Article Text

Abstract
Objective To assess associations of health-related quality of life (HRQoL) with patient profile, resource use, cardiovascular (CV) events and mortality in stable patients post-myocardial infarction (MI).
Methods The global, prospective, observational TIGRIS Study enrolled 9126 patients 1–3 years post-MI. HRQoL was assessed at enrolment and 6-month intervals using the patient-reported EuroQol-5 dimension (EQ-5D) questionnaire, with scores anchored at 0 (worst possible) and 1 (perfect health). Resource use, CV events and mortality were recorded during 2-years’ follow-up. Regression models estimated the associations of index score at enrolment with patient characteristics, resource use, CV events and mortality over 2-years’ follow-up.
Results Among 8978 patients who completed the EQ-5D questionnaire, 52% reported ‘some’ or ‘severe’ problems on one or more health dimensions. Factors associated with a lower index score were: female sex, older age, obesity, smoking, higher heart rate, less formal education, presence of comorbidity (eg, angina, stroke), emergency room visit in the previous 6 months and non-ST-elevation MI as the index event. Compared with an index score of 1 at enrolment, a lower index score was associated with higher risk of all-cause death, with an adjusted rate ratio of 3.09 (95% CI 2.20 to 4.31), and of a CV event, with a rate ratio of 2.31 (95% CI 1.76 to 3.03). Patients with lower index score at enrolment had almost two times as many hospitalisations over 2-years’ follow-up.
Conclusions Clinicians managing patients post-acute coronary syndrome should recognise that a poorer HRQoL is clearly linked to risk of hospitalisations, major CV events and death.
Trial registration number ClinicalTrials.gov Registry (NCT01866904) (https://clinicaltrials.gov).
- coronary artery disease
- myocardial infarction
- quality of healthcare
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known about this subject?
Patients’ self-reported health-related quality of life (HRQoL) can be assessed using the EuroQol-5 dimension (EQ-5D) for patients with stable coronary artery disease following myocardial infarction (MI).
What does this study add?
This study finds that a lower EQ-5D index score was associated with clinical and demographic factors assessed 1–3 years post-MI, and with subsequent hospitalisations, cardiovascular (CV) events and all-cause death.
How might this impact on clinical practice?
Clinicians managing patients after acute coronary syndrome should recognise that patient’s self-reported HRQoL is strongly associated with CV events and subsequent mortality.
Introduction
Improved survival following myocardial infarction (MI) has encouraged interest in identifying factors that are associated with subsequent cardiovascular (CV) events.1 Clinicians require evidence about health-related quality of life (HRQoL) to inform clinical decisions for patients with stable coronary artery disease (CAD). Generic tools such as the EuroQol-5 dimension (EQ-5D)2 can provide useful insights into a patient’s well-being and prognosis, including after MI, beyond those offered by disease-specific tools, such as the Seattle Angina Questionnaire.2 3
A systematic review of HRQoL for patients with stable CAD, 1–3 years after MI,4 found major issues with published studies, in that they did not report the approach to assessing HRQoL,5–7 followed up patients for short time periods (up to 1 year post-MI)5–10 and included small samples of patients (≤2000),6 7 9 10 recruited from few countries.7–11 Munyombwe et al identified some factors associated with lower HRQoL, including advancing age and presentation with non-ST-elevation myocardial infarction (NSTEMI).5 Pocock et al found that EQ-5D index score at hospital discharge following MI was an independent predictor of subsequent outcomes.12 13 While these previous studies showed that the EQ-5D can report HRQoL in populations with stable CAD, little research has assessed whether HRQoL predicts subsequent clinical outcomes and resource use.
This article reports HRQoL for patients enrolled 1–3 years post-MI in a prospective, global registry. We aimed to: (1) assess the association of patient characteristics with HRQoL; (2) estimate the association of HRQoL with resource use, CV events and all-cause death; and (3) assess the effect of CV events on change in HRQoL between enrolment and 1-year’s follow-up.
Methods
Study design
TIGRIS (long-Term rIsk clinical manaGement and healthcare Resource utilization of stable coronary artery dISease in post-myocardial infarction patients) is a prospective, global registry of 9126 patients enrolled 1–3 years post-MI, during June 2013–November 2014, from 369 centres across 25 countries in Europe, North America, Latin America, Asia and Australia, who were followed up for 2 years. Details of the TIGRIS Study have been reported.14 15 In brief, patients included were aged ≥50 years with stable CAD, a documented history of MI occurring 1–3 years prior to enrolment and at least one of the following risk factors: age ≥65 years, diabetes mellitus requiring medication, history of a second prior MI, angiographic evidence of multivessel CAD and/or chronic non-end-stage kidney disease. Baseline data at enrolment included relevant medical history, demographics, details regarding the index MI before enrolment, and variables from routine physical examination and laboratory testing, where available.
Data collection and outcome measures
Patients were contacted every 6 months over the follow-up period, either by telephone or hospital visit. At each contact, patients were asked to complete the EQ-5D-3L survey instrument.2 16 The EQ-5D-3L is a generic HRQoL instrument with five dimensions of health (mobility, self-care, usual activities, pain and discomfort, anxiety and depression), for which there are three levels of response (no problems, some problems, severe problems). The EQ-5D-3L profiles reported by each patient were combined with health state preference values from the UK general population,17 to give EQ-5D-3L health state index scores on a scale anchored at 0 (equivalent to death) and 1 (perfect health). Patients were also asked to report their own health status on the EQ-5D Visual Analogue Scale (VAS) from 0 (worst health you can imagine) to 100 (best health you can imagine). In CV disease, the EQ-5D-3L has been used widely internationally and found to have strong convergent validity with other HRQoL measures, and good discriminant ability in detecting differences in health status.1 At each contact, patients were also asked to recall hospitalisations and visits to the emergency room (ER), general practitioner (GP), cardiologist or other specialists over the previous 6 months. These healthcare encounters were summed to report each patient’s resource use over 2-years’ follow-up. If a death occurred, efforts were made to identify the cause (CV or non-CV related). The primary endpoint of the TIGRIS Study was a composite comprising CV death, MI, stroke and unstable angina requiring urgent revascularisation. All outcome events and resource use measures were confirmed by the treating physician or hospital, including determination of final diagnosis, primary cause of hospitalisation, duration of hospital stay, procedures and interventions.
Statistical analysis
We summarised the responses to the EQ-5D-3L questionnaire at baseline enrolment according to the number (%) of patients reporting ‘some’ or ‘severe’ problems for each dimension, and by reporting histograms for the resulting index scores and VAS scores. The EQ-5D index score had a right-skewed distribution18 and had several spikes in its distribution (figure 1). Hence, it has been grouped into four ordered categories: <0.60 (lowest HRQoL); 0.60–0.74 0.75–0.99; and 1 (highest HRQoL). Similarly, we grouped responses to the EQ-5D VAS score into five ordered categories: <60; 60–69; 70–79; 80–89; and ≥90 which represent ‘lowest’ to ‘highest’ self-rated health status.
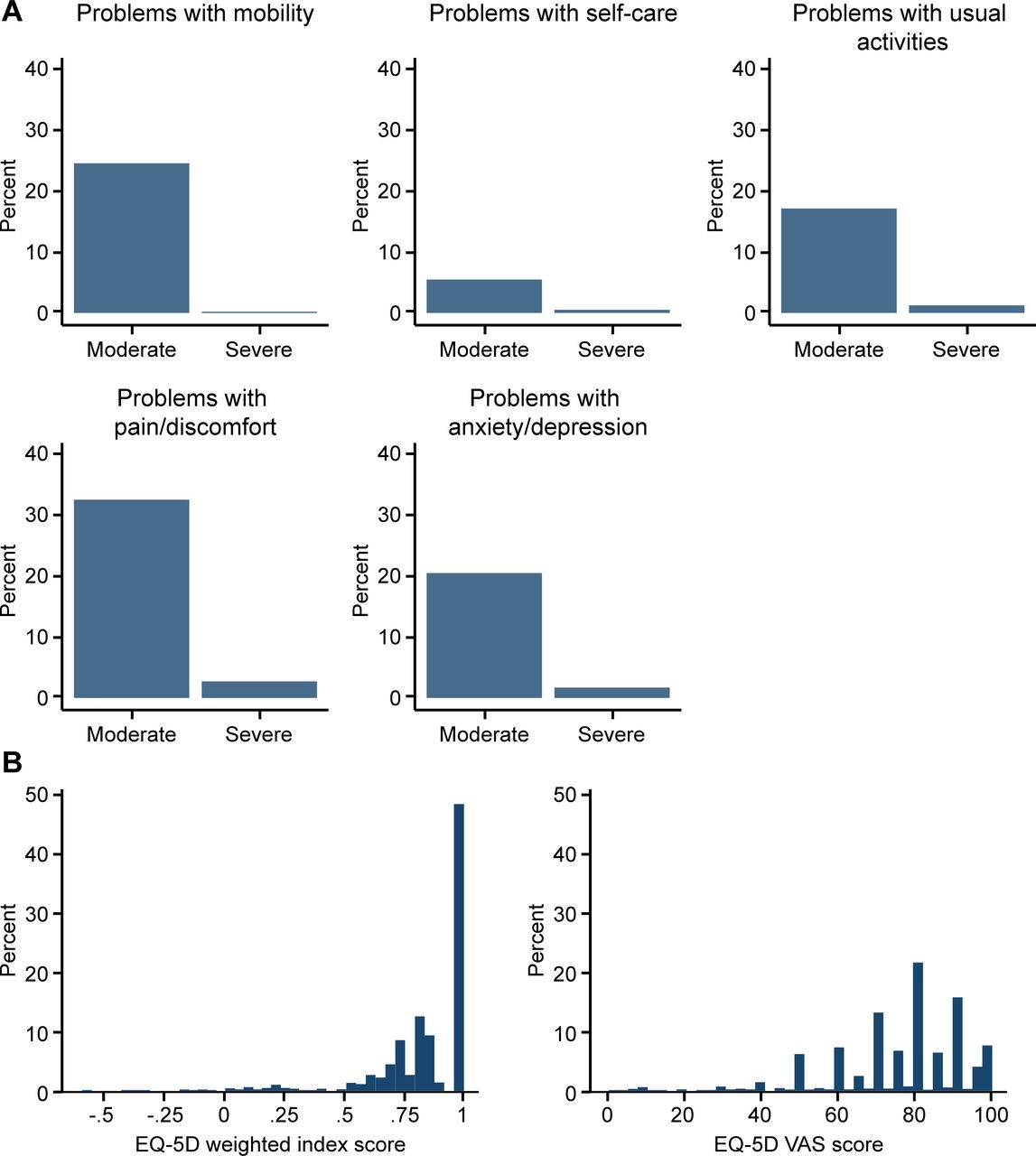
(A) Distributions of the EQ-5D items and (B) the consequent EQ-5D index score and VAS score in 8978 patients at enrolment. EQ-5D, EuroQol-5 dimension; VAS, Visual Analogue Scale.
We estimated the association of clinical factors with the index score category at enrolment using an ordinal logistic regression model. We reported the common OR of being in a ‘lower’ versus ‘higher’ index score category according to the presence versus absence of each risk factor, adjusting for other patient characteristics. We retained independent variables in the regression model according to a forward stepwise procedure with the criteria for an independent association of p<0.01.
We estimated the association of the index score category at enrolment with all-cause death, the composite CV outcome and each resource use measure. For all-cause death and the composite CV endpoint, Poisson regression models were used to recognise that rates were constant over time. We reported the incidence rate ratios and 95% CI for index scores at enrolment in each of the three lower categories, versus the category that represented perfect health. We also reported the association of the VAS score at enrolment with all-cause death and the CV outcome, and considered the association of the index score and VAS score simultaneously, adjusting for other factors.
We reported the association of the index score category and VAS score at enrolment with resource use up to 2 years for patients who survived up to 2 years and who had complete resource use data. Although each of these resource use measures had a right-skewed distribution, we used Ordinary Least Squares regression relying on the central limit theorem, to adjust for patient characteristics in reporting the mean resource use for each index score category as the requisite asymptotic assumptions were plausible, given the sample size.19 For each model, we adjusted for those patient characteristics previously identified in the TIGRIS Study as predictive of prognosis.20 We took the same approach in reporting incidence rate ratios according to the independent association of each of the five EQ-5D health state dimensions at enrolment with both all-cause death and the composite CV outcome, adjusting for other factors.
Finally, we estimated the association of CV events (MI, stroke, unstable angina requiring urgent revascularisation, bleeding event requiring hospitalisation) that occurred between enrolment and 1-year’s follow-up with the mean (95% CI) changes in the EQ-5D index score, and the EQ-5D VAS score over the same time period. We reported associations for those patients with complete data, which assume that HRQoL data were missing at random, conditional on the variables included in the regression model. All analyses were performed using STATA V.15.1.
Results
Baseline patient characteristics
A total of 8978 (99.5%) patients completed EQ-5D questionnaires at enrolment. Table 1 presents key baseline characteristics with accompanying mean EQ-5D index and VAS scores (see also online supplemental table 1 for a fuller list of baseline variables). Before adjustment for potential confounding factors, female sex, increasing age and presence of each comorbidity were each associated with lower mean index and VAS scores. For example, the mean HRQoL index score for men was 0.87 vs 0.77 for women.
Supplemental material
Univariate associations of EQ-5D index score and EQ-5D VAS score by patient characteristics
Figure 1A shows the proportion of patients at study enrolment who reported ‘moderate’ or ‘severe’ problems according to each EQ-5D dimension. Pain and discomfort had the highest prevalence (33.1% ‘moderate’ and 2.7% ‘severe’ problems) followed by ‘mobility’ (24.4% and 0.2%, respectively). Over half (52%) of patients reported a ‘moderate’ or ‘severe’ problem on at least one of the EQ-5D dimensions. Figure 1B summarises EQ-5D index scores at enrolment and shows that 48% of patients had scores of 1 (perfect health), 26% between 0.75 and 0.99, 18% between 0.60 and 0.74%, and 8% less than 0.60.
Associations with index score at enrolment
Table 2 reports the independent association of each factor with the index score category at enrolment in a multivariable model. Compared with men, women were more likely to have lower index scores, with an OR of 1.94 (95% CI 1.76 to 2.14). Other factors significantly associated with a lower index score were older age, obesity, current or ex-smoker, higher heart rate, less formal education, presence of each comorbidity (angina, insulin-treated diabetes mellitus, stroke, peripheral artery disease, prior peptic ulcer, chronic obstructive pulmonary disease, heart failure), ER visit in the previous 6 months and index MI unknown or NSTEMI (vs STEMI). When the VAS score rather than the index score was used as the summary measure of HRQoL, the results were similar (see online supplemental table 2). There were regional differences in the index score (lowest in Latin America, highest in Asia/Australia), whereas the VAS score was lowest in Europe and highest in Latin America.
Multivariable model for factors associated with EQ-5D index score as an ordinal measure with categories 1, 0.75–0.99, 0.60–0.74, <0.60, selected by a stepwise regression procedure using p<0.01 for inclusion
Impact of HRQoL on prognosis
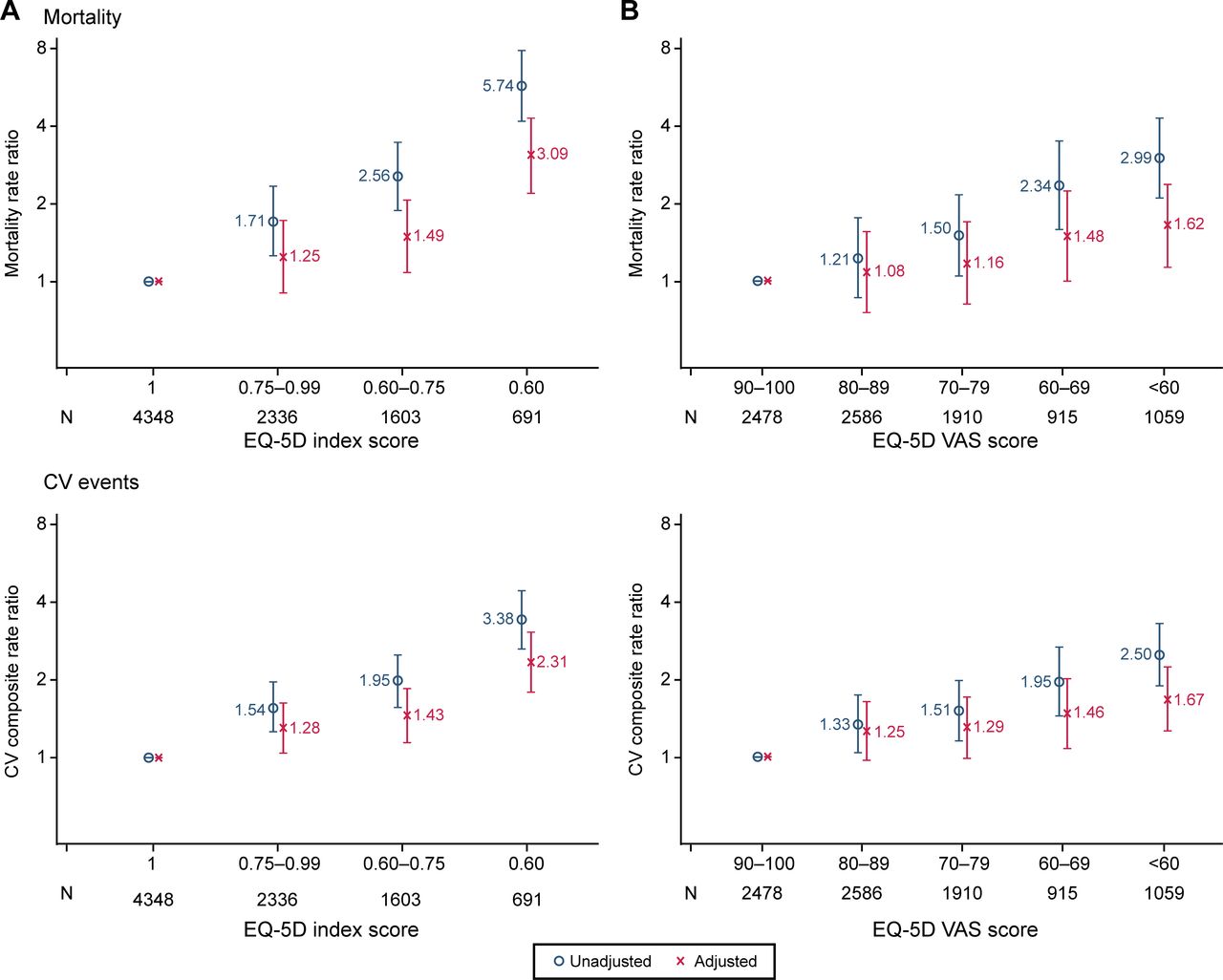
Lower EQ-5D index scores were associated with higher risk of all-cause death and the composite outcome of CV death, MI, stroke and unstable angina requiring urgent revascularisation (figure 2A) over 2-years’ follow-up. Patients with an index score of less than 0.60 and those with scores of 0.60–0.74 had rate ratios of all-cause death of 3.09 (95% CI 2.20 to 4.31) and 1.49 (95% CI 1.07 to 2.07), respectively, compared with those with an index score of 1, after adjustment for differences in other patient characteristics at enrolment. The corresponding rate ratios for the composite outcome were 2.31 (95% CI 1.76 to 3.03) and 1.43 (95% CI 1.12 to 1.82), respectively. The relationships between HRQoL at enrolment and both sets of subsequent outcomes were similar when the VAS score rather than the index score was used to predict subsequent outcomes (figure 2B). When the association of both HRQoL measures were considered simultaneously, the index score was independently associated with increased mortality risk (p<0.001), while the VAS score was not (p=0.84).

The associations of (A) baseline EQ-5D index score and (B) baseline VAS score with mortality and the composite outcome of CV death, MI, stroke and unstable angina requiring urgent revascularisation (using Poisson regression models with and without adjustment for other patient variables). Adjusted for variables in the TIGRIS index model: age ≥65 years; diabetes; second prior MI; chronic kidney disease; heart failure; peripheral artery disease; CV event in past 6 months; prior major bleed; medical management only of index MI; on diuretics at enrolment. CV, cardiovascular; EQ-5D, EuroQol-5 dimension; MI, myocardial infarction; VAS, Visual Analogue Scale.
After adjustment for patient characteristics at enrolment, the EQ-5D dimensions that most strongly associated with all-cause death were problems with ‘self-care’ and ‘mobility’ (table 3), with estimated ORs of 1.70 (95% CI 1.'26 to 2.29) and 1.52 (1.14 to 2.03), respectively. The EQ-5D dimensions of ‘pain/discomfort’ and ‘usual activities’ were most strongly associated with the composite CV outcome. figure 3A reports the association of index scores at enrolment with resource use over 2-years’ follow-up for the 7846 patients who survived to that timepoint and provided complete information. A further 296 patients died, and 840 patients had missing resource use data. Lower index and VAS scores at enrolment were associated with higher subsequent use of healthcare resources, before and after adjustment for other patient characteristics at enrolment (figure 3B). For example, compared with patients who were in ‘perfect health’ at enrolment, the mean numbers of hospitalisations for any reason were 89% higher for patients with index score less than 0.60 and 81% higher for index score between 0.60 and 0.74. Similar patterns emerged for CV-specific hospitalisations, ER visits, visits to the GP and visits to other specialists, but in contrast, visits to cardiologists were less common for those with lower HRQoL.
The associations of the five specific problems in the EQ-5D on (A) all-cause death and (B) the composite outcome of CV death, MI, stroke and unstable angina requiring urgent revascularisation (using Poisson regression models with and without adjustment for other patient variables)

{kind=link}
{kind=link}
{kind=link}
Health resource use over 2-years’ follow-up by baseline self-rated health in 7846 patients with health resource data at every visit (using OLS regression models with and without adjustment for other patient variables). (A) EQ-5D index score and (B) EQ-5D VAS score adjusted for variables in the TIGRIS index model: age ≥65 years; diabetes; second prior MI; chronic kidney disease; heart failure; peripheral artery disease; CV event in past 6 months; prior major bleed; medical management only of index MI; on diuretics at enrolment. CV, cardiovascular; EQ-5D, EuroQol-5 dimension; ER, emergency room; GP, general practitioner; MI, myocardial infarction; OLS, Ordinary Least Squares; VAS, Visual Analogue Scale.
Changes in index score over time
Among survivors, there is no evidence of an overall change in the index score over time. For the 5932 patients with the EQ-5D recorded at every 6-monthly visit, the mean index score was 0.87 at all four follow-up visits vs 0.86 at baseline. For the 2754 patients who were alive at the end of the follow-up period, but missed at least one visit, the mean index score at baseline was 0.83.
The estimated effect of non-fatal CV and bleeding events on a patient’s change in self-rated health over 1 year is shown in table 4. MI, unstable angina requiring revascularisation and a bleeding event requiring hospitalisation occurred in 103, 52 and 46 patients, respectively, and all events were associated with a deterioration in self-rated health. Stroke occurred in 28 patients but showed less impact on self-rated health. These effects were more marked for change in VAS score than for the change in index score, but the patterns were similar.
Influence of clinical events over 1 year on change in self-rated health at 1 year
Discussion
This prospective study of HRQoL 1–3 years post-MI included almost 9000 patients from 25 countries in four continents. The TIGRIS Study was designed to assess the association of clinical factors with HRQoL at enrolment, the effect of HRQoL on subsequent outcomes and resource use, and the change in HRQoL associated with CV events. After adjustment for a full range of patient factors using a previously validated risk model,20 the study found that HRQoL was associated with chronic comorbidities, being female, age >80 years, being obese, fewer years in education and having an NSTEMI index event. A lower index score category at enrolment was associated with a higher subsequent risk of all-cause death, of a major CV event and more hospitalisations over the 2-years’ follow-up period. Patients who experienced any CV event had a reduction in the mean index score between enrolment and 1-year’s follow-up.
We found that the EQ-5D index score at enrolment was on average 0.87 for men vs 0.77 for women, and women were more likely to have lower EQ-5D index scores after adjustment for other factors. In an age−sex matched general population, the corresponding index scores were 0.78 for men and 0.77 for women.21 HRQoL post-MI may be lower for women than men because of a different profile of symptoms in the post-MI period22 and lower access to cardiac rehabilitation services.23 Previous studies reported that women have lower HRQoL than men post-MI but were focused on specific countries and did not consider HRQoL 1–3 years post-MI.3 13 23 24
Previous studies have also found that following MI, HRQoL is lower in older patients, following NSTEMI and for patients with comorbidities.5 25 Lower HRQoL in NSTEMI has been attributed to more symptomatic disease, a history of angina and multimorbidity.5 23 Previous research has found that for chronic disease, more generally, obesity, lower socioeconomic status and presence of comorbidities are associated with lower HRQoL.26–28 Our study is unique in finding that these risk factors were independently associated with HRQoL in the context of a large multinational study. We also found that the mean index score was lower for patients attending centres in Latin America and higher for those in Asia, but it is unclear whether this reflects differences in patient management, severity of their initial MI or other regional features.
Our study shows the importance of HRQoL measured 1–3 years after MI in predicting future events and resource use. We found that poorer HRQoL (ie, a lower EQ-5D index score) predicted a higher risk of all-cause death and a composite of major CV events. While VAS score categories also predicted these outcomes, the associations were weaker, and when both scores were considered simultaneously, the VAS score was not independently associated with these outcomes. Methodological guidelines also support the use of the index score in preference to the VAS score.2 Consistent with a previous systematic review of the use of EQ-5D in CVD,3 we found that the presence of problems on the ‘self-care’ and ‘mobility’ dimensions of the EQ-5D index were most strongly associated with all-cause mortality, whereas problems on the ‘pain/discomfort’ and ‘usual activities’ dimensions were most strongly associated with CV events.
This study estimated the effect of CV events on changes in EQ-5D index scores between enrolment and 1-year's follow-up. Our finding that ‘any CV event’, MI, unstable angina and bleeding event requiring hospitalisation were each associated with a mean reduction in the index score is consistent with previous studies.5–11 22 The PEGASUS-TIMI 54 trial reported decrements of similar magnitude.29 Our study also added to the limited literature that has reported that lower index scores are associated with increased mean number of hospitalisations and ER visits.8 Future studies could use these estimates in cost-effectiveness models that evaluate new treatments for stable patients following MI.
The main strengths of the study are the large sample size, wide spread of centres, prospective design and use of a validated risk adjustment model when examining the association of HRQoL score with subsequent outcomes. A limitation is that CV events during the follow-up period were identified at each centre but were not confirmed by an independent event validation committee. Also, the finding that HRQoL was not significantly lower following stroke may reflect that only few (n=32) patients had this event over 1-year’s follow-up. Also, as assessment of HRQoL at enrolment was at least 1-year post-MI, those who died within a year or did not consent to participate, were excluded. Further research is required to consider the association of HRQoL following MI with subsequent outcomes over longer time periods.
Conclusions
In a large global population of patients enrolled 1–3 years post-MI, self-reported health status provided valuable insights. First, HRQoL is associated with both objective evidence of disease and sociodemographic characteristics. Second, poorer HRQoL is strongly associated with increased hospitalisations. Third, poorer HRQoL 1–3 years after MI is an independent predictor of CV events and all-cause death. We recommend that clinical management post-MI should pay greater attention to patients’ perceptions of their own health status.
Acknowledgments
Editorial support was provided by Cactus Life Sciences (part of Cactus Communications, Mumbai, India) and funded by AstraZeneca.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors SP and RG contributed to the conception and design, data analysis and interpretation of data, and drafting and writing the final version of the manuscript. DBB, RO, JC, MGC, SG, CBG, JCN, TS, DW, SY, KH, CM and KAS participated in the conduct of the registry and revision of the manuscript.
Funding The long Term rIsk, clinical manaGement and healthcare Resource utilization of stable coronary artery dISease (TIGRIS) Study is sponsored by AstraZeneca AB, Södertälje, Sweden.
Disclaimer The sponsor contributed to the study conception and design, and commented on the analyses.
Competing interests SP has received research grant support from AstraZeneca. DBB has received speaker/consulting honoraria and/or research grant support from Amgen, AstraZeneca, Bayer, Boehringer Ingelheim, BMS, Eli Lilly, Merck and Sanofi. RO has received research grant support from AstraZeneca. JC has received research grant support from AstraZeneca and consulting honoraria from MicroPort, APT Medical and JW Medical. MGC has received speaker/consulting honoraria and/or research grant support from AstraZeneca, Medtronic, Abiomed and Merit Medical. SG has received speaker/consulting honoraria and/or research grant support from Amgen, AstraZeneca, Bayer, Boehringer Ingelheim, BMS, CSL Behring, Daiichi Sankyo/American Regent, Eli Lilly, Ferring Pharmaceuticals, GlaxoSmithKline, HLS Therapeutics, Janssen/Johnson & Johnson, Merck, Novartis, Novo Nordisk, Pfizer, Regeneron, Sanofi, Servier and Tenax Pharmaceuticals. CBG has received consulting honoraria and/or research grant support from Armetheon, AstraZeneca, Bayer, Boehringer Ingelheim, BMS, Daiichi Sankyo, Eli Lilly, Gilead, GlaxoSmithKline, Hoffmann-La Roche, Janssen, Metronic, Pfizer, Salix Pharmaceuticals, Sanofi, Takeda and The Medicines Company. JCN has received speaker/consulting honoraria and/or research grant support from Amgen, AstraZeneca, Bayer, BMS, Boehringer Ingelheim, GSK, Merck, Novartis, Pfizer and Sanofi. TS has received speaker/consulting honoraria and/or research grant support from Astellas, Amgen, AstraZeneca, Bayer, Boehringer Ingelheim, Eli Lilly, GlaxoSmithKline, Merck, Novartis, Pfizer and Sanofi. DW has received speaker/consulting honoraria and/or research grant support from AstraZeneca, Bayer, Berlin-Chemie, Biotronik and Novartis. SY has received speaker/consulting honoraria and/or research grant support from Takeda, Daiichi Sankyo, AstraZeneca, Boehringer Ingelheim and BMS. KH, CM and KAS are employees of AstraZeneca.
Patient consent for publication Not required.
Ethics approval All patients provided written informed consent. The study protocol was approved by the corresponding health authorities and ethics boards for all participating study sites. This includes China HGR approval of inclusion of 750 Chinese patients.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request. Data underlying the findings described in this manuscript may be obtained in accordance with AstraZeneca’s data sharing policy described at https://astrazenecagrouptrials.pharmacm.com/ST/Submission/Disclosure.