Article Text

Abstract
Objectives To characterise and risk-stratify patients presenting to a heart failure (HF) clinic according to the National Institute for health and Care Excellence (NICE) algorithm.
Methods This is an observational study of prospectively collected data in the Sheffield HEArt Failure registry of consecutive patients with suspected HF between April 2012 and January 2020. Outcome was defined as all-cause mortality.
Results 6144 patients were enrolled: 71% had HF and 29% had no HF. Patients with N-terminal pro-brain-type natriuretic peptide (NT-proBNP) >2000 pg/mL were more likely to have HF than those with NT-proBNP of 400–2000 pg/mL (92% vs 64%, respectively). Frequency of HF phenotypes include: HF with preserved ejection fraction (HFpEF) (33%), HF with reduced ejection fraction (HFrEF) (29%), HF due to valvular heart disease (4%), HF due to pulmonary hypertension (5%) and HF due to right ventricular systolic dysfunction (1%). There were 1485 (24%) deaths over a maximum follow-up of 6 years. The death rate was higher in HF versus no HF (11.49 vs 7.29 per 100 patient-years follow-up, p<0.0001). Patients with HF and an NT-proBNP >2000 pg/mL had lower survival than those with NT-proBNP 400–2000 pg/mL (3.8 years vs 5 years, p<0.0001). Propensity matched survival curves were comparable between HFpEF and HFrEF (p=0.88).
Conclusion Our findings support the use by NICE’s HF diagnostic algorithm of tiered triage of patients with suspected HF based on their NT-proBNP levels. The two pathways yielded distinctive groups of patients with varied diagnoses and prognosis. HFpEF is the most frequent diagnosis, with its challenges of poor prognosis and paucity of therapeutic options.
- heart failure
- epidemiology
- diastolic
- systolic
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known about this subject?
Since the publication of the Chronic Heart Failure National Institute for health and Care Excellence (NICE) guidelines of 2010, which was updated in 2018, there was no published demonstration of its application in the real world until this year 2020. Recently, colleagues from Portsmouth and Southampton published their experience with the application of the diagnostic algorithm of these guidelines in a smaller cohort than ours. Their experience suggested that 53% of the patients presented with N-terminal pro-brain-type natriuretic peptide (NT-proBNP) >2000 pg/mL. The diagnostic yield of NICE’s NT-proBNP threshold in their cohort was 55%, much lower than expected from the research literature. They found no difference in the survival between those with and without heart failure.
What does this study add?
Our study reports on an almost 8-year experience with a large consecutive cohort of patients reflecting the incidence of heart failure in the community in Sheffield, an English city with 551 800 inhabitants. We believe that our findings provide an insight into the real-world incidence of heart failure in the community, and demonstrate the value of the diagnostic algorithm suggested by NICE guidelines.
Our study showed the diagnostic yield of NICE’s NT-proBNP threshold (400 pg/mL) is 71%, with the majority of the patients presenting with NT-pro BNP of 400–2000 pg/mL. The study provides an insight into the survival rate of the different heart failure phenotypes and looks into the impact of the height of NT-proBNP, the symptom burden stipulated by the New York Heart Association functional class and the stages of chronic kidney disease on the prognosis. The study showed that there is no difference in the survival rate between those with heart failure and reduced or preserved ejection fraction, similar to the experience shown in acute heart failure setting among hospitalised patients in the UK National Heart Failure audit.
Key questions
How might this impact on clinical practice?
The data we provide demonstrate the prominence of heart failure with preserved left ventricular ejection fraction as the most common diagnosis encountered in the community. This particular syndrome remains deprived of any evidence-based effective therapy. This calls on the medical and scientific community to concentrate the efforts into further research into the patho-physiology, prevention and treatment of the patients with this heart failure phenotype.
Introduction
Heart failure (HF) is common (26 million patients worldwide) and is one of the leading causes of morbidity and mortality.1 HF predominantly affects people aged 50 years and beyond,2 and adversely affects patients’ quality of life and survival. It poses an economic burden on the National Health Service of the UK.3 Early and accurate diagnosis and management of HF are paramount to alleviate symptoms, improve prognosis and lead to more cost-effective healthcare delivery.4
The National Institute for health and Care Excellence (NICE) produced a diagnostic algorithm for the patients suspected of HF.5 Thus, patients are referred for transthoracic echocardiography (TTE) and specialist assessment based on clinical presentation and measurement of N-terminal pro-brain-type natriuretic peptide (NT-proBNP). The diagnostic algorithm recommends patients are seen and assessed within 2 weeks if NT-proBNP >2000 pg/mL and within 6 weeks if NT-proBNP is 400–2000 pg/mL.5
Although the guidelines were published 10 years ago, limited data are available on the performance of the diagnostic algorithm.6 Reliable and contemporary description and characterisation of the population with HF is important to develop insight into HF trends, recognise clinical outcomes, and to improve and shape both current services and future clinical HF pathways.
The main objectives of this study are: first, to characterise real-world patients presenting to a HF clinic serving the city of Sheffield in the UK; second, to stratify patients whose diagnosis followed the established NICE HF diagnostic algorithm; and finally, to explore and investigate predictors of all-cause mortality in subphenotypes of HF defined in line with NICE guidelines 2010 (CG108) and its update in 2018 (NG106).5 7
Methods
Data and patients
Patients suspected of HF from a population of 551 800 are screened by their general practitioners (GPs) using a single measurement of NT-proBNP. In accordance with NICE guidelines, those with symptoms and/or signs suggestive of HF and a raised NT-proBNP (threshold 400 pg/mL) are referred to the HF clinic in Sheffield.5 7 Data were collected prospectively and electronically encrypted with an annual data validation check. The analytical cohort was derived from all patients presenting to this HF clinic between 13 April 2012 and 31 January 2020. The inclusion criteria were: age 18 years or over, raised NT-proBNP (>400 pg/mL) and symptoms and/or signs suggestive of HF. Exclusion criteria were: incomplete TTE study, or absence of NT-proBNP measurement.
HF assessment
All patients referred to the HF clinic by their GPs with NT-proBNP >400 pg/mL underwent a resting 12-lead ECG and TTE. Each patient was clinically assessed by a specialist. The final diagnosis was determined by the HF specialist integrating the presenting history, clinical examination and the results of investigations in keeping with NICE guidelines.5 8
The patients with HF were subdivided into five phenotypes: HF with preserved ejection fraction (HFpEF), HF with reduced ejection fraction (HFrEF), HF due to pulmonary hypertension (HF-PH) where the only cardiac abnormality is pulmonary artery pressure of >40 mm Hg, HF due to right ventricular systolic dysfunction (HF-RVSD) where the only cardiac abnormality is the systolic impairment of the right ventricle, and HF due to valvular heart disease (HF-VHD) where severe valvular disease is the only abnormality responsible for the syndrome of HF. It is recognised that pulmonary hypertension, RVSD and severe valvular disease could coexist with either HFrEF or HFpEF. In those circumstances, the patients were assigned as having HFrEF or HFpEF, respectively.
Study variables
Clinical and TTE variables are detailed in online supplemental file. The 12-lead ECG documented: rhythm (sinus, atrial fibrillation, atrial flutter or paced), QRS duration, left axis deviation, ST/T-wave changes, presence of ectopic beats, any conduction delays or atrioventricular blocks and presence of left ventricle (LV) hypertrophy using the standard voltage criteria.9 Similarly, details of the TTE findings were recorded in the database.
Supplemental material
Statistical analysis
Statistical analyses were performed in MedCalc V.19.0.5. Categorical baseline characteristics are described with numbers and percentages. Continuous variables are described using means and SD. Comparison of continuous variables was done using an independent t-test, while the comparison of categorical variables was done using Χ2 t-test. Mortality rates are presented as per 100 patient-years (100PY) of follow-up (FU). Kaplan-Meier (KM) curves were used to visualise and interpret the data of variables associated with mortality. KM curves used the log-rank test to investigate the differences in curves between alive and dead patients at FU. Further survival analysis was done using propensity score matching for all clinical demographics which demonstrated association to all-cause mortality. In addition to propensity matched score method, we also tested the difference of survival curves between HFpEF and HFrEF using Cox’s proportional hazard model.10 The Kruskal-Wallis one-way analysis of variance test was used to investigate the overall differences in clinical characteristics, the New York Heart Association (NYHA) symptom burden and chronic kidney disease (CKD) distribution of different subphenotypes of HF. All tests were two-sided, and statistical significance was considered if p value was <0.05.
Results
Patient characteristics
The demographic data and patient characteristics are summarised in tables 1 and 2. In almost 8 years’ duration, 6272 patients were assessed in our HF clinic. From the total cohort, 128 (2%) patients had other disorders (non-cardiac such as pulmonary fibrosis and cancer, and cardiovascular such as atrial arrhythmias, and pure valvular disease such as aortic stenosis without HF) and were excluded from further analysis. The study cohort was thus 6144 patients. Of this referred cohort of patients, 4368 patients (71%) were diagnosed with HF and 1776 patients (29%) did not have HF. Patients with HF were older (80±9 years vs 78±9 years, p<0.01), had higher mean NT-proBNP levels (2593±8918 pg/mL vs 946±810 pg/mL, p<0.01) and had higher NYHA functional class (2.3±0.7 vs 1.8±0.7, p<0.01) than the patients with no HF. Women comprised 54% of those with HF. For the total population, the mean NT-proBNP was 2114.4±7501 pg/mL.
Study demographics
Patient characteristics in various heart failure subcategorisations
Compared with the patients with no HF, those with HF had higher prevalence of comorbidities such as systemic hypertension (65% p=0.032), CKD (60% p<0.01) and ischaemic heart disease (36% p<0.01). Similarly, more patients with HF had VHD, previous myocardial infarction (MI), diabetes mellitus (DM) and hypercholesterolaemia (p<0.01). Nearly one-third of the referred patients were smokers (28% of those with no HF vs 38% of those with HF). On the other hand, there was no statistically significant difference in the incidence of chronic obstructive pulmonary disease (COPD) between patients with HF and without HF. Surprisingly, obesity was not a statistically significant comorbidity in any of the phenotypes of patients with HF.
NT-proBNP >2000pg/mL vs NT-proBNP 400–2000pg/mL
Patients with NT-proBNP >2000 pg/mL, using the 2-week pathway of the diagnostic algorithm, were 1624 patients (26.4% of the referred cohort). The remaining 4520 patients (73.6%), who had NT-proBNP 400–2000 pg/mL, used the 6-week pathway.
Patients with NT-proBNP >2000 pg/mL had a higher chance of having HF compared with those with NT-proBNP of 400–2000 pg/mL (92% vs 64%, respectively) (figure 1). Patients with HFpEF were similarly distributed between the 2-week and 6-week pathways (31% and 34%, respectively). The similarity in distribution between those with NT-proBNP of 400–2000 pg/mL and those with NT-proBNP >2000 pg/mL was also noted in those with HF-PH, HF-VHD and those with HF-RVSD. On the other hand, HFrEF was the single most common HF diagnosis (50%) among the patients with NT-proBNP of >2000 pg/mL.

Final diagnosis in heart failure clinics for the whole population. (A) Histogram of the number of patients in each category of diagnosis. From a total of 6144 patients seen in the HF clinic, 29% of patients did not have HF. (B) In patients with NT-proBNP > 2000pg/ml, HFrEF was the main presenting diagnosis (50%) which was followed by HFpEF (31%).HF, heart failure; HFpEF, HF with preserved ejection fraction; HF-PH, HF with pulmonary hypertension; HFrEF, HF with reduced ejection fraction; HF-RVSD, HF with right ventricular systolic dysfunction; HF-VHD, HF with valvular heart disease; NT-proBNP, N-terminal pro-brain-type natriuretic peptide.
Phenotypes of HF
Table 2 shows the characteristics of the five phenotypes of the population with HF. Patients with HFrEF are significantly younger than patients with HFpEF and patients with HF-VHD. Of the 6144 referred cohort, HFpEF was the most common phenotype seen in 2022 patients (33%), whereas HFrEF affected 1759 patients (29%). Patients with HFpEF had a lower mean NT-proBNP levels (1780±311 pg/mL) than those with HFrEF (3603±1345 pg/mL) or HF-VHD (2698±362 pg/mL). Male patients predominated among those with HFrEF (60%) and with HF-RVSD (64%). There was female predominance in those with HFpEF (66%), HF-VHD (61%) or HF-PH (56%).
Symptom burden in HF phenotypes
With an increase in HF symptom burden, HFrEF, HF-PH and HF-RVSD become more prevalent (p<0.0001) (figure 2A). HF-RVSD and HF-PH are more common in the patients presenting in NYHA functional class IV than those presenting in NYHA functional classes I–III. HFpEF is the diagnosis of the largest group of patients with NYHA classes I and II (48% and 49%, respectively), while representing only 23% of those presenting with NYHA functional class IV. This suggests that the majority of the patients with HFpEF have milder symptoms. In contrast, HFrEF is the diagnosis in 50% of the patient cohort in NYHA functional class IV.
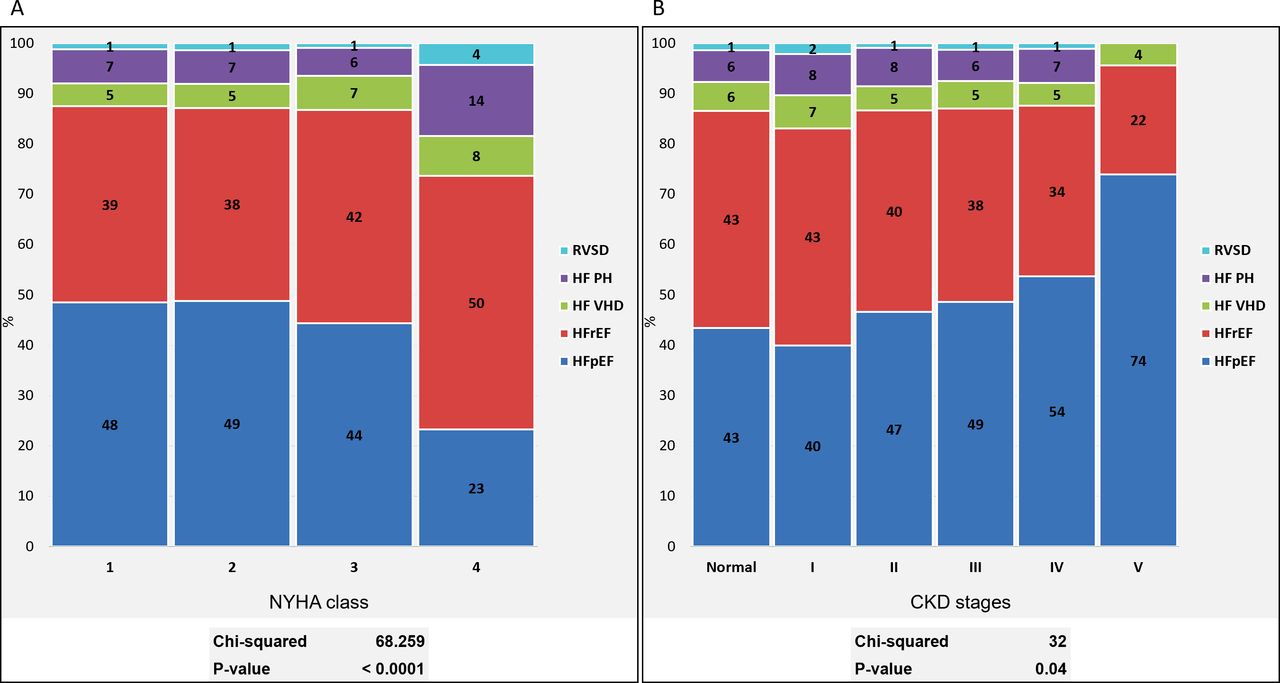
Stacked histogram demonstrating the percentage of patients with a specific HF diagnosis in each category of NYHA and CKD stage. (A) Patients with HFpEF were predominantly in NYHA functional class I/II, versus patients with HFrEF, who were predominantly in NYHA functional class IV. (B) HF patients with a diagnosis of HFpEF were more likely to have worse CKD stage than any other type of HF diagnosis. CKD, chronic kidney disease; HFpEF, heart failure with preserved ejection fraction; HF-PH, heart failure with pulmonary hypertension; HFrEF, heart failure with reduced ejection fraction; NYHA, New York Heart Association; RVSD, right ventricular systolic dysfunction; VHD, valvular heart disease
The HF phenotypes in different stages of renal dysfunction (CKD)
HFpEF was the diagnosis of 74% of the patients with HF and CKD stage V (figure 2B). In contrast, patients with HFrEF constituted 34%–43% of those with the other CKD stages. However, it is important to note that of the complete cohort, CKD stage V only represented 0.6% of the population (online supplemental figure 1). Thus, the observed increased incidence of HFpEF in CKD V is unlikely to have an impact on the outcomes of the cohort.
Supplemental material
Survival analysis
Of the referred cohort, there were 1485 (24%) deaths over a maximum FU period of 6 years (mean FU 2.3±2 years). The death rate was significantly higher in patients with HF (11.5 (95% CI 11 to 12.2) vs 7.3 (95% CI 6.5 to 8.2) per 100PY, p<0.0001).
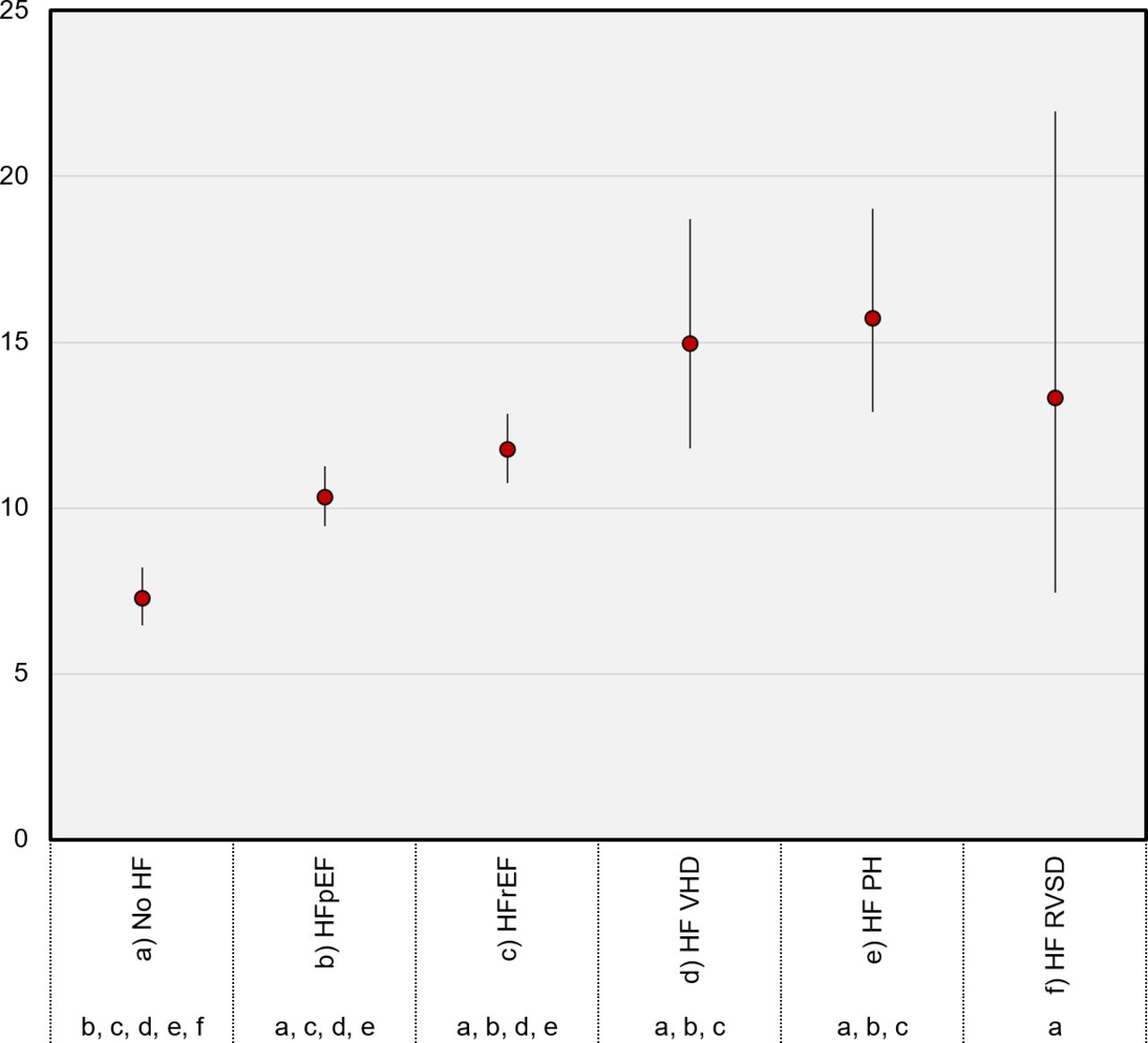
The all-cause mortality as measured per 100PY of the patients with HF demonstrated an ascending order of the HF phenotypes: HFpEF (10.3 (95% CI 9.4 to 11.3) per 100PY), HFrEF (11.8 (95% CI 10.8 to 12.8) per 100PY), HF-RVSD (13.3 (95% CI 7.5 to 22) per 100PY), HF-VHD (15 (95% CI 11.8 to 18.7) per 100PY) and the highest was HF-PH (15.7 (95% CI 12.9 to 19) per 100PY). There was no statistically significant difference between the mortality of those with HF-PH, HF-VHD or HF-RVSD. However, the differences were significant between those with HFpEF and HFrEF; and between each of those and the categories with the highest mortality (HF-PH and HF-VHD) (figure 3). The median age for those with HFpEF was 81±8 years of age and the median age of those with HFrEF being 78±10 years of age (p<0.01). However, since the patients with HFrEF are not particularly young, this difference may not have a significant biological difference.

Incidence of all-cause mortality in each sub-phenotype of heart failure per 100 patient-years. Statistical significant changes to other groups are highlighted with letters representing the specific group. The lines represent the 95% confidence interval. HF, heart failure; HFpEF, HF with preserved ejection fraction; HF-PH, HF with pulmonary hypertension; HFrEF, HF with reduced ejection fraction; HF-RVSD, HF with right ventricular systolic dysfunction; HF-VHD, HF with valvular heart disease.
On KM analysis, the survival curves were wide apart between those with no HF versus the patients with HF over the long- term FU period (χ2=47.14, p<0.0001) (figure 4A). Whereas, the survival curves were not significantly different between HFpEF and HFrEF (χ2=3.63, p=0.06).
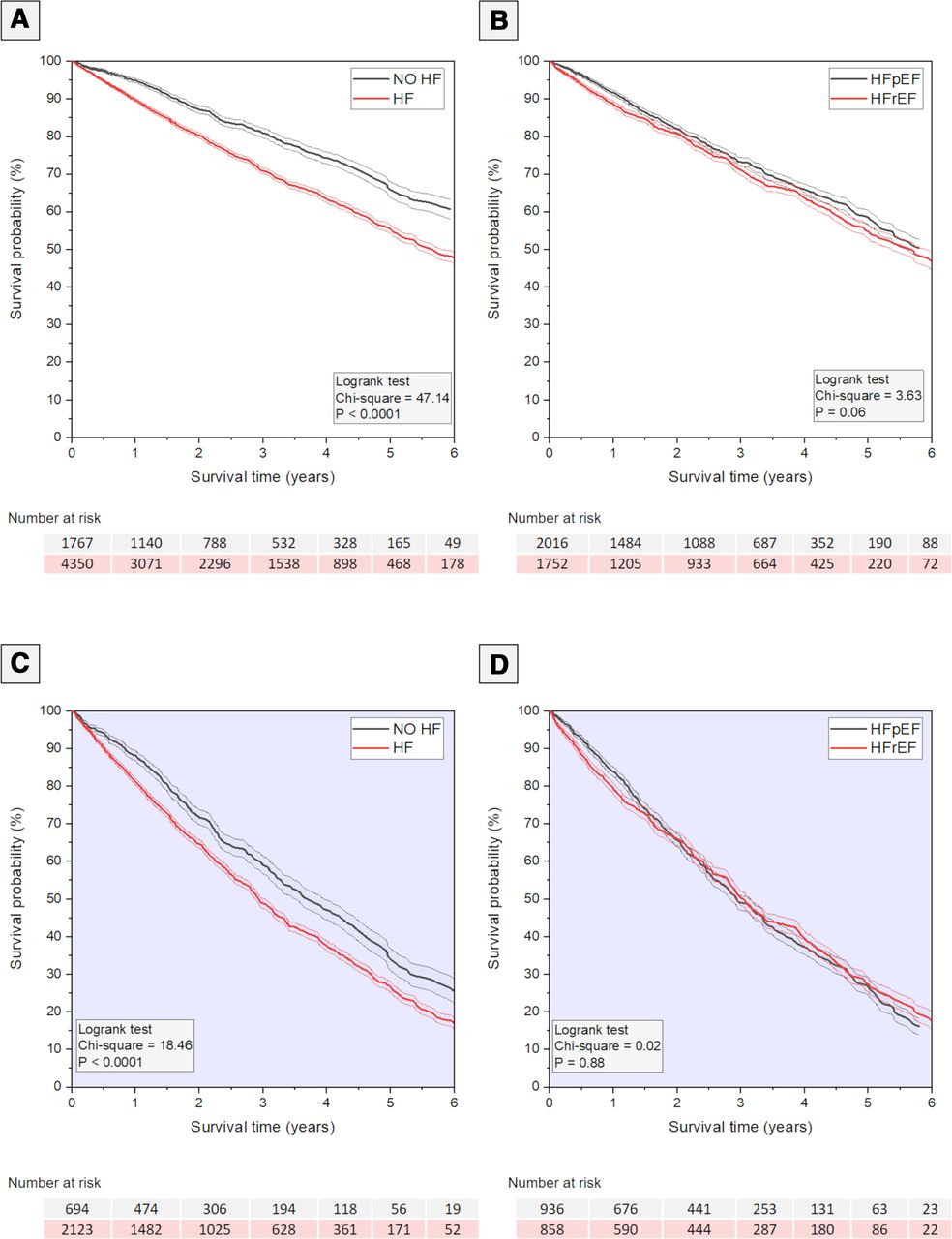
Kaplan-Meier survival curves. (A and B) Survival comparison of patients with versus without HF and with HFpEF versus HFrEF, over a follow-up period of up to 6 years. (C and D) Propensity matched survival comparison of patients with versus without HF and with HFpEF versus HFrEF, over a follow-up period of up to 6 years. HF, heart failure; HFpEF, HF with preserved ejection fraction; HFrEF, HF with reduced ejection fraction.
Patients with HF and an NT-proBNP ≥2000 pg/mL had significantly worse survival rate than patients with lower NT-proBNP levels (3.8 years vs 5 years, χ2=173.5, p<0.0001) (figure 5).

Kaplan-Meier survival curves. (A and B) Survival comparison of patients with NTproBNP 400-1999pg/ml versus ≥NTproBNP 400-1999pg/ml, and in different NYHA functional status, over a follow-up period of up to 6 years. (C and D) Propensity matched survival comparison of patients with NTproBNP 400-1999pg/ml versus ≥NTproBNP 400-1999pg/ml, and in different NYHA functional status, over a follow-up period of up to 6 years. NT-proBNP, N-terminal pro-brain-type natriuretic peptide; NYHA, New York Heart Association.
Worsening NYHA functional class was similarly associated with worsening mean survival (NYHA I: 4.8 years; NYHA II: 4.9 years; NYHA III: 4.2 years and NYHA IV: 2.47 years, χ2=221.3, p<0.0001) (figure 5B). On KM analysis, the obvious deterioration in survival rate started with NYHA functional class III and became marked with NYHA functional class IV.
For comparing patients with HF versus those with no HF, and for comparing those with HFpEF versus those with HFrEF, the following covariates demonstrated association to outcome and were used in propensity matching: age, NT-proBNP level, male gender, obesity, hypertension, DM, hypercholesterolaemia, COPD, dementia, VHD, MI, stroke and renal impairment.
When comparing the survival of patients in different NYHA functional classes, all of the above variables were included for propensity matching, except NT-proBNP level that was replaced by phenotype diagnosis.
Post-propensity matching, the differences between the survival curves were less for the comparison of patients with no HF versus patients with HF than those seen on KM analysis before propensity matching, but remained statistically significantly different (χ2=18.46, p<0.0001) (figure 4C). The survival curves of HFpEF and HFrEF almost overlap demonstrating no actual difference in survival over time (χ2=0.02, p=0.88) (figure 4D). By adjusting for covariates using the Cox’s proportional hazard model, the survival trend was worse for HFrEF, but this again remained statistically not significant (figure 6). The differences in survival curves remained statistically significantly different for both NT-proBNP and NYHA functional class after propensity matching (figure 5).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Kaplan-Meier curves comparing HFpEF and HFrEF survival. These curves have been adjusted for covariates using the Cox’s proportional-hazards regression. CKD, chronic kidney disease; COPD, chronic obstructive pulmonary disease; HFpEF, heart failure with preserved ejection fraction; HFrEF, heart failure with reduced ejection fraction; MI; myocardial infarction; NT-proBNP, N-terminal pro-brain-type natriuretic peptide; VHD, valvular heart disease.
Discussion
Our study sought to characterise the patients referred from the community to the HF clinic using NICE diagnostic algorithm5 and to investigate their outcomes. Until this year 2020, these have remained largely untested.
We prospectively entered all patients referred to the HF clinic into the SHEAF registry.11 We excluded the few patients before 2013 whose entry into the diagnostic algorithm was through a history of MI. We observed that GPs tended to test the NT-proBNP even when there was a history of MI. Zheng et al6 made a similar observation to ours. The majority of the patients with a history of MI referred to our HF clinic in that first year had NT-proBNP levels <2000 pg/mL. Thus, these patients were entered into the 6-week pathway. We have amended the protocol making raised NT-proBNP as the single port of entry into the diagnostic HF service. This modification was subsequently adopted by NICE in the chronic HF guidelines (NG106-2018).7
The most common phenotype of HF in the community patients in the SHEAF registry was HFpEF. Indeed, one of the step changes in the HF NICE guidelines (CG108) of 2010 was the introduction of the almost universal use of natriuretic peptides (NPs) by GPs as the main port of entry into the HF diagnostic algorithm.5 This key investigation to access HF diagnostic services in secondary care is based on its high specificity at the thresholds chosen.12 13 Prior to those guidelines, many cases of HFpEF were undiagnosed. Within the diagnostic algorithm, the referred patients are triaged into a 2-week and 6-week pathways based on the level of the NPs. This was due to the poor short-term and medium-term outcomes shown in patients with HF and very high NP levels.14 Thus, patients with NT-proBNP >2000 pg/mL have their TTE and see the specialist within 2 weeks, while those with NT-proBNP 400–2000 pg/mL have the TTE and the specialist’s review within 6 weeks. Providing patients with early specialist review to ensure the correct diagnosis is made and the appropriate management plan is implemented are known to improve outcomes.9
The HF NICE guidelines of 2010 (CG108) and of 2018 (NG106) chose the diagnostic threshold for NT-proBNP at 400 pg/mL. This is at variance with the European Society of Cardiology (ESC) threshold of 125 pg/mL.15 16 The ESC approach is based on ruling out HF, at the expense of low specificity at that threshold. This approach can potentially overwhelm echocardiography services and specialist clinics.17 The cost-effectiveness of NICE approach of using NT-proBNP as a gatekeeper for the diagnosis of HF has been further confirmed by the work of Taylor et al.7 17
We recognise that elevated NT-proBNP is an independent risk factor for cardiovascular events and mortality in the general population.18 Indeed, we demonstrated that those with no HF (29%) suffered mortality rate at 7.3 (95% CI 6.5 to 8.2) per 100PY. We have published the clinical predictors of mortality in this group of people.11 The patients diagnosed with HF had a significantly higher mortality rate of 11.5 (95% CI 11 to 12.2) per 100PY.
Biomarkers of myocardial fibrosis in patients with chronic HF (soluble ST2 receptor, galectin-3 and high sensitivity cardiac troponin) were proposed as additives to NP in aiding prognostication of patients with HF.19–21 Whether we adopt novel cardiac biomarkers as an adjunct to NT-proBNP in the triage or prognostication process remains to be seen.
Among our cohort of 6144 patients, 26.4% entered the 2-week pathway (NT-proBNP >2000 pg/mL), while 73.6% entered the algorithm via the 6-week pathway (NT-proBNP 400–2000 pg/mL). Those percentages follow a natural distribution pattern, but are at odds with those of Zheng et al6 as 53% of their patients used the 2-week pathway.
In our cohort, 71% of the patients with NT-proBNP >400 pg/mL had HF, which is close to the expected yield of diagnostic studies that formed the basis of NICE’s choice of that threshold.5 7 13 Furthermore, there was a higher diagnostic yield (92%) with the NT-proBNP >2000 pg/mL versus a diagnostic yield of 64% when NT-proBNP is 400–2000 pg/mL. It was interesting to note that in their recently published study, Zheng et al6 reported a low diagnostic yield of the same NT-proBNP threshold of >400 pg/mL at only 55%.
While our study and that of Zheng et al6 have implemented the same diagnostic algorithm by NICE,5 our results appear to reflect potentially different incidence of HF in the community. Their two centres serve a population of 1 175 000 people. Portsmouth and Southampton contributed to their study for 35 months and 24 months, respectively. Their 1271 referrals suggested that Southampton received 2 referrals/100 000/month, and Portsmouth received 4 referrals/100 000/month. In contrast, in Sheffield we serve a population of 551 800, and received 6144 referrals in 93 months, at a mean rate of 12 referrals/100 000/month.
Notwithstanding the differences between our findings and those by Zheng et al, it is important to recognise that observational studies like ours and theirs are significantly affected by the epidemiological differences related to the different characteristics of the populations each of our groups serves, and the impact of referral patterns by primary care.
Unsurprisingly, the survival analysis of our larger registry showed the mortality rate is higher among our patients with HF versus those with no HF table 3(figure 4). While the two groups were similar in age and comorbidities, the main difference between them is the presence of any form of HF. Taylor et al22 published a population-based cohort study in the UK from primary care data of 55 959 new diagnoses of HF over 17 years. The survival trends were significantly worse at 1 year, 5 years and 10 years in the HF versus no HF groups. These findings are consistent with what we observed in the SHEAF registry. In contrast, Zheng et al6 reported no difference in the survival between the HF versus no HF groups, which is surprising.
Other findings of interest are the impact on the prognosis of both the degree of rise in the NT-proBNP and the severity of symptoms at presentation as defined by the NYHA class. Those presenting with NT-proBNP >2000 pg/mL survived on average 1.2 year less than those presenting with NT-proBNP of 400–2000 pg/mL. Similarly, there was a 2.33 years difference in survival between those with NYHA functional class I at presentation and those presenting with NYHA functional class IV.
We have confirmed the findings of others23 as we demonstrated that those with HF-PH have an even higher mortality than those with HFpEF or HFrEF (figure 3).
Those who emphasise the impact of lower left ventricular ejection fraction (LVEF) on survival feel that patients with HFrEF should have higher mortality than those with HFpEF. Others may attach more emphasis on the impact of comorbidities such as advanced CKD or characteristics such as ageing. A third group may believe that the absence of effective therapy for patients with HFpEF should increase their mortality rate compared with the patients with HFrEF. In our study, the mortality at 100PY FU showed statistically significant difference between those with HFpEF and those with HFrEF. However, when we adjusted for covariates using the Cox’s proportional hazard model (figure 6), the KM survival curves showed no statistically significant difference between the two groups. As our dataset is a large one, we have appropriately used propensity matched analysis representing real data instead of adjusting for the mean of covariates. The latter method produced KM survival curves of HFpEF and HFrEF that almost overlapped demonstrating no actual difference in survival over time (figure 4D). Thus, we confirmed there is no statistically significant difference between the survival of patients with these two phenotypes of HF over a maximum FU of 6 yearstable 3.
Not unlike our findings, Ambrosy et al24 showed that while there is a trend toward lower in-hospital mortality among hospitalised patients with HF with HFpEF in the Get With The Guidelines-HF programme, FU data from the Organized Program to Initiate Lifesaving Treatment in Hospitalized Patients With HF registry suggest that post-discharge survival is poor irrespective of EF. In other words, when one extends the FU beyond the first 3 months, one would be surprised to find similar survival in both groups. Similarly, Varela-Roman et al demonstrated no effect of LVEF on the survival.25
These are similar to other studies including the results from the UK HF national audit. An older cohort studied between 1987 and 2001 showed small differences in the mortality of patients with HFpEF and patients with HFrEF, at 1 and 5 years (29% vs 32%, and 65% vs 68%, respectively).26 The latter series predates the impact of major advances in therapeutics for HFrEF, with beta-blockers and mineralocorticoid antagonists. Thus, the improved survival of patients with HFrEF coupled with absence of disease-modifying therapy for HFpEF27 allowed the outcomes of these two phenotypes of HF to become similar.
We propose that a UK-wide diagnostic HF registry is established along the lines we established in the SHEAF registry in Sheffield. This will require several conditions to be met as described in a recent editorial in Heart.28
Clinical perspective
This is the largest published registry of an HF clinic in the UK and is the second description of the implementation of the diagnostic algorithm of NICE HF guidelines.5 7 The prospective entry of data by specialists in HF, and the fact the clinic serves the whole population of patients with suspected HF in one city improves our confidence that the characterisation of the patients enrolled is a true representation of such a population.
Limitations
There are four limitations: we are uncertain that all the patients reporting symptoms of HF were tested and referred, we do not know if there were patients suspected of HF with raised NT-proBNP who were not referred to the service, there were patients whose HF diagnosis was made when they were admitted acutely with HF bypassing our clinic, and finally we have not been able to provide detailed analysis of patients without complete TTE due to lack of data.
Conclusion
Our findings support the use by NICE’s HF diagnostic algorithm of tiered triage of patients with suspected HF based on their NT-proBNP levels. The two pathways yielded distinctive groups of patients with varied diagnoses and prognoses. We recognise the eminence of HFpEF as the most frequent diagnosis, with its challenges of poor prognosis and paucity of therapeutic options. This demands of all of us to work harder to investigate the pathophysiology, course and potential management of HFpEF.
Acknowledgments
We thank the Sheffield Teaching Hospitals Heart Failure services in their pursuit to collect, record and manage the data used for this study.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @HosamAssadi, @AAlMohammad87
Contributors PG and AA-M conceptualised and organised the study. GF, NL, DR, AC and AA-M facilitated data collection. AJS and PG did all the statistical analyses. AJS facilitated the ethical approval. HA, UN and AD helped draft the initial manuscript. PG drafted and revised figures and tables. AA-M and PG provided critical input into the content and discussion regarding the findings of the study. All authors took part in critical review and drafting of the manuscript, and have read and approved the final manuscript.
Funding AJS is supported by Wellcome Trust (AS: 205188/Z/16/Z). PG is supported by the Academy of Sciences Starter Grant (PG: SGL018/1100).
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The Sheffield HEArt Failure registry (SHEAF registry) has been sanctioned by the local 3D-lab committee under the registration number 222349P4. This has the appropriate research ethics committee approval (17/YH/0142). This study complies with the Declaration of Helsinki.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as online supplemental information.