Article Text

Abstract
Transcatheter aortic valve replacement (TAVR) has recently been approved for use in patients who are at intermediate and low surgical risk. Moreover, recent years have witnessed a renewed interest in minimally invasive aortic valve replacement (miAVR). The present meta-analysis compared the outcomes of TAVR and miAVR in the management of aortic stenosis (AS). We conducted an electronic search across six databases from 2002 (TAVR inception) to December 2019. Data from relevant studies regarding the clinical and length of hospitalisation outcomes were extracted and analysed using R software. We identified a total of 11 cohort studies, of which seven were matched/propensity matched. Our analysis demonstrated higher rates of midterm mortality (≥1 year) with TAVR (risk ratio (RR): 1.93, 95% CI: 1.16 to 3.22), but no significant differences with respect to 1 month mortality (RR: 1.00, 95% CI: 0.55 to 1.81), stroke (RR: 1.08, 95% CI: 0.40 to 2.87) and bleeding (RR: 1.45, 95% CI: 0.56 to 3.75) rates. Patients undergoing TAVR were more likely to experience paravalvular leakage (RR: 14.89, 95% CI: 6.89 to 32.16), yet less likely to suffer acute kidney injury (RR: 0.38, 95% CI: 0.21 to 0.69) compared with miAVR. The duration of hospitalisation was significantly longer in the miAVR group (mean difference: 1.92 (0.61 to 3.24)). Grading of Recommendations Assessment, Development and Evaluation assessment revealed ≤moderate quality of evidence in all outcomes. TAVR was associated with lower acute kidney injury rate and shorter length of hospitalisation, yet higher risks of midterm mortality and paravalvular leakage. Given the increasing adoption of both techniques, there is an urgent need for head-to-head randomised trials with adequate follow-up periods.
- heart valve prosthesis implantation
- aortic valve stenosis
- meta-analysis
Data availability statement
Data are available from the corresponding author upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Aortic stenosis (AS) is a progressive age-related disease with a prevalence of up to 7.2% in the elderly.1 The stenotic aortic valve increases the ventricular afterload, leading to initial compensatory left ventricular hypertrophy and eventual progression to left-sided heart failure, if not treated.2 The 5-year mortality rates are as high as 50% in medically managed patients.3 Traditionally, surgical aortic valve replacement (SAVR) was the standard of care; however, the advent of transcatheter aortic valve replacement (TAVR) has gained appreciable momentum, with a nearly ninefold increase in utilisation between 2012 and 2016.4–6 Until recently, TAVR was reserved for high-risk patients unfit for surgery; however, following the landmark PARTNER 3 and Evolut Low Risk trials,7 8 the Food and Drug Administration approved TAVR for low-risk patients as well.
In addition, recent years have witnessed a renewed interest in minimally invasive aortic valve replacement (miAVR) in selected patients.9 This approach involves either a mini-sternotomy or a right anterior mini-thoracotomy, as opposed to the full median sternotomy in traditional surgical approaches. The outcomes of miAVR in recent studies have been favourable, including decreased blood loss, shorter intensive care unit stay durations, and lower acute kidney injury (AKI) and perioperative mortality rates.10 11 Potential concerns with this approach are the increased cardiopulmonary bypass and aortic cross-clamp durations,12 which carry greater risks of adverse outcomes.13 14 The adoption of sutureless or rapid deployment valves, however, has mitigated these concerns to some extent.15
Potential advantages of miAVR over TAVR include the ability to directly observe the valve during the operation, removal of annular calcifications and lower incidence of paravalvular leakage.16 However, these may come at the cost of longer hospital stay durations and higher risk of AKI.17 Aside from these differences, recent studies that compared the two approaches were controversial with regard to the superiority of either approach for stroke,17–22 atrial fibrillation (AF),17–20 22 23 and AKI16–18 20 outcomes. To that end, we conducted the present systematic review and meta-analysis to compare the outcomes of TAVR and miAVR in the treatment of AS in the contemporary era.
Materials and methods
The protocol for this systematic review was prospectively registered on PROSPERO (CRD42020170176) and the meta-analysis was reported in compliance with the MOOSE checklist24 (online supplemental appendix 1).
Supplemental material
Literature search
We searched the following databases: MEDLINE via PubMed, Embase, Web of Science, CENTRAL, the WHO clinical trials registry (WHO ICTRP) and clinicaltrials.gov during December 2019. The main terms included in the search strategy were free-text and MeSH combinations of ‘TAVR’, ‘TAVI’, ‘Transcatheter Aortic Valve Replacement’, ‘percutaneous’, ‘Minimally Invasive Surgical Procedures’, ‘Heart valve prosthesis implantation’, ‘Aortic valve stenosis/Surgery’, ‘Replace*’, ‘Implant*’ and ‘Aortic Stenosis’. The details of our search strategy used can be found in online supplemental appendix 2. A starting date restriction was placed at 2002 (first TAVR procedure in humans).25 No restrictions by language were employed. We inspected the reference lists of the included studies to ensure that no relevant studies were missed.
Inclusion/exclusion criteria
All randomised controlled trials (RCTs) or cohort studies comparing the outcomes in patients with symptomatic AS26 who underwent either TAVR (regardless of access route) or miAVR (regardless of whether a sternotomy or a mini-thoracotomy was used, and regardless of sutureless valve use) were eligible. We excluded studies which adopted the traditional SAVR technique solely or those from which relevant data could not be extracted.
Selection and data extraction
Two reviewers (KW and SA) independently screened the titles and abstracts of all citations identified by the search strategy. Full-text articles were then obtained for studies that met our inclusion criteria, or studies which were inconclusive and required further review. The full-text articles were thoroughly examined for eligibility. Disagreements between authors regarding the inclusion of a particular study were resolved by an independent third reviewer (AS).
Data extraction was performed using a standardised spreadsheet. We collected data from eligible studies regarding the baseline characteristics, sample sizes, study designs and outcome measures. The main outcomes included all-cause mortality (both short-term and midterm ≥1 year), stroke, paravalvular leakage, AKI, AF, major bleeding and hospitalisation durations.27 The data extraction was performed by two independent reviewers (KW and SA) and the conflicts were resolved by a third reviewer (AS). When insufficient details were provided in the published articles, we attempted to contact the study authors.
Two reviewers (KW and SA) used the Newcastle-Ottawa scale (NOS) to assess the risk of bias in the included cohort studies. We planned to use the Cochrane risk of bias-2 tool to assess RCTs; however, we did not identify any RCTs that met our inclusion criteria. Conflicts were resolved by a third author (MM). The Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach was applied to assess the certainty of evidence (very low, low, moderate and high) based on the following: risk of bias as assessed by NOS, imprecision, indirectness, inconsistency and publication bias. We considered large effect sizes as a possible upgrading factor.
Data synthesis
We used the random-effects model (DerSimonian and Laird method) to obtain pooled estimates of the risk ratio (RR) or mean difference (MD) due to the anticipated high heterogeneity. We only pooled data from studies where baseline matching was performed since including studies without baseline matching would have introduced confounding by indication/selection bias. Additionally, a number of studies reported only the pooled results for their entire surgical cohort rather than for miAVR specifically. In such cases, we only included their outcome if it did not occur at all (event rate=0) in the surgical group. Heterogeneity quantification was performed using the I2. We used R meta package (V.3.5.1., R Foundation for Statistical Computing, Vienna, Austria) for statistical analyses.
Results
Characteristics of the included studies
We identified 1666 records of which 1370 remained after duplicates were removed. After initial title/abstract screening, 26 articles remained of which 14 were excluded due to ineligible interventions, lack of separate outcome reporting and studies being only available as abstracts. Finally, we included 11 studies (12 reports) in our qualitative analysis,9 16–23 28–30 7 of which were eligible for meta-analysis16–22 (figure 1). Among the included studies, there were no clinical trials, one unmatched,9 one matched,20 three where adjustment was made via a multivariate model23 28–30 and six propensity-matched16–19 21 22 cohort studies. The included studies comprised a total sample size of 4674 patients, of which 2346 underwent TAVR, while 2328 patients underwent miAVR. The average reported follow-up among the included studies was 26.7 months (range: 13–46.7 months; table 1).

Flow diagram of literature search and study selection.
Characteristics of the included studies
Patient baseline characteristics
The mean pooled age across the included studies is 82.08 years (range: 63–85.6 years), and most studies reported nearly equal numbers of males and females. There was variable reporting of baseline comorbidities in the included studies. Of the studies that reported on diabetes, none had a proportion <20%. The majority of studies reporting on hypertension had rates >75%.18 19 21–23 30 AF was reported in three studies, with an overall prevalence <20% (table 2).
Baseline characteristics of enroled patients in the included studies
Furukawa et al18 and Hirji et al30 were the only studies to report STS scores (3.4 and 5.95, respectively). Six studies used EuroScore II for risk stratification, with propensity-matched cohorts including patients with a low-to-moderate surgical risk (defined as a EuroScore II<6%). Five of the included studies reported logEuroScore with risks ranging from 38% in Zierer et al’s20 cohort to 3.77% in Tokarek et al’s study.
Risk of bias in included studies
A summary of the risk of bias assessment is illustrated in figure 2. Overall, the majority of included studies were at low risk of bias, aside from two studies in which the risk of bias was moderate due to inadequate adjustment for baseline factors9 or inadequate reporting on attrition rates.23 28 Across all outcomes, no evidence of significant publication bias was detected. GRADE assessment revealed ≤moderate quality of evidence in all outcomes. GRADE assessment results for each outcome are reported in table 3.

Risk of bias assessment results as per the Newcastle-Ottawa scale.
Summary of findings and GRADE assessment results
Selection
All included studies had a low risk of selection bias. The use of a central/hospital database to select patients and retrieve information by all studies meant that selection of the non-exposed cohort was adequate in all studies and that the studies were representative of the exposed cohort. The ascertainment of exposure among all studies was done through medical records. Finally, given that our primary outcome was mortality and acute postoperative complications, we can ensure that the outcome of interest was not present at the start of the study in all patients.
Comparability
All of the included studies, except for one,9 adjusted for comparability between the intervention groups, either by propensity-score matching or multiregression analysis.
Outcome
All studies had at least a 30-day follow-up period (which we considered sufficient based on our primary outcome of 30-day mortality). Nine out of the 11 studies either had a complete follow-up or minimal attrition rates suggesting a low risk of attrition bias.
Outcomes
All-cause mortality
One month
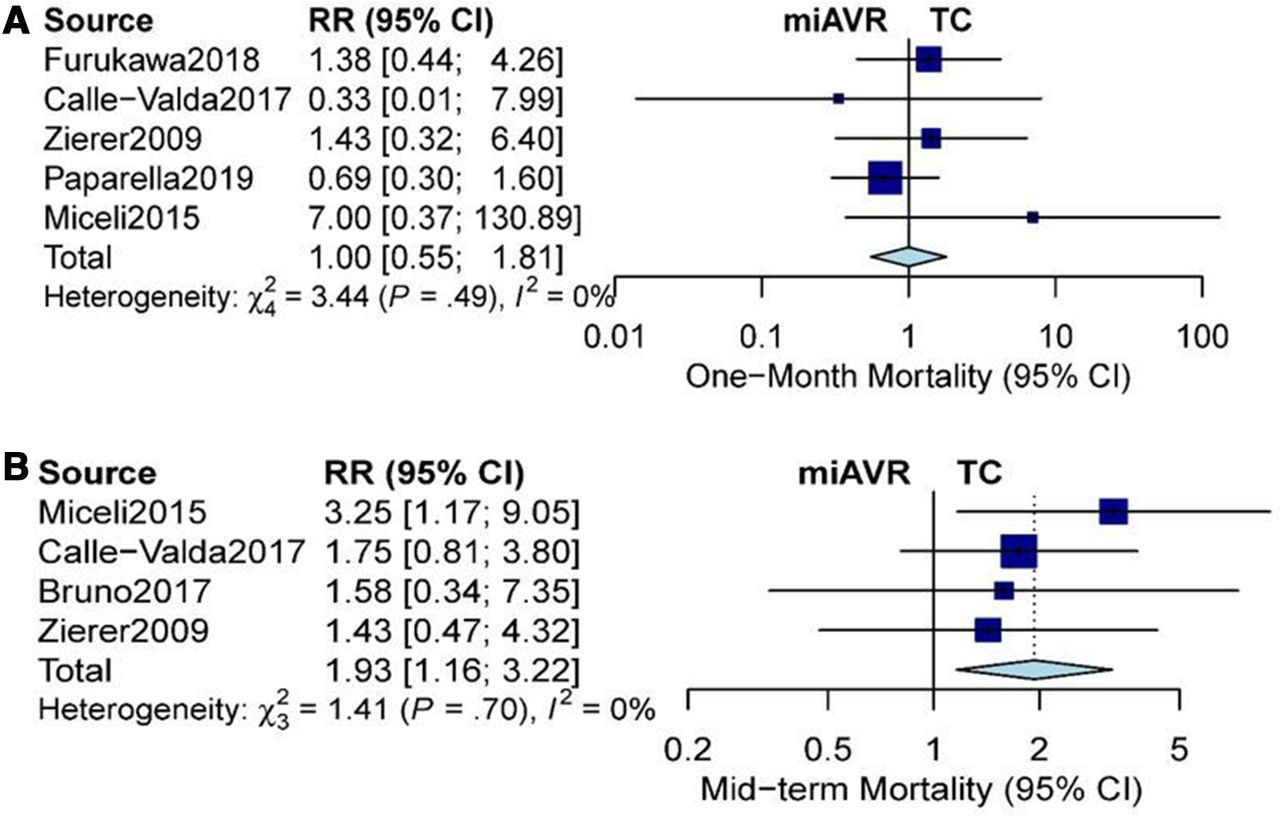
Five studies17–21 reported on 30-day all-cause mortality. We found no significant difference between TAVR and miAVR (RR: 1.00, 95% CI: 0.55 to 1.81, n=1528, I2=0%) with no evidence of heterogeneity. Even after excluding the high surgical-risk cohort by Zierer et al20 from the analysis, the pooled effect estimate showed no significant difference (RR: 1.23, 95% CI: 0.57 to 2.64, I2=23%). This difference remained non-significant after limiting the analysis to studies that adopted a transapical approach (RR: 0.57, 95% CI:0.15 to 2.15, I2=0%), studies which (partially) employed newer generation valves (RR: 0.88, 95% CI: 0.45 to 1.73, I2=0%) and recent studies, published no earlier than 2015 (RR: 0.96, 95% CI: 0.48 to 1.91, I2=6%; figure 3A).
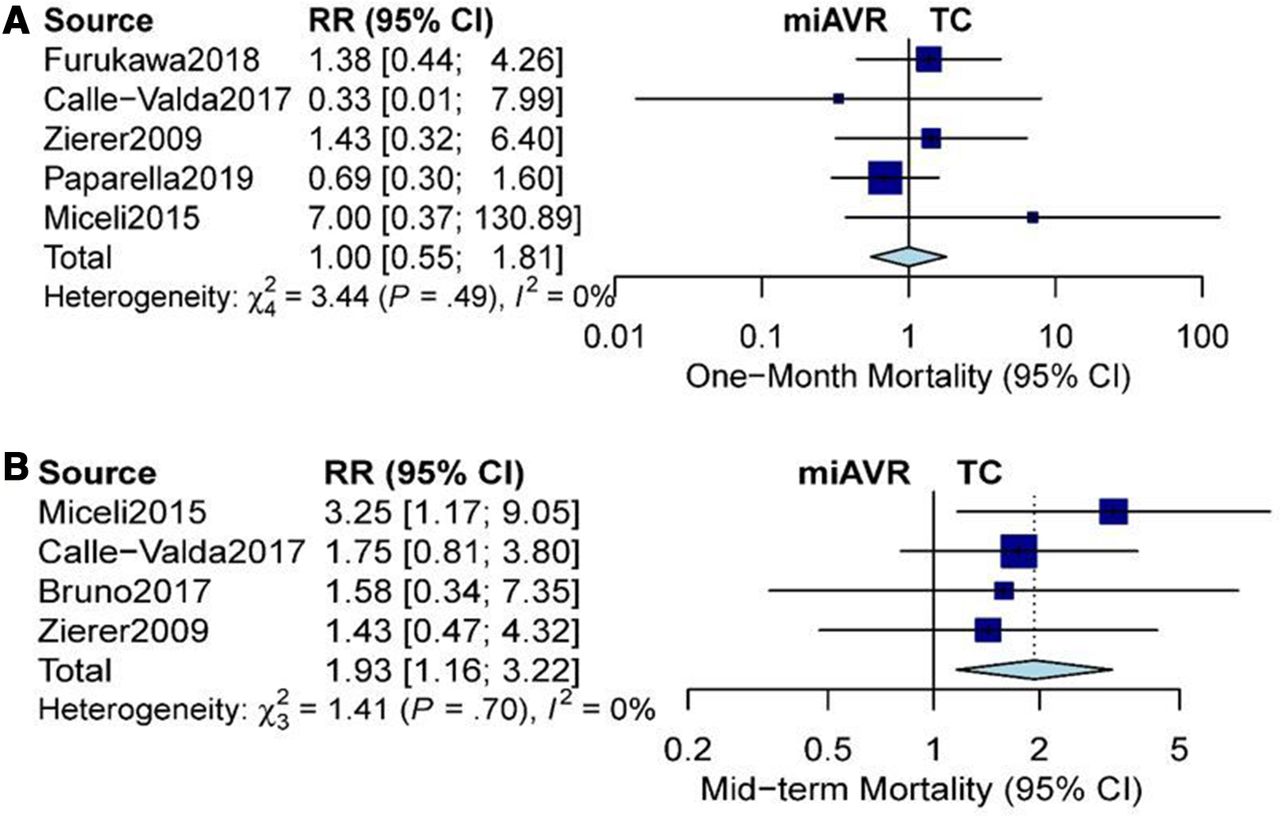
Forest plot comparing TC and miAVR (RR, 95% CI). (A) One month all-cause mortality and (B) midterm all-cause mortality. miAVR, minimally invasive aortic valve replacement; RR, risk ratio; TC, transcatheter.
Midterm mortality
Four studies19–22 contributed to the effect estimate of midterm mortality (as defined by a minimum follow-up of 1 year). Patients undergoing TAVR had a significantly higher rate of midterm mortality than those undergoing miAVR (RR: 1.93, 95% CI: 1.16 to 3.22, n=211, I2=0%). Challenging our results, we included Bruno et al’s22 results on the worst-case assumption that both patients who died in the surgical arm were in the miAVR group as separate data were not made available for the miAVR arm; figure 3B. A similar finding was obtained when analysing only recent studies (published no earlier than 2015, RR: 1.85, 95% CI: 1.05 to 3.26, I2=0%). However, subgroup analysis of the two studies that exclusively employed the transfemoral (TF) approach revealed a non-significant difference (RR: 1.71, 95% CI: 0.86 to 3.43, I2=0%), which could be due to either better results with TF approach or a significant reduction in the analysis power when excluding the other two studies.
Stroke
Six studies17–22 reported the outcome of stroke. We found no significant differences between TAVR and miAVR (RR: 1.08, 95% CI: 0.40 to 2.87, n=1588, I2=5%) with little evidence of heterogeneity; figure 4A. Similar results were obtained after limiting analysis to studies (partially) employing newer generation valves (RR: 0.67, 95% CI: 0.17 to 2.61), recent studies published no earlier than 2015 (RR: 1.18, 95% CI: 0.42 to 3.31, I2=0%) or studies that used the TF approach (RR: 1.70, 95% CI: 0.47 to 6.23, I2=0%).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Forest plot comparing transcatheter and miAVR (RR, 95% CI). (A) Stroke and (B) paravalvular leakage. miAVR, minimally invasive aortic valve replacement; RR, risk ratio; TC, transcatheter.
Paravalvular leakage
Five studies16 18–21 23 reported on paravalvular leakage. Our results show an increased incidence of paravalvular leakage with TAVR (RR: 14.89, 95% CI: 6.89 to 32.16, n=1537, I2=0%; figure 4B). This result was persistent after excluding the study by Santarpino et al16 where data were not provided separately for the miAVR group but was included in the main analysis as paravalvular leakage did not occur at all in the entire surgical cohort (RR: 15.24, 95% CI: 6.85 to 33.92, I2=0%). Similar results were obtained after limiting analysis to studies published no earlier than 2015 (RR: 15.79, 95% CI: 6.87 to 36.27, I2=0%) or employing newer generation valves (RR: 16.18, 95% CI: 5.21 to 50.22).
Acute kidney injury
Four studies16–18 20 reported on AKI. We showed a significantly lower incidence of AKI with TAVR compared with miAVR (RR 0.38, 95% CI: 0.21 to 0.69, n=1428, I2=35%), with moderate evidence of heterogeneity. On excluding Santarpino et al’s16 results where miAVR outcomes were not reported separately, the heterogeneity was resolved (RR: 0.34, 95% CI: 0.23 to 0.51, I2=0%) with more of an advantage for TAVR.
Atrial fibrillation
Six studies17–20 22 23 reported on AF outcome. Initially, our results showed no significant differences between the two groups in terms of the incidence of postoperative AF (RR: 0.37, 95% CI: 0.10 to 1.32, n=1514, I2=89%). However, the significant heterogeneity prompted us to probe further; we found that when considering only TF–TAVR procedures where some of the patients received newer generation valves, the reduction in postoperative AF became statistically significant in favour of TAVR, though heterogeneity was still high (RR: 0.14, 95% CI: 0.04 to 0.48, I2=88%).
Major bleeding
Four studies reported on major postoperative bleeding,18 20–23 with no significant difference between the two approaches (RR: 1.24, 95% CI: 0.46 to 3.35, n=716, I2=0%).
Hospitalisation duration
Six studies17–22 reported on hospitalisation duration, with miAVR showing significantly longer durations as compared with TAVR (MD: 1.92, 95% CI: 0.61 to 3.24, n=1588, I2=95%), though high heterogeneity was observed. On excluding the TA cohorts of Zierer et al20 and Bruno et al,22 both of which had extreme values (the former in favour of TAVR and the latter in favour of miAVR), heterogeneity was resolved (MD: 2.00, 95% CI: 1.61 to 2.40, I2=0%).
Discussion
Despite the promising short-term results of the PARTNER trials,7 31 long-term outcomes after TAVR remain an ongoing concern. For instance, 2 to 5 year follow-up analysis of the PARTNER 2 trial31 demonstrated a higher incidence of all-cause mortality in the TAVR cohort. Many have postulated that the underlying reasons may include the increased likelihood of structural valve degeneration and paravalvular leakage associated with TAVR. Consistent with this hypothesis, the TAVR cohort in the PARTNER 2 trial had a greater need for repeat intervention and valve-in-valve TAVR. Unfortunately, the PARTNER trials did not separately compare TAVR with miAVR (as the surgical arm was inclusive of all approaches); therefore, leaving an important gap in the literature.
In our pooled analysis, the 30-day all-cause mortality did not differ significantly between both groups; however, midterm mortality was significantly higher in the TAVR cohort. It should be noted that none of the included studies independently demonstrated a survival difference, likely due to the lack of statistical power, a common issue with propensity-matched studies (owing to the smaller sample size produced by the matching process). We could not include the study by Tokarek et al,23 which found no significant differences between the two approaches because rather than matching patients at baseline, the authors only adjusted for confounders by inserting the propensity score as a variable in their logistic regression model. Their results contrasted with ours in that they trended towards (but were not significant for) higher survival rates with TAVI; however, the small sample size and consequently wide confidence intervals limit our ability to draw solid conclusions. The study by Hirji et al30 investigated the same question in octogenarians and after adjustment for a number of important variates in a Cox model, none of the approaches (TF/TA–TAVI, miAVR or conventional surgery) seemed to be statistically significant determinants of survival. Further studies, especially RCTs, are warranted to better delineate the outcome differences between the two procedures.
Our finding that TAVR is associated with a greater degree of paravalvular leakage is consistent with previous studies.7 31 The PARTNER 2A trial suggested that moderate-to-severe regurgitation may be associated with higher mortality on extended follow-up, which may explain our previous finding. The lower risk of paravalvular leakage with miAVR may be due to a number of factors, including the ability to resect the previously calcified native valve,32 and the relatively lower degree of mechanical stress on valve leaflets.33
In addition, our analysis demonstrated a lower risk of AF with TF–TAVR when newer generation valves were utilised. This finding is in agreement with previous studies which have reported a lower risk of AF with TAVR procedures, and others which suggest that the TF approach and newer generation valves are associated with a lower risk of AF.34–38 This is particularly important as AF has been shown to be associated with a higher incidence of mortality, stroke, bleeding and pacemaker placement post-TAVR.39–43
Our analysis also demonstrated that TAVR was associated with a lower risk of AKI compared with miAVR. This contrasts with a previous study by Haldenwang et al,29 which showed a higher incidence of AKI with TAVR; however, in Haldenwang et al’s study, the TAVR arm only employed the TA approach, which was shown to be associated with higher rates of AKI than TF approach.44 A possible explanation may be the non-pulsatile blood flow provided by cardiopulmonary bypass and aortic cross-clamping, which may either increase ischaemic times or increase the risk for embolic events to the kidney, causing reversible ischaemic renal damage.
As previously reported in the literature, TAVR was associated with shorter hospitalisation durations. This finding is understandable if we consider the relatively greater degree of surgical trauma and invasiveness inherent to miAVR. The heterogeneity in our result was explained by the utilisation of TA–TAVR in one study20 and an increased incidence of pacemaker implantation in the TAVR cohort in the other.22 The only study to report on quality of life was an unmatched cohort that showed better quality of life with TAVI on the short term (1 month and 1 year), but no differences on the long term (2 years).28
Our study has some limitations. First, we could not conduct separate subgroup long-term mortality analysis for the TF cohort or different surgical risk strata given the lack of sufficiently detailed data within the included studies. Second, many of the studies used older-generation valves, which may have hampered or confounded TAVR’s longer-term effectiveness over miAVR. Further, some eligible studies did not provide data on important outcomes such as long-term mortality and AKI; therefore future studies should employ longer follow-up periods in addition to a more comprehensive reporting of outcomes. Finally, though we only included propensity-matched studies in our analyses, we were still unable to completely rule-out the possible confounding by variables not accounted for in the matching process. An individual patient data meta-analysis approach could be valuable in this regard.
The recent results of the PARTNER 2A and 37 31 trials seem to have placed TAVR in the driving seat for most AVR procedures. Nevertheless, long-term valvular dysfunction and consequent mortality remain valid concerns. Likewise, miAVR has also seen a considerable increase in uptake over the past few years along with the general preference for less invasive approaches dominating the realm of AVR in selected patients. The use of miAVR may retain the superior haemodynamic outcomes usually associated with surgery, while minimising the downsides of the highly invasive SAVR; all while providing better long-term survival outcomes than TAVR. Yet, the higher risks of AKI and prolonged hospitalisation deserve attention. Nevertheless, these findings need to be confirmed in future RCTs, as the current state of the literature does not allow a definitive statement in this regard. In addition, our findings suggest an urgent need to develop comprehensive evidence-based criteria to determine which patients, especially the younger population, may benefit most from either of the two procedures.
Conclusion
According to our meta-analysis of matched cohort studies, miAVR may be associated with a lower risk of midterm mortality, while TAVR was associated with shorter hospitalisation durations and a lower risk of AKI. Given the increasing adoption of both techniques, there is an urgent need for head-to-head randomised trials with adequate follow-up periods.
Data availability statement
Data are available from the corresponding author upon reasonable request.
Ethics statements
Patient consent for publication
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @drabendary, @Shoukmed
Correction notice This article has been corrected since it first published. The provenance and peer review statement has been included.
Contributors Literature search, screening and data extraction were performed by AS, SA, KW and MM. Data analysis was done by AS and AIA. Manuscript drafting was performed by AS, SA, KW, MM and AIA. Analysis and writing revision were done by AR, SH and AIA.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.