Article Text

Abstract
Objectives Transcatheter aortic valve replacement (TAVR) is increasingly performed. Physically small Asians have smaller aortic root and peripheral vessel anatomy. The influence of gender of Asian patients undergoing TAVR is unknown and may affect outcomes. The aim of this study was to assess sex differences in Asian patients undergoing TAVR.
Methods Patients undergoing TAVR from eight countries were enrolled. In this retrospective analysis, we examined differences in characteristics, 30-day clinical outcomes and 1-year survival between female and male Asian patients.
Results Eight hundred and seventy-three patients (54.4% women) were included. Women were older, smaller and had less coronary artery and lung disease but tended to have higher logistic EuroSCOREs. Smaller prostheses were used more often in women. Major vascular complications occurred more frequently in women (5.5% vs 1.8%, p<0.01); however, 30-day stroke and mortality (women vs men: 1.5% vs 1.6%, p=0.95% and 4.3% vs 3.4%, p=0.48) were similar. Functional status improvement was significant and comparable between the sexes. Conduction disturbance and permanent pacemaker requirements (11.2% vs 9.0%, p=0.52) were also similar as was 1-year survival (women vs men: 85.6% vs 88.2%, p=0.25). The only predictors of 30-day mortality were major vascular injury in women and age in men.
Conclusions Asian women had significantly smaller stature and anatomy with some differences in clinical profiles. Despite more frequent major vascular complications, women had similar 30-day stroke or mortality rates. Functional status improvement was significant and comparable between the sexes. Conduction disturbance and permanent pacemaker requirements were similar as was 1-year survival.
- transcatheter aortic valve replacement
- aortic valve stenosis
- heart valve prosthesis implantation
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known about this subject?
Although many studies have examined sex differences in transcatheter aortic valve replacement (TAVR) in Western countries, there are no data for sex differences in TAVR in Asia.
What does this study add?
Despite the very small stature and more major vascular injury, Asian women have similar 30-day outcomes, functional status improvement, permanent pacemaker requirements and 1-year survival as Asian men, comparable with previously published studies on gender differences in TAVR.
How might this impact on clinical practice?
Gender does not affect outcomes after TAVR in Asian patients and should not be a factor taken into consideration when assessing Asian patients for TAVR.
Introduction
Transcatheter aortic valve replacement (TAVR) has rapidly evolved to become an established treatment for patients with severe aortic valve stenosis who are inoperable or at high surgical risk1 2 and an attractive alternative in intermediate-surgical-risk and low-surgical-risk patients.3–6
TAVR was introduced in Asia in 2009,7 and the procedure has been increasingly performed in many centres and countries. There are now several reports demonstrating that women have outcomes comparable with men after TAVR in Western populations.8–16 However, data on the influence of gender on outcomes after TAVR in an Asian population are lacking, and there has only been a single report of a multicentre Asian registry.17 Asians are of smaller stature, and Asian women, in particular, have the smallest physique compared with other ethnic groups. It has been shown that Asians have smaller annulus and lower left coronary height than Caucasians,18 and Asian women have a significantly smaller iliofemoral anatomy than Asian men.19 Thus, the aims of this study were to assess the sex differences and outcomes of TAVR in Asian patients.
Methods
Eight hundred and seventy-three patients undergoing TAVR from centres in eight countries across Northeast Asia and Southeast Asia were retrospectively included on all-comers basis in this observational registry. All centres underwent training and proctoring of the initial cases according to the manufacturers’ protocols. Both high-volume and low-volume centres were eligible to participate.
All procedures were performed either with the balloon-expandable transcatheter heart valve (THV) or with the self-expanding THV. The balloon-expandable Edwards Sapien XT valve was delivered via the NovaFlex (18–19 French introducer sheaths) and then subsequently via the NovaFlex+ systems (16–18 French e-sheaths). Medtronic CoreValve prosthesis was delivered via the Accutrak (18-French introducer sheath) system.
Patient selection
Patients were enrolled if they were inoperable for surgical aortic valve replacement or if they were deemed to be at high surgical risk. High surgical risk was defined as a logistic EuroSCORE ≥20% or a Society of Thoracic Surgeons Predicted Risk of Mortality ≥8% or a consensus opinion of two cardiothoracic surgeons/TAVR heart team.
Valve sizing
Early in the experience, echocardiography and angiography were the main imaging modalities used for valve sizing and for access site assessment. Subsequently, CT angiography became widely used and, where possible, was performed for nearly all cases of valve sizing and peripheral access measurements due to its superior spatial resolution.
End points
All end points were defined according to the Valve Academic Research Consortium -2 criteria.20 They were site-reported, and there was no central adjudication. Baseline demographics, procedural parameters, in-hospital and 30-day outcomes and, where available, 1-year outcomes were recorded. The primary safety outcome was all-cause mortality at 30 days.
Statistical analysis
Continuous variables are presented as mean±SD and were compared between groups through the use of a two-sample t-test. Categorical variables are given as frequencies and percentages and were compared by the χ2 test or Fisher’s exact test. A value of p<0.05 was considered statistically significant.
The Kaplan-Meier survival analysis was used to estimate the unadjusted 1-year survival rate. Cox regression analysis was used to identify possible predictors of mortality. The first step was selection of the variables using univariate analysis. Significant variables (p≤0.1) were included in the multivariate model using stepwise Cox regression. Statistical significance remained the conventionally defined p≤0.05 in the univariate and multivariate models. Statistical analyses were performed with SPSS V.20 (SPSS).
The study was investigator-led, and no industry funding was obtained. Each centre obtained local ethics committee approval for the study (including waiver of consent). There was no patient or public involvement in the study. The investigators take responsibility for the integrity of the data and have read and agree to the manuscript as written. We used the Strengthening the Reporting of Observational Studies in Epidemiology cohort checklist when writing our report.
Results
Demographics
The mean age was 80±7.2 years, and 54.4% were women, with women being older (80.8±6.8 years vs 78.9±7.5 years, p<0.001). The average female height was 149.4±7.0 cm (vs men 163.3±7.1 cm, p<0.001), and the corresponding body surface area (BSA) was 1.47±0.17 m2 versus 1.67±0.17 m2, respectively (p<0.001). Women had less comorbidities of smoking, coronary artery disease including percutaneous coronary intervention or bypass graft surgery, and lung disease (table 1). More women had prior valve surgery and tended to have a higher logistic EuroSCORE (19.3±14.9 vs 17.5±13.6, p=0.07). The mean left ventricular ejection fraction (LVEF) was higher, and the annulus diameter was smaller in women (table 1).
Clinical characteristics
Procedural parameters
Slightly more CoreValves (52.7%) were used, less frequently in women compared with men (44.2% vs 62.8%, p<0.001). Conversely, the Sapien valve was used in 413 patients (47.3%), more frequently in women compared with men (55.8% vs 37.2%, p<0.001). The transfemoral route was the access approach in 83.8% of women versus 88.2% of men (p=0.06). Valve sizes ≤23 mm were used more frequently in women (51.4% vs 10.6%, p<0.001), whereas valve sizes ≥29 mm were used less frequently in women (11.0% vs 47.1%, p<0.001). Procedural success was high and similar (women vs men: 98.3% vs 98.5%, p=0.85) in both sexes (table 2).
Procedural parameters and outcomes
Clinical outcomes
Women experienced more major vascular complications (5.5% vs 1.8%, p=0.006) but had a lesser incidence of ≥mild paravalvular leaks (28.8% vs 35.9%, p=0.02), without any difference in the incidence of moderate/severe paravalvular leaks (2.7% vs 4.5%, p=0.16) (table 3). Mean pressure gradients were similar (women vs men: 11.0±6.0 mm Hg vs 10.6±5.7 mm Hg, p=0.40); women had a smaller mean aortic valve area (AVA) (1.6±0.4 cm2 vs 1.9±0.5 cm2, p<0.01), although there was no difference in the indexed AVA (1.09±0.30 vs 1.12±0.32, p=0.33) (table 3). Both sexes derived comparable symptomatic benefit with a 30-day mean New York Heart Association (NYHA) class of 1.5±0.6 (from NYHA class 2.8±0.7), with only 5.7% of women and 4.8% of men remaining in NYHA class III or IV (p=0.82). There was no difference in the incidence of new left bundle branch block (women vs men: 14.5% vs 14.7%, p=0.99) or permanent pacemaker requirement (overall 9.4%; women vs men: 11.2% vs 9.0%, p=0.52).
Thirty-day clinical outcomes
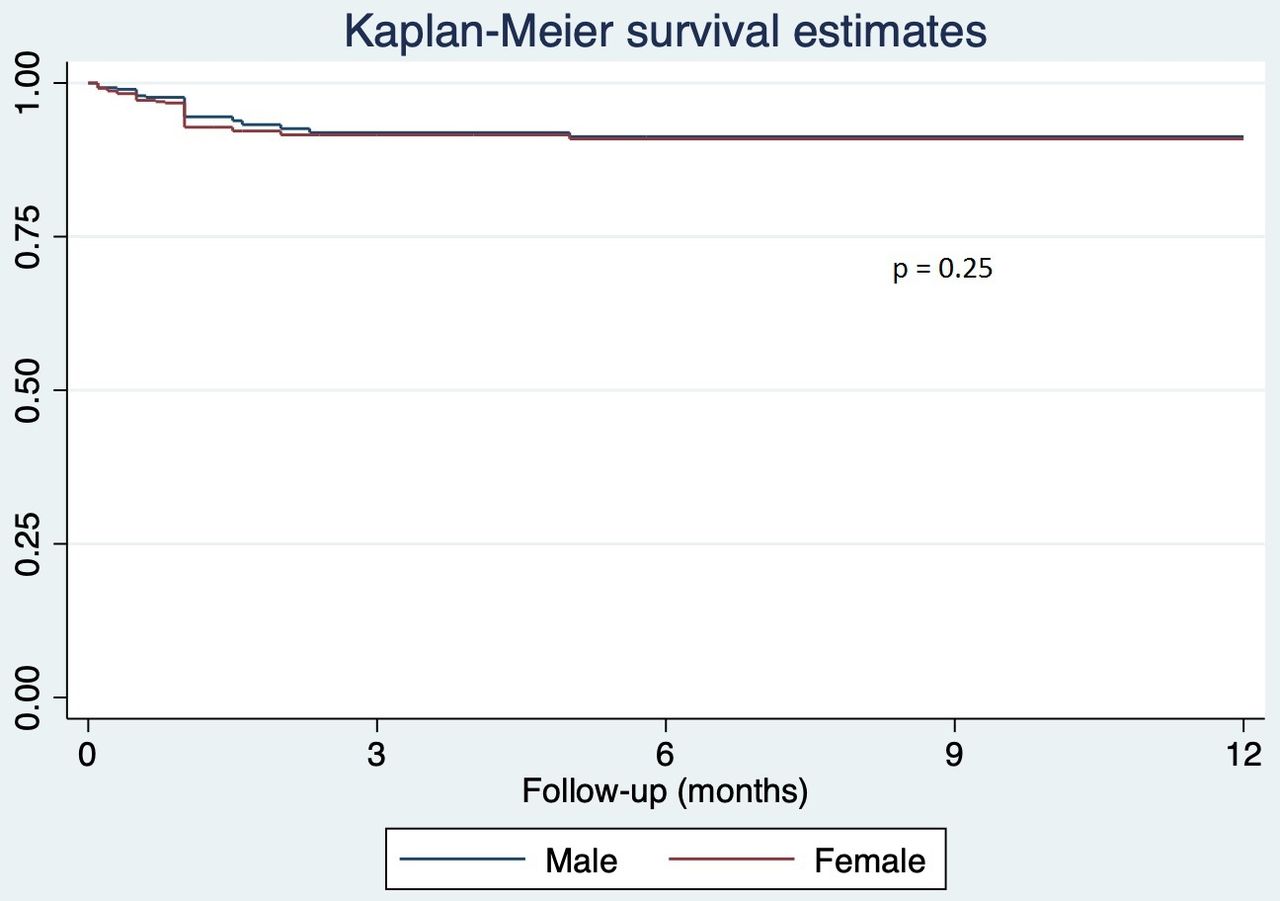
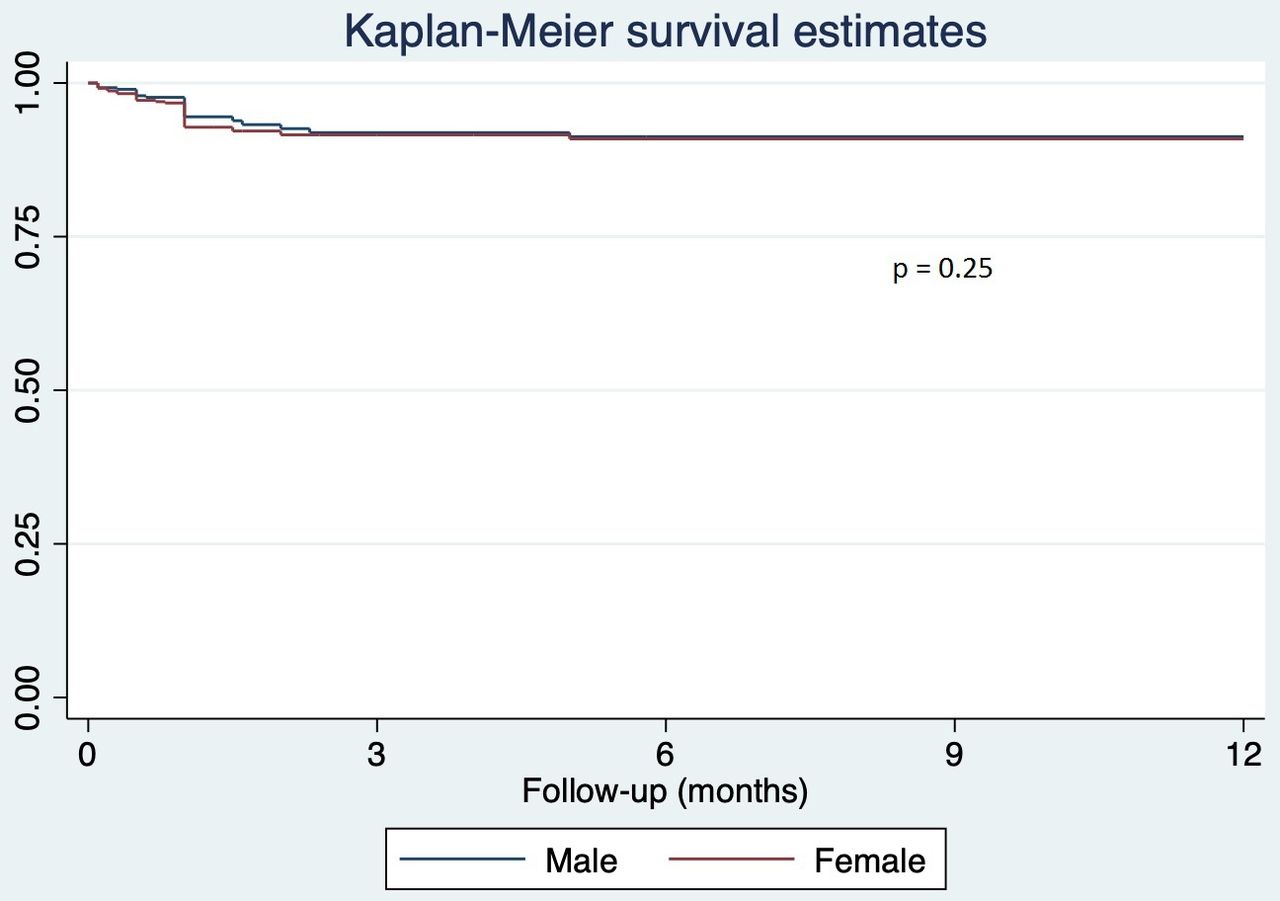
The 30-day mortality was 3.8%, with no difference between women and men (4.3% vs 3.4%, p=0.48). The 30-day stroke rate was also similar (women vs men: 1.5% vs 1.6%, p=0.95). Survival at 1 year was 85.6% in women and 88.2% in men (p=0.25) (figure 1).
{kind=link}
One-year Kaplan-Meier survival curves of women versus men.
On multivariable analyses, predictors of major vascular injury were age (OR 1.08, 95% CI 1.02 to 1.16, p=0.011) and female sex (OR 2.81, 95% CI 1.02 to 7.74, p=0.046), whereas BSA or body mass index (BMI) was not associated.
Predictors of 30-day mortality were age (OR 0.93, 95% CI 0.88 to 0.99, p=0.016) and major vascular injury (OR 11.66, 95% CI 3.28 to 41.41, p<0.001) for the entire cohort—major vascular injury only for women (OR 21.70, 95% CI 4.17 to 112.79, p<0.001) and age only for men (OR 0.87, 95% CI 0.80 to 0.95, p=0.002). Predictors of 1-year mortality were logistic EuroSCORE (OR 1.05, 95% CI 1.02 to 1.08, p=0.004), hypertension (OR 20.65, 95% CI 2.21 to 192.64, p=0.008), moderate or more paravalvular leak (OR 43.52, 95% CI 5.38 to 352.07, p<0.001) and 30-day NYHA class III or IV (OR 8.90, 95% CI 1.82 to 43.64, p=0.007) for the entire cohort; no separate analysis stratified by sex was performed due to the low end point count.
Discussion
Transcatheter aortic valve replacement (TAVR) is increasingly performed in Asia after a relatively late start.21 Several studies have now examined TAVR in an Asian population,17 22 23 with the majority of data from the Japanese Optimised transCathEter vAlvular iNtervention (OCEAN)-TAVR registry, which is specific, however, to one Asian ethnic group and to the balloon-expandable device. Data comparing gender differences in a broad geography of Asia and across various Asian ethnicities are lacking. Our study is the first description of sex-related differences in patients undergoing TAVR across Asia and across the various Asian ethnic groups.
An interesting and unique finding was the very small physical stature (eg, average height ≈149 cm) in elderly female Asians. Female patients had better LVEF and less comorbidities with respect to coronary artery disease, smoking and chronic lung disease, but were older and more likely to have had prior heart valve surgery, resulting in a trend towards a higher logistic EuroSCORE. With the smaller physical stature, smaller aortic annulus and, as shown in a previous study, smaller iliofemoral dimensions,19 the transfemoral route was used slightly less frequently, and the prostheses used in women were also smaller in size. However, mild or more paravalvular leak was also less frequent in women.
Despite more serious vascular complications occurring in female patients, the 30-day rates of stroke or mortality were low and similar between the sexes. Of note, most, if not all, centres were beginning their TAVR programmes, and most of the valves used were second-generation balloon-expandable or self-expanding valves. Functional status improved significantly and uniformly for both sexes; NYHA class III or IV at baseline was 67.5% in women versus 65.3% in men (p=0.35) to 5.7% in women and 4.8% in men at 30 days (p=0.92). At 1 year, there was no difference in survival between the sexes, despite women being older and having a trend towards a higher baseline EuroSCORE. The 1-year mortality somewhat approximated the baseline logistic EuroSCORE and is concordant with the findings from a previous Asian registry.17
Our data are consistent with several studies showing no difference in 30-day or 1-year survival between the sexes despite a higher incidence of major vascular complications,8 11–13 24 25 although some studies demonstrate that women have a better 1-year or long-term survival after TAVR.10 11 14 16 Although we did not record the iliofemoral dimensions in this study, it has been shown in a previous study by the first author that Asian women had significantly smaller iliofemoral dimensions than Asian men.19 In that study, the minimal femoral diameters were 6.3±1.5 mm versus 7.3±1.8 mm in women and men, respectively (p<0.001). The BSA of both sexes in that study was nearly identical with the current results (women vs men: 1.5±0.2 vs 1.7±0.2, p<0.001 in the previous study compared with 1.47±1.7 vs 1.67±1.7, p<0.001 in this study), indicating that the physical stature of the study populations was similar. As there was no difference in the incidence of peripheral artery disease between the sexes and interestingly because BSA or BMI was not associated with major vascular injury, the higher rate of major vascular complications in women in our study may be attributed to smaller ilio-femoral dimensions, older age and female sex itself (both of these may arguably be markers of vessel fragility).
More importantly, our study demonstrated that TAVR could achieve an equally good outcome for Asian women despite their smaller size and anatomy and higher incidence of major vascular complications. In contrast, it has been shown in some studies that a smaller height and female sex may be correlated with increased mortality after surgical TAVR25–27; thus, it is reassuring that physically small Asian women do not experience increased short-term mortality after TAVR. In concordance with Western data, women had less comorbidities associated with coronary artery disease and lung disease,8–11 13 and these could be accounted for by a much lower incidence of smoking. Women also had less mild or more paravalvular leaks, consistent with some studies9 11 12 24 25 but not others.10 It has been suggested that this is possibly due to the smaller aortic annulus in women leading to less frequently undersized prosthesis and more relative valve oversizing. It is reassuring, however, to note that the incidence of permanent pacemaker replacement was not increased in women.
It was interesting to note that although age and major vascular injury predicted overall 30-day mortality, only major vascular injury was significant for women and only age was significant for men. This implies that it is imperative to reduce major vascular injury in women to decrease short-term mortality.
The factors associated with 1-year mortality in this study—logistic EuroSCORE, hypertension, moderate or more paravalvular leak, 30-day NYHA class III or IV—reaffirm what is already well understood and are broadly consistent with a previous Asian registry.17
With the third-generation balloon-expandable (Sapien 3) valve and self-expanding (Evolut R and Pro) valves becoming commercially available in Asia in the recent years, the outcomes can be expected to improve. In particular, residual paravalvular leaks (both severity and frequency) for both sexes should be lowered, and the incidence of major vascular complications, especially in women, can be expected to be reduced.
Limitations
This study was limited to centres that agreed to participate, and hence data from many institutions in Asia were not available. These factors may have introduced bias into the study population. The data and outcomes were recorded by the individual centres, and no central adjudication was available. The data were analysed retrospectively and the possibility of unmeasured confounders that may have affected our results could not be excluded. There were missing parameters such as femoral/iliac vessel dimensions (CT measurements were unavailable or incomplete in many centres).
No information was available regarding the types of anaesthesia used (general anaesthesia vs local anaesthesia/conscious sedation) or the technique of femoral access (surgical cut-down versus fluoroscopy-guided percutaneous access). However, studies have shown that the incidence of major vascular injury was similar regardless of the access technique.28 29 The devices used in this study were second-generation Sapien or CoreValve prostheses; thus, these results may not apply to other devices or new-generation contemporary technologies.
Conclusions
This is the first study examining sex differences in TAVR in patients across Asia and across multiple Asian ethnicities. Women had significantly smaller physical stature and anatomy with some differences in clinical profiles. Despite a higher rate of major vascular complications, Asian women had similar 30-day stroke or death rates, functional status improvement, permanent pacemaker requirements and 1-year survival as men.
References
Footnotes
Contributors PTLC conceived the study, interpreted the data and wrote the manuscript. NQN performed the statistical analyses and reviewed the manuscript. All other authors helped to critically revise the manuscript and approved the final manuscript. PTLC takes responsibility for the overall content as a guarantor.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests PTLC, KH, YW, W-HY, MKYL, MC, WJK, KC, M-SL and HSK have served as proctors for Edwards Lifesciences. PTLC, YW, W-HY, H-LK, MKYL, WB, Dy, KC, M-SL, KWH and HSK have served as proctors for Medtronic. WJK has served as a consultant for Medtronic.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; internally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information. All data are deidentified and stored in a secure stand-alone computer.