Article Text

Abstract
Objective Functional tricuspid regurgitation (TR) is a frequent finding in echocardiography. Literature suggests significant TR is associated with poor prognosis. Still, data remain limited. This study aimed to evaluate long-term prognostic implications in patients with TR.
Methods In this observational cohort study, data from 1650 consecutive patients were analysed. Primary endpoint was all-cause mortality. Mean follow-up time was 1090 days. TR grades at baseline and follow-up were compared. Survival analyses were performed to identify prognostic factors.
Results At baseline, 14.1% patients showed no, 63.8% mild, 17.4% moderate and 4.7% severe TR. 359 patients (21.8%) died within the study period. TR at baseline was associated with excess mortality. Moderate and severe TR were of prognostic implication in all subgroups irrespective of systolic pulmonary artery pressure (sPAP) (</≥40 mm Hg) and left ventricular ejection fraction (LV-EF) (</≥50%). Survival was worst in patients with moderate and severe TR and concomitant elevated sPAP or reduced LV-EF at 1 and 3 years, respectively (p<0.001; p<0.001). In a multivariate model, including cardiac and non-cardiac risk factors, moderate and severe TR, sPAP and impaired right ventricular (RV) function were independent predictors for survival (HR 1.89, CI 1.07 to 3.36, p=0.029; HR 2.93, CI 1.57 to 5.49, p=0.001; HR 1.44, CI 1.25 to 1.65, p<0.001; HR 1.43, CI 1.14 to 1.79, p=0.002). Overall progression of TR on follow-up was 28.4%. Patients with TR progression showed significantly worse survival (HR 1.44, CI 1.11 to 1.81; p=0.006).
Conclusion While TR progressed over time, it was associated with impaired long-term survival. TR grade, RV dysfunction, sPAP and TR progression were independent predictors for survival.
- tricuspid valve insufficiency
- pulmonary arterial hypertension
- echocardiography
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known about this subject?
Literature suggests significant tricuspid regurgitation (TR) is associated with poor prognosis. Still, data remain limited. Particularly quantitative assessment of TR and right ventricular (RV) parameters are lacking in large trials investigating survival.
What does this study add?
This is the first study to assess TR and its natural course according to quantitative echocardiographic measures, including measurement of TR and the right ventricle in particular. We identified TR grade, RV dysfunction, pulmonary pressure and TR progression as independent predictors for survival besides known risk factors such as left ventricular ejection fraction, NT-proBNP, aortic stenosis, type 2 diabetes and atrial fibrillation. Our findings imply that moderate-to-severe TR robustly associates with mortality and confirm that TR is of prognostic value.
How might this impact on clinical practice?
As TR is a potentially treatable pathology and progression might be preventable, a more aggressive management may improve patient outcomes, which is of interest since tricuspid valve interventions are on the rise.
Accurate and standardised echocardiographic assessment of the tricuspid valve and the right ventricle is of prognostic relevance.
Introduction
Functional tricuspid regurgitation (TR) is a frequent finding in echocardiography. It is mostly secondary due to left-sided heart disease and occurs predominantly in patients with mitral and aortic valve pathologies.1 2 Besides that, there is evidence that atrial fibrillation (Afib) and right ventricular (RV) pacing may also be of pathophysiological importance.3–5 While significant reflux may be well tolerated for years TR is often neglected. However, literature suggests significant TR is associated with poor prognosis.6 7 Still, data remain limited. Particularly quantitative assessment of TR and RV parameters are lacking in large trials investigating survival.
Quantitative assessment of TR, especially proximal isovelocity surface area (PISA) and effective regurgitant orifice area (EROA) measurement, has recently been shown to be a more powerful and independent predictor for evaluation of TR compared with qualitative assessment by jet area and should be therefore included in the standard assessment.2 The prognostic value of PISA in the evaluation of clinical outcome in TR patients remains unclear.
Furthermore, it is unknown whether TR itself or rather TR in combination with other comorbidities such as RV dysfunction, pulmonary hypertension (PH), left heart failure or arrhythmias account for an increase in mortality.2 6
Current guidelines for treatment of patients with TR are cautious due to contradictory study results.2 8 At present, only diuretics represent a conservative therapeutic option for volume relief. Surgical treatment has not shown promising results and is primarily recommended in patients undergoing open-heart surgery for mitral and aortic valve disease.8 9 Transcatheter solutions may be a promising approach in the future, still devices are in development and outcome on symptom relief and survival largely unclear10
Also, the natural course of TR is not very well known. It has been shown to progress over time. TR development appears to be associated with an increase in pulmonary artery pressures, Afib and coronary artery disease.11 Prognostic implications remain largely unclear.
This study aimed to assess TR and its natural course according to quantitative echocardiographic measures in clinical practice and long-term prognostic implications including possible risk factors for adverse outcomes such as RV dysfunction, PH and left heart failure.
Methods
Patient population
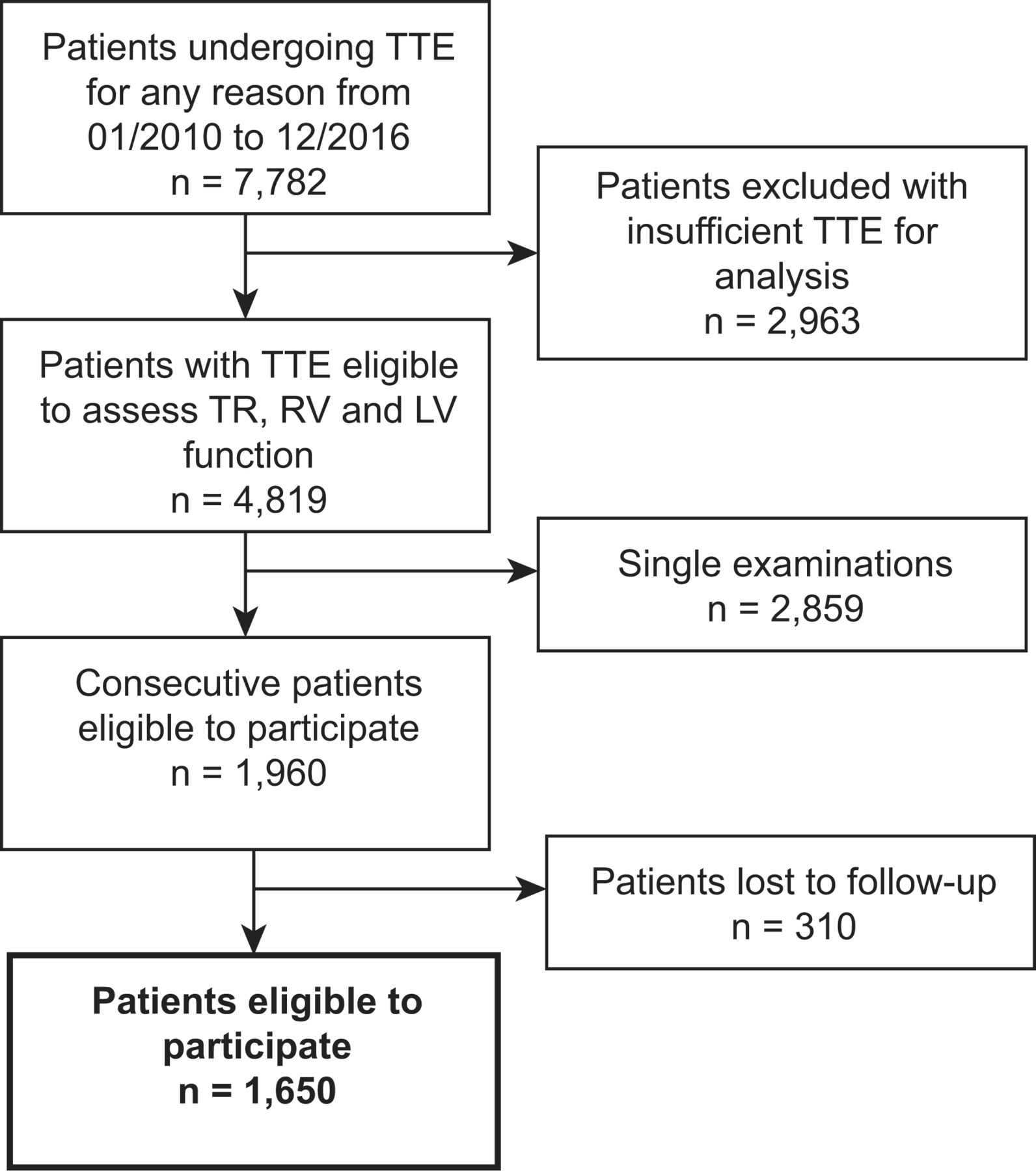
In this retrospective observational cohort study, data from 1650 consecutive patients (42.8% female) undergoing echocardiography at two time points at a tertiary care centre in Brandenburg, Germany, from January 2010 to December 2016 were analysed. Follow-up was conducted from June 2018 to June 2019. The patient flow is shown in figure 1.

Patient flow through the study. Figure shows patients included and excluded in the study with a number of n individuals at each step. LV, left ventricular; RV, right ventricular; TR, tricuspid regurgitation; TTE, transthoracic echocardiography.
Data collection and outcome definition
Demographics and clinical data including relevant comorbidities and laboratory results were collected using patient medical records. Follow-up data for survival rates were collected from the hospital database and primary care physicians. Patients were followed for all-cause mortality.
Echocardiographic examinations were performed with commercially available ultrasound systems (GE-Vingmed, Vivid 7 and E9, Horten Norway) by trained physicians. Complete echocardiograms included 2-dimensional, pulsed-wave, continuous-wave and colour Doppler imaging. The original datasets were prospectively reanalysed. Investigators were blinded for all endpoints to avoid bias. Standard echocardiographic measurements for the evaluation of left atrial size and left ventricular (LV) geometry and function were performed according to the guidelines of the American Society of Echocardiography.12 TR determination was conducted in line with current recommendations and guidelines using the following criteria: dilated annulus with no valve coaptation or flail leaflet, large central jet >50% of right atrial, vena contracta (VC) width >7 mm, PISA radius >9 mm at Nyquist 30–40 cm/s, dense triangular continuous wave jet or sine wave pattern and dilated RV. PISA/EROA measurement was employed including angle correction. PISA and VC were obtained from an apical four chamber zoom view. TR was graded in four stages: none (0), mild (1), moderate, (2) and severe (3).13 14 On a 2D RV focused four chamber view RV size and RV function were analysed. Tricuspid annular plane systolic excursion (TAPSE) was calculated on M-mode recordings. RV function was measured using TAPSE, RV fractional area change (FAC) and tricuspid annular systolic velocity as described previously.15 RV dilation was assessed by RV diameters (basal, mid and longitudinal) and RV end-diastolic area in four chamber view.12 16
The same views were used for baseline and follow-up examinations. EchoPAC V.202 (GE-Vingmed, Horten, Norway) was used for all echocardiographic analyses.
PH was determined by echocardiographic measurement of TR Vmax and graded into unlikely, possible and likely according to the guidelines of the European Society of Cardiology.17 18
Chronic kidney disease (CKD) was defined according to kidney damage with glomerular filtration rate (GFR) <60 mL/min/1.73 m2 using CKD-EPI creatinine equation for estimation, irrespective of cause.19 20
Age-adjusted N-terminal probrain natriuretic peptide (NT-proBNP) cut-offs were determined in accordance with the recommendations of the Heart Failure Association of the European Society of Cardiology.21
The primary endpoint was defined as all-cause mortality; the secondary endpoint was progression of TR at follow-up.
The Strengthening the Reporting of Observational Studies in Epidemiology recommendations for reporting observational studies were applied.22
The public was involved in the design of this research. Outcome measures and methods of recruitment were discussed in a focus group session.
Statistics
Data were analysed using descriptive statistics, with categorical variables presented as absolute values and frequencies (%) and continuous variables presented as means with SD. Comparisons between the four TR grade groups were carried out using an analysis of variance for continuous variables, Fisher’s exact or χ2 test for categorical variables.
For the analysis of differences regarding TR grades at baseline and follow-up, TR grade comparisons between these groups were carried out using Wilcoxon test. Survival analysis data are presented as Kaplan-Meier curves. Cox-regression analysis with backwards elimination (using a p value>0.100 as removal criterion) for all-cause mortality including cardiac and non-cardiac risk factors was performed. Risk factors included in the analysis were: TR grade, systolic pulmonary artery pressure (sPAP), RV function, TR progression, CKD stage, LV-EF, Afib, age, sex, body mass index (BMI), aortic stenosis, mitral regurgitation, coronary artery disease, hypertension, dyslipidaemia, type 2 diabetes and implantable cardiac device (pacemaker or defibrillator). Results are presented as HRs with CIs.
A p value of ≤0.05 was considered statistically significant.
All statistical tests were performed using IBM SPSS Statistics software V.24.0 or V.26.0 (IBM Corporation).
Results
Baseline characteristics
Of all 1650 consecutive patients (42.8% male), 232 (14.1 %) patients showed no, 1053 (63.8 %) mild, 287 (17.4 %) moderate and 78 (4.7 %) severe functional TR at baseline. On average, patients were obese (BMI 27.9±5.1 kg/m2) and showed a relevant number of cardiovascular risk factors, cardiac and general comorbidities (table 1).
Patients characteristics
Higher TR grades were found when patients were at an advanced age (TR 0 70.6±12.8 years vs TR 1 73.0±10.8 years, TR 2 75.7±9.3 years and TR 3 74.5±9.9 years; p<0.001) or of female sex (TR 0 37.5% vs TR 1 40.9 %, TR 2 50.7% and TR 3 55.1%; p=0.001). Patients with moderate and severe TR showed a trend towards a lower BMI (TR 0 29.8±5.5 kg/m2 vs TR 1 27.9±4.9 kg/m2, TR 2 26.7±5.1 kg/m2 and TR 3 26.9±5.0; p<0.001).
PH according to echocardiographic criteria was more likely in patients with TR compared with those with none (TR 0 4.7% vs TR 1 18.8 %, TR 2 48.4 and TR 3 29.5%; p<0.001). With increasing TR severity, there was an incline in the incidence of Afib (TR 0 25.9% vs TR 1 44.7 %, TR 2 70.3% and TR 3 80.5%; p<0.001). Aortic stenosis, mitral regurgitation and dyslipidaemia were less often detected in patients with TR, while prior implantation of a cardiac device (pacemaker or defibrillator), prior mitral valve surgery and CKD were more likely (table 1).
Patients with TR showed significantly higher NT-proBNP levels (no TR 1264±1783 pg/mL vs mild TR 3461±4695 pg/mL, moderate TR 5264±5025 pg/mL and severe TR 6029±6689 pg/mL; p<0.001) and worse CKD-EPI GFR (no TR 71.0±29.3 mL/min vs mild TR 65.6±26.4 mL/min, moderate TR 56.4±27.0 mL/min and severe TR 55.5±21.3 mL/min; p<0.001) compared with those with no TR (table 1).
TR PISA, EROA and VC were significantly higher in patients with TR compared with no TR as baseline (all p<0.001). Tricuspid valve (TV) annular diameters (p<0.001) and RV size increased with TR grade (RV basal p<0.001, RV mid p<0.001, RV longitudinal p=0.009, RV end-diastolic area p<0.001). Patients with moderate or severe TR showed significantly reduced RV function compared no TR (TAPSE p<0.001, RV FAC p<0.001, TASV p<0.001). TR was also associated with impaired LV function (p<0.001).
Echocardiographic characteristics overall and divided by TR grade are shown in table 2.
Echocardiographic parameters at baseline echocardiography
Long-term survival
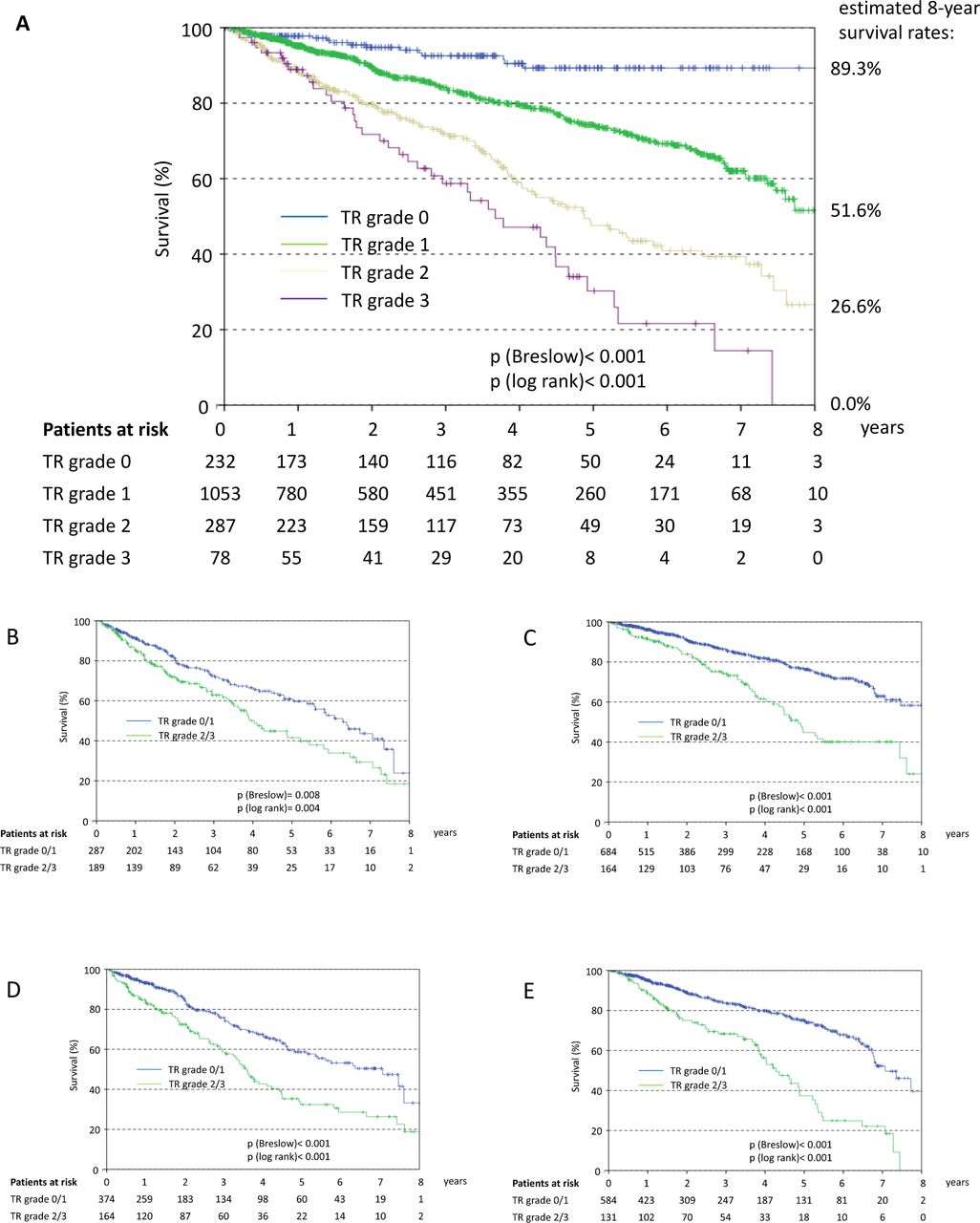
A total of 359 patients (21.8 %) died within the study period. Mean follow-up time was 1090 days. TR on baseline echocardiography was associated with excess mortality in Kaplan-Meier analysis (log rank, p<0.001) (figure 2A). Moderate and severe TR were of prognostic implication in all subgroups irrespective of sPAP (</≥40 mm Hg) and LV-EF (</≥50 %) (figure 2B–E). Survival was worst in patients with moderate and severe TR and concomitant elevated sPAP or reduced LV-EF (p<0.001; p<0.001) (figure 2B–E).

Kaplan-Meier survival curve for (A) all patients divided by TR grade and patients separated by TR grade 0/1 versus 2/3 and (B) sPAP ≥40 mmHg, (C) sPAP <40 mm Hg, (D) LV-EF <50 %, and (E) LV-EF ≥50%. Patients with TR show significantly worse survival. Moderate and severe TR had prognostic value irrespective of sPAP (</≥40 mm Hg) and LV-EF (</≥50 %). However, survival was lowest in patients with concomitant elevated sPAP and reduced LV-EF.
In a multivariate model, including cardiac and non-cardiac risk factors, moderate and severe TR, sPAP (≥40 mm Hg) and impaired RV function (TAPSE ≥18.5 mm) were independent risk factors for survival (HR 1.89, CI 1.07 to 3.36, p=0.029; HR 2.93, CI 1.57 to 5.49, p=0.001; HR 1.44, CI 1.25 to 1.65, p<0.001; HR 1.43, CI 1.14 to 1.79, p=0.002) besides CKD, impaired LV-EF, NT-proBNP, aortic stenosis, type 2 diabetes and Afib (table 3).
Cox-regression for all cause mortality
Progression of TR
Compared with baseline echocardiographic assessment, there was significant overall progression of TR on follow-up in 28.4% of patients within the study period (at least one grade on echocardiography). TR progressed stronger over time but was only detectable after at least 1 year of follow-up (≤1 year p=0.310; >1 year – 3 years p=0.033, >3–6 years p<0.001 and >6–9 years p<0.001; figure 3).

TR progression over time divided by follow-up (FU) time intervals: Total, ≤1 year, >1 to ≤3 years, >3 to ≤6 years, and >6 to<9 years. Compared with baseline echocardiographic assessment, there was significant overall progression of TR on follow-up. TR progressed stronger over time but was only detectable after more than 1 year of FU.
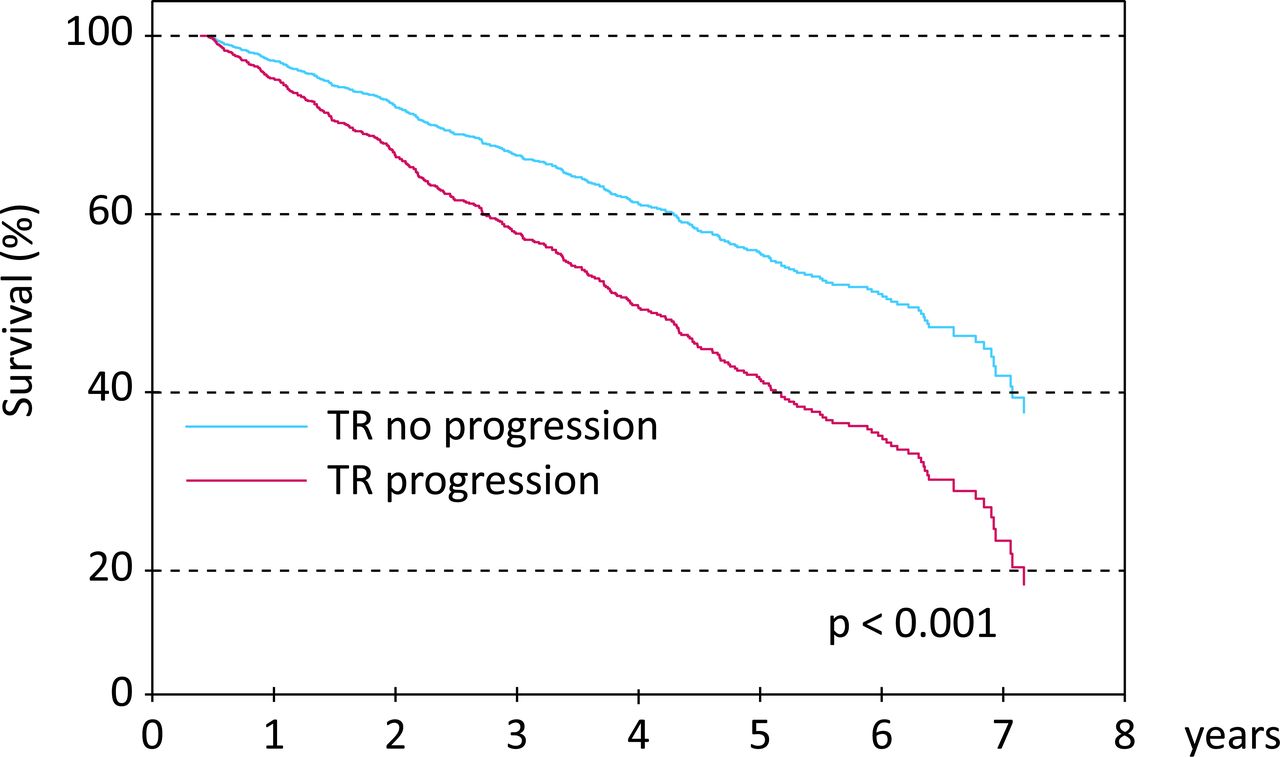
Patients with TR progression showed significantly worse survival (HR 1.44, CI 1.11 to 1.81; p=0.006; table 3 and figure 4).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Kaplan-Meier survival curve for patients divided by TR progression (at least one grade) on follow-up echocardiography. Patients with TR progression showed significantly worse survival (HR 1.44, CI 1.11 to 1.81; p=0.006).
Discussion
In this study, we assessed TR and its natural course according to quantitative echocardiographic measures in clinical practice and evaluated the long-term prognostic implications including possible risk factors.
Within our patient population, almost 25% of patients exhibited moderate or severe TR. Moderate and severe TR had prognostic value irrespective of sPAP and LV-EF. However, survival was lowest in patients with concomitant elevated sPAP and reduced LV-EF. On follow-up, there was significant progression of TR in approximately 30% of patients.
Besides TR grade, RV dysfunction, sPAP, TR progression, LV-EF, NT-proBNP, CKD, aortic stenosis, type 2 diabetes and Afib were independent predictors for survival.
Patients with significant TR were more likely at an advanced age and female. They exhibited Afib, PH and CKD more often and were more prone to have a history of prior mitral valve surgery or implantation of a cardiac device.
Clinical implications
TR is a common finding in echocardiography and considered benign at first.1 2 Initially, symptoms are nonspecific and progress slowly. Patients at later stages, who present with relevant TR and heart failure, often already show signs of irreversible RV dysfunction.
In our study, moderate-to-severe TR was associated with increased mortality throughout all patient subgroups, including normal and impaired LV-EF as well as normal and increased pulmonary pressure. However, survival was worst in those patients with reduced LV-EF and elevated pulmonary pressure.
This is the first study to assess TR and its natural course according to quantitative measurement of TR and RV in particular, showing that TR is of prognostic value irrespective of sPAP and LV-EF in a large patient cohort. It confirms the results of Nath et al and Benfari et al, that moderate and severe TR are associated with a poor prognosis.6 7 However, Nath et al only qualitatively graded TR by jet area, which is less robust. Quantitative assessment may have been helpful, as the authors state. Also, RV enlargement was considered primarily in comparison to LV size without definite measurements. RV function was mainly evaluated by TAPSE only. Most of patients were men and clinical characteristics were unknown.7 The other study by Benfari et al only addressed patients with heart failure and impaired LV function, that is, mean LV-EF 36 %, which only represents a limited subgroup of patients at risk.6
Moderate-to-severe TR is associated with annular dilation. Pathophysiologically, functional TR cannot be considered a mere valvular disease. It should rather be regarded in the context of RV dysfunction. Increased RV afterload, that is, elevated pulmonary pressure by either LV dysfunction or left-sided valvular disease, cause RV and tricuspid annular dilation and thus TR.23 Patients with relevant TR showed significantly dilated RV and impaired RV function in this cohort. Hemodynamically, a ‘vicious circle’ of RV dilatation, RV dysfunction and TR evolves over the course of time. Previous studies have shown an association between RV dilation and increased mortality.24 At the same time, TR is commonly associated with RV enlargement. However, the reason for excess mortality in patients with TR remains to be determined.
Interestingly, almost half of patients with severe PH showed only mild TR.25 These findings underline difficulties in echocardiographic assessment of right heart function including TR and PH. In this context, new imaging techniques represent a spectrum of high interest. In the future, the use of new echocardiographic methods such as RV strain using speckle tracking may allow a much more precise assessment of the RV.
Mild TR in structurally heart-healthy individuals is considered a physiological and not a pathological finding. In this study, we were able to identify a significant overall progression of TR on follow-up. Based on our results, a time interval of at least 1 year is necessary to detect a significant change on echocardiography. This seems to be important for planning routine follow-ups, as relevant progression is likely over time. Furthermore, patients, who suffer from fast development of TR, have been shown to have worse survival than those with slower development.11 In this context, large prospective studies, ideally with knowledge of the invasive pressure gradients, would be necessary to find a sustainable therapeutic approach to break the cycle of RV dysfunction and TR.
Increased NT-proBNP were associated with excess mortality in this study. However, unspecific regarding the cause of heart failure, the marker may add additional information with prognostic implications in patients with TR.
Interestingly, there were several significant differences between patient groups with regard to TR grade, that is, gender, BMI and prior implantation of cardiac devices, which did not appear to be independent risk factors for mortality.
Women showed a trend towards higher TR grades in this cohort with regard to baseline characteristics, even though gender was insignificant in the multivariate survival model. According to current literature, the incidence of heart failure is generally lower in women than in men at all ages. Due to an increase in incidence of heart failure with age and a proportionally larger number of elderly women, the total number of men and women living with heart failure has been overall reported as similar.26
Patients with RV dysfunction may furthermore show signs of cardiac cachexia. This has been associated with adverse effects in the past and reported as a relevant risk factor in patients undergoing valvular surgery indicating end-staged disease.27 28 A decreasing BMI with TR progression in our study population might indicate a pathological shift of metabolism towards a rather catabolic state. Despite this negative trend, it is noteworthy that even in patients with severe TR mean BMI was >25 kg/m2.
There has been growing evidence of interplay regarding Afib, TV annular and right atrial dilation and remodelling with consequent functional TR.4 On the one hand, restoration of sinus rhythm has been associated with reverse remodelling of the right atrium and improvement of TR severity.3 Still, data are limited. On the other hand, atrial enlargement caused by atrioventricular valve reflux is a well-known risk factor for Afib itself.29
Chronic RV pacing may further deteriorate RV (and LV) function causing pacing-induced cardiomyopathy and therefore worsen TR.30 RV lead interference can mechanically cause TR while there is also evidence for increase in TR grade by RV pacing, irrespective of altered RV function and direct mechanical disruption.5 Patients with advanced TR had up to three times more often a history of prior pacemaker or defibrillator implantation, which appears logical because they suffer from progressive heart failure.
Our findings imply that moderate-to-severe TR robustly associates with mortality. We believe that in the future accurate and standardised assessment of the TV and RV is of importance to identify patients at risk. Still further prospective data including possible interventions of the TV are needed in order to establish an ideal treatment of patients with TR. Since TR is a potentially treatable pathology and progression may be preventable, a more aggressive management might improve patient outcomes in the future. At the moment, TR is mainly managed medically by administering diuretics for symptomatic relief.31 Surgical isolated TV repair has not been shown to be promising. Indication for TV surgery is limited mainly to patients who simultaneously undergo mitral or aortic valve repair. Referral for surgery in patients with isolated TR may be beneficial at an early stage.32 Data imply the importance to intervene while the right ventricle has not been irreversibly damaged.33 Transcatheter solutions may be a promising approach in the future since they are less invasive. However, all interventional devices are still in development.10
Study limitations
The study was retrospectively performed at a single centre. Lead time bias may be a confounder. Patients underwent echocardiography for a variety of indications. Early detection of TR in the disease course may artificially inflate perceived survival duration.
While tricuspid, aortic and mitral valve pathologies, RV and LV function were analysed in all patients at baseline and follow-up, some parameters, such as PH or GFR, could not be reanalysed in all patients but still the vast majority. Only patients with echocardiographic examinations at baseline and follow-up were included.
TR is known to fluctuate and to be load dependent. Standards for evaluation of TR are less robust than for mitral or aortic valve disease. The jet area can have an overlap in patients with mild versus moderate TR. It can be considered semiquantitative, as the flow in wide-open TR may be so low that aliasing does not occur as a distinct jet. Since imaging of the inferior vena cava and hepatic vein flow were not part of the standard echocardiography protocol, they could not be assessed in this cohort.
There were no data available for administered medications, especially diuretics.
Conclusion
While TR progressed over time, it was associated with impaired long-term survival in all subgroups. TR grade, RV dysfunction, sPAP and TR progression were independent predictors for survival besides LV-EF, NT-proBNP, aortic stenosis, type II diabetes and Afib.
References
Footnotes
Contributors MB coordinated the study, acquisited and analysed data, prepared figures and wrote the manuscript. CRE interpreted data, contributed to manuscript preparation and final submission. UK, JL and MO acquisited and analysed data. VH, VD, FS and TK interpreted data and contributed to manuscript preparation. KB and PB analysed data and revised the article critically for the content. AH-F and CB planned the study. All authors provided final approval of the article.
Funding This research received funding from Deutsche Stiftung für Herzforschung, Bockenheimer Landstr. 94-96, 60323 Frankfurt am Main.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The study was approved by the local Ethics Committee of the State Brandenburg (AS 155(bB)/2017) and was conducted in accordance with the Declaration of Helsinki.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Original data are available upon reasonable request.