given to patients across the NHS who are suffering from AS. The objectives of the Valve for Life programme are ambitious, but we hope that the UK experience will be as successful as previous initiatives and leave a lasting legacy that will benefit patients for years to come.
References
Footnotes
Contributors NA and DJB were involved in writing the manuscript. AF was involved in collecting data described within the manuscript. PL provided data and generated figures. All authors were involved in the critical appraisal and modification of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.