Article Text

Abstract
Objectives Patients’ backgrounds and clinical outcomes in urgent/emergent/salvage transcatheter aortic valve replacement (Em-TAVR) remain unclear. We investigated patient characteristics and the mortality in Em-TAVR and the predictors for the need for Em-TAVR.
Methods We consecutively enrolled 1613 patients undergoing TAVR for severe aortic stenosis between October 2013 and July 2016 from the Optimised transCathEter vAlvular interventioN (OCEAN)-transcatheter aortic valve implantation (TAVI) registry. The urgency was based on the European System for Cardiac Operative Risk Evaluation II. Urgent, emergent or salvage were included with the Em-TAVR group and elective with the El-TAVR group.
Results Em-TAVR was observed in 87 (5.4%) patients. A higher Clinical Frailty Scale (CFS), peripheral artery disease (PAD), hypoalbuminaemia, reduced left ventricular ejection fraction (LVEF) and preoperative at least moderate mitral regurgitation (MR) predicted the need for the Em-TAVR by the multivariate logistic regression analysis. The Em-TAVR group had the higher Society of Thoracic Surgeons Score (13.7 (IQR 8.2–21.0) vs 6.5 (IQR 4.6–9.2); p<0.001) and higher 30-day mortality (9.2% vs 1.3%; p<0.001) than the El-TAVR group. Accordingly, Kaplan-Meier analysis showed that the cumulative mortality was higher in the Em-TAVR group than that in the El-TAVR group (log-rank; p<0.001). However, Em-TAVR did not predict mortality in the multivariate Cox regression analysis.
Conclusions Em-TAVR was performed in 5.4% of patients. Higher CFS, PAD, hypoalbuminaemia, reduced LVEF and preprocedural MR predicted the need for Em-TAVR. Em-TAVR was not a predictor for mortality in the multivariate analysis, suggesting that it is a reasonable treatment option.
- transcatheter aortic valve replacement
- aortic valve stenosis
- heart valve prosthesis implantation
This is an open access article distributed in accordance with the Creative Commons Attribution 4.0 Unported (CC BY 4.0) license, which permits others to copy, redistribute, remix, transform and build upon this work for any purpose, provided the original work is properly cited, a link to the licence is given, and indication of whether changes were made. See: https://creativecommons.org/licenses/by/4.0/.
Statistics from Altmetric.com
Key questions
What is already known about this subject?
Previous studies suggested urgent/emergent/salvage transcatheter aortic valve replacement (Em-TAVR) as an effective treatment option in patients with severe aortic stenosis (AS) with acute decompensated heart failure. However, because the backgrounds of patients who underwent Em-TAVR differed across these studies, the effectiveness and safety of Em-TAVR have not been confirmed and predictors of need for Em-TAVR remain unclear.
What does this study add?
The percentage of patients with severe AS who needed to undergo Em-TAVR in our study was 5.4%. The predictors for the need for Em-TAVR were a high Clinical Frailty Scale, a history of peripheral artery disease, hypoalbuminaemia, reduced left ventricular ejection fraction and at least moderate mitral regurgitation. Urgency did not negatively affect the mortality after TAVR according to the multivariate analysis. This is the first report on Em-TAVR from an Asian multicentre registry.
How might this impact on clinical practice?
As the finding that Em-TAVR itself does not predict mortality, there may be no need for hesitation when deciding to perform Em-TAVR. It may be better to consider the procedure ahead of time in patients with severe AS with congestive heart failure, especially in those using catecholamines and/or mechanical circulatory support because bed rest is associated with sarcopenia, infections and a greater length of stay.
Introduction
Transcatheter aortic valve replacement (TAVR) has emerged as a safe and effective treatment option for patients with symptomatic severe aortic stenosis (AS) who are at prohibitive, high or intermediate risk for surgical aortic valve replacement (SAVR).1 Recently, the U.S. Food and Drug Administration approved an expanded indication for several transcatheter heart valves to include patients with severe AS at low surgical risk.2 3
Previous studies suggested urgent/emergent/salvage TAVR (Em-TAVR) as an effective treatment option in patients with severe AS with acute decompensated heart failure or cardiogenic shock.4–7 However, the baseline characteristics of patients who underwent emergent TAVR differed across these studies. For example, regarding a status of urgency of TAVR procedure, no ‘salvage’ status patient, ‘emergent’ with 0.2% of patients and ‘urgent’ with 9.7% were included in the study from the Society of Thoracic Surgeons (STS) and the American College of Cardiology Transcatheter Valve Therapy (ACC TVT) Registry.4 In contrast, another study only included patients with cardiogenic shock.5 Thus, the results of these previous studies should be interpreted with caution. The patients’ backgrounds and clinical outcomes in Em-TAVR have not been thoroughly studied.
The aim of this study was to investigate the predictors for the need for Em-TAVR, and the patients’ characteristics and mortality in Em-TAVR using data from a multicentre Japanese registry.
Methods
Study population and definitions
The Optimised transCathEter vAlvular interventioN TAVI (OCEAN-TAVI) registry is a Japanese multicentre prospective registry affiliated to 14 high-volume medical centres, including the Keio University School of Medicine, Teikyo University School of Medicine, New Tokyo Hospital, Kokura Memorial Hospital, Saiseikai Yokohama-City Eastern Hospital, Sendai Kosei Hospital, Shonan Kamakura General Hospital, Toyohashi Heart Center, Nagoya Heart Center, Toyama University, Tokyo bay medical centre, Osaka city university Hospital, Kishiwada tokusyu-kai Hospital and Ogaki Municipal Hospital. This trial is registered with the University Hospital Medical Information Network (UMIN; UMIN000020423). Between October 2013 and July 2016, 1613 patients with severe AS undergoing TAVR with the Edwards Sapien XT and Sapien 3 valve (Edwards Lifesciences) and the Medtronic CoreValve (Medtronic, Minneapolis, Minnesota, USA) were included in the OCEAN-TAVI registry. The inclusion criteria for this registry have been previously reported.8
Patients who admitted for a planned TAVR operation were included in the elective TAVR (El-TAVR) group. The others who required unplanned hospitalisation and TAVR during the same hospitalisation were included in the Em-TAVR group. The level of urgency was defined as urgent, emergent or salvage, based on the European System for Cardiac Operative Risk Evaluation (EuroSCORE) II risk model.9 Urgent: a status requiring unplanned hospitalisation and TAVR during the same hospital stay due to unstable symptoms, catecholamine dependency and/or a need for mechanical circulatory support (MCS), such as intra-aortic balloon pumping, extracorporeal membrane oxygenation or mechanical respiratory support. Emergent: requiring TAVR before the beginning of the next working day after the decision to operate. Salvage: requiring cardiopulmonary resuscitation (external cardiac massage) before TAVR and subsequent TAVR.
Statistical analysis
Continuous variables were assessed for normality of distribution using the Shapiro-Wilk test; those that followed a normal distribution were reported as the mean±SD, and those that did not were reported as the median and IQR. Student’s t-test was performed for intergroup comparisons of parametric data, and the Mann-Whitney U test was used for intergroup comparisons of non-parametric data. Categorical variables were reported as a number (percentage) and compared using Pearson’s χ2 test or Fisher’s exact test. A p<0.05 was considered statistically significant. Parameters for the prediction (p<0.05) of the need for Em-TAVR were entered into a multivariable logistic regression model. To determine independent predictors for all-cause mortality after TAVR, multivariate Cox proportional hazards models were used. Cumulative mortality was estimated by the Kaplan-Meier method, and differences were assessed with the log-rank test. JMP V.14 for Mac (SAS Institute) was used for all statistical analyses.
Results
Baseline characteristics and echocardiographic variables
Of the 1613 patients in our study, 87 (5.4%) patients underwent Em-TAVR (70 (4.3%) urgent, 15 (0.9%) emergent and 2 (0.1%) salvage) due to decompensated heart failure. The remaining 1526 patients (94.6%) underwent El-TAVR. The median follow-up time was 250 (IQR 99–447) days. The baseline patient characteristics, laboratory data and echocardiography data are listed in table 1. The mean age was 84.4±5.1 years and 70.4% were female in the all TAVR patients. The Em-TAVR patients had the higher Surgical Risk Scores compared with the El-TAVR patients (STS Score: 13.7 (IQR 8.2–21.0) vs 6.5 (IQR 4.6–9.2); p<0.001 and EuroSCORE II: 11.0 (IQR 4.6–19.2) vs 3.6 (IQR 2.3–5.6); p<0.001). Regarding preoperative echocardiographic findings, Em-TAVR patients had a lower left ventricular ejection fraction (LVEF) than El-TAVR patients (47.9%±16.1% vs 58.5%±11.9%, p<0.001). Compared with El-TAVR patients, Em-TAVR patients had a higher prevalence of at least moderate mitral regurgitation (MR) (27.6% vs 9.0%, p<0.001) and at least moderate tricuspid regurgitation (TR) (14.9% vs 6.0%, p=0.004). Contrast-enhanced CT was performed for all patients in this study.
Baseline patient characteristics of the study population
Procedural characteristics and in-hospital outcomes
The procedural characteristics and clinical outcomes are presented in table 2. The 30-day mortality in Em-TAVR patients was higher than in El-TAVR patients (9.2% vs 1.3%, p<0.001). Acute device success, according to the Valve Academic Research Consortium 2 definition,10 was achieved in 76 (87.4%) Em-TAVR patients and in 1440 (94.4%) El-TAVR patients. Among the patients in our study, the Clinical Frailty Scale (CFS) score (OR 1.50, 95% CI 1.24 to 1.83, p<0.001), peripheral artery disease (PAD; OR 2.34, 95% CI 1.32 to 4.13, p=0.003), serum albumin concentration <3.5 g/dL (OR 2.15, 95% CI 1.25 to 3.68, p=0.006), LVEF (OR 0.96, 95% CI 0.94 to 0.97, p<0.001) and preoperative moderate or severe MR (OR 2.60, 95% CI 1.42 to 4.74, p=0.002) were identified by the multivariate logistic regression analysis as predictors for the need for Em-TAVR (table 3). According to the multivariate Cox regression analysis, TAVR urgency was not associated with mortality after TAVR (online supplemental table 1).
Supplemental material
Procedural characteristics and in-hospital outcomes in transcatheter aortic valve replacement
The multivariate logistic regression analysis for predictors for the need for urgent/emergent/salvage transcatheter aortic valve replacement
Cumulative survival rate of the urgency of TAVR
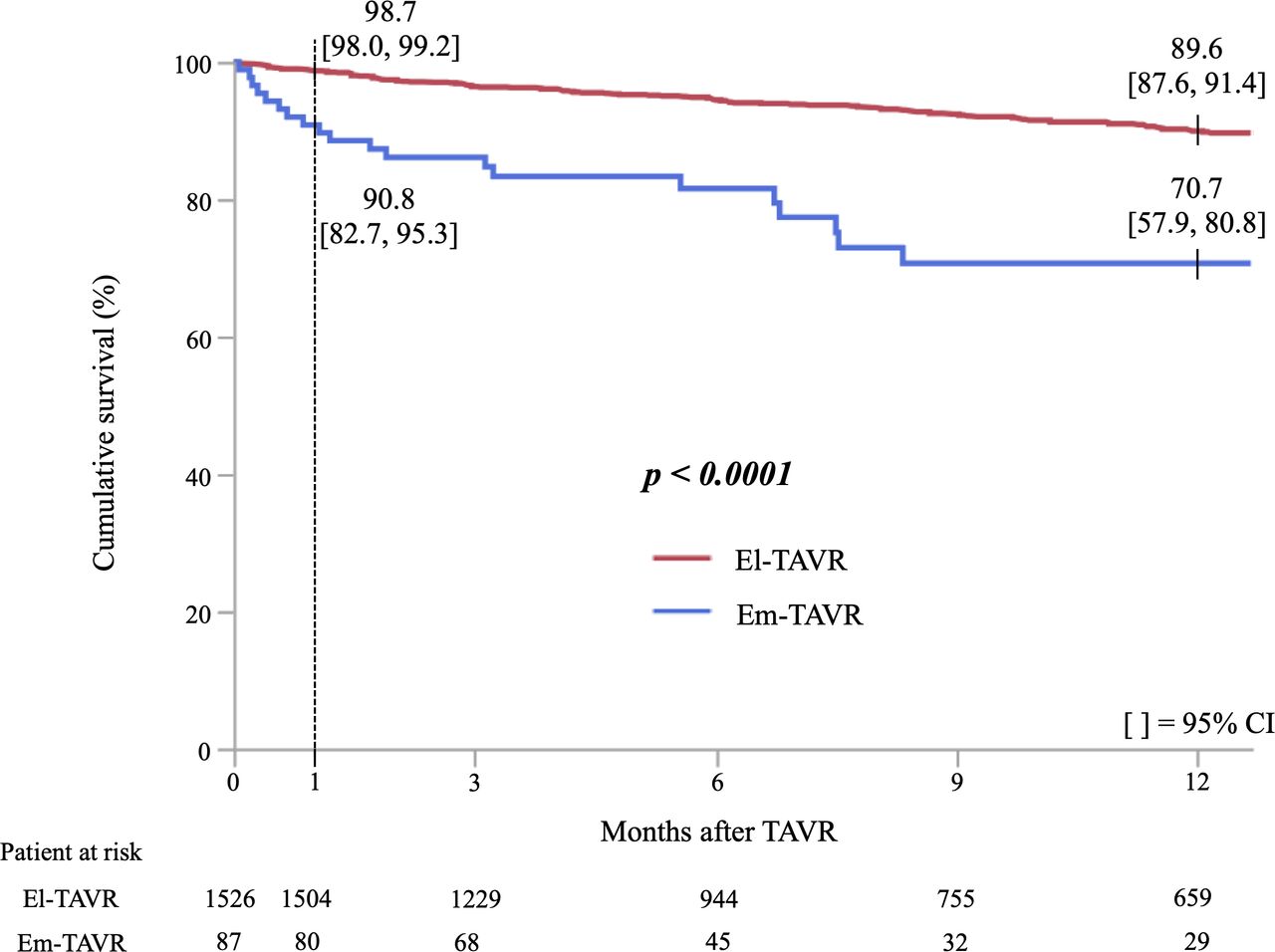
The cumulative survival rate in Kaplan-Meier analysis was significantly lower in Em-TAVR patients compared with El-TAVR patients (log-rank test; p<0.001) (figures 1 and 2). There was a significant difference in the cumulative survival rate between El-TAVR and urgent TAVR patients (log-rank test; p<0.001) (online supplemental figure 1). However, the cumulative survival did not differ between urgent and emergent/salvage TAVR patients (log-rank test; p=0.996) (online supplemental figure 2).
Supplemental material
Supplemental material
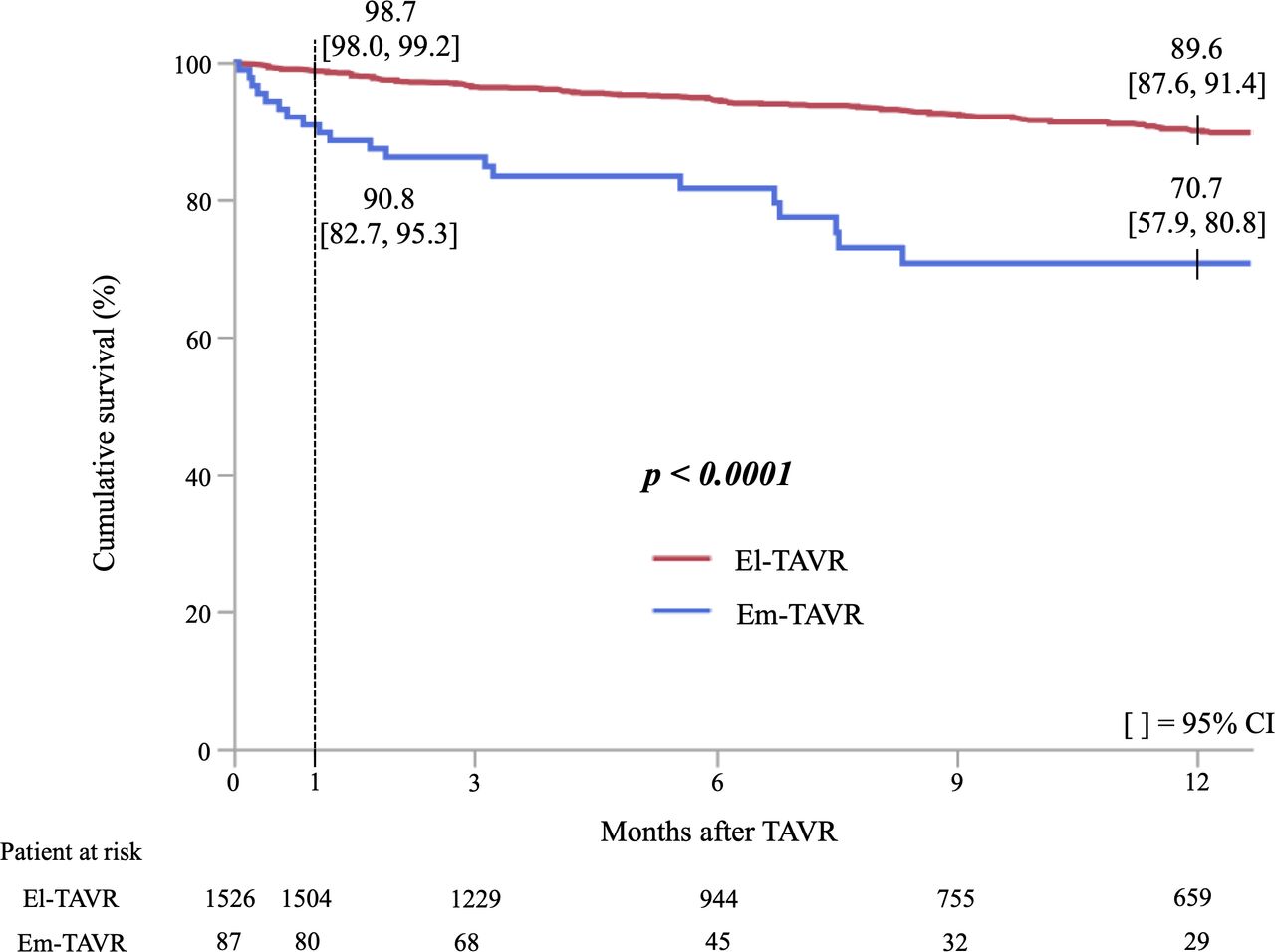
Cumulative survival curves according to urgency of transcatheter aortic valve replacement (TAVR). El-TAVR=elective TAVR; Em-TAVR=urgent/emergent/salvage TAVR.

{kind=link}
{kind=link}
Cumulative survival curves according to urgency of transcatheter aortic valve replacement (TAVR). El-TAVR=elective TAVR.
Subgroup analysis in the Em-TAVR patient cohort
We performed a subgroup analysis to investigate variables associated with 1-year mortality in Em-TAVR patients. The Em-TAVR patients were divided into two groups based on whether or not they had survived for 1 year after TAVR; 20/87 (23.0%) had died with 1 year of TAVR. The baseline patient characteristics of these patients are presented in online supplemental table 2). Compared with the survivor group, the CFS Score was higher (5.6±1.4 vs 4.8±1.2; p=0.016) and haemoglobin level (9.6±1.6 g/dL vs 11.1±1.8 g/dL, p=0.002) was lower in the mortality group. The prevalence of prior coronary artery bypass graft (CABG) (25.0% vs 6.0%; p=0.024) and prior stroke (40.0% vs 17.9%; p=0.048) in the mortality group was higher than in the survivor group. The procedural characteristics, clinical outcomes and procedural complications among the two groups are presented in online supplemental table 3. Seventeen patients in the mortality group underwent postoperative echocardiography. The prevalence of at least moderate aortic regurgitation (11.8% vs 0.0%; p=0.010) and at least moderate TR (29.4% vs 9.0%; p=0.026) was higher in the mortality group than in the survivor group. In the univariate logistic regression analysis, a higher CFS (OR 1.50, 95% CI 1.06 to 2.14, p=0.023), prior CABG (OR 3.18, 95% CI 1.15 to 8.77, p=0.026), lower serum haemoglobin concentration (OR 0.71, 95% CI 0.54 to 0.91, p=0.010) and lower serum albumin concentration (OR 0.91, 95% CI 0.85 to 0.98, p=0.014) were significantly associated with an increased risk of 1-year mortality after Em-TAVR (online supplemental table 4).
Discussion
We made three important clinical observations in this study. First, the percentage of patients with severe AS who needed to undergo Em-TAVR in our study was 5.4% (87/1613). Second, the predictors for the need for Em-TAVR were a high CFS, a history of PAD, hypoalbuminaemia, reduced LVEF and at least moderate MR. Although Kaplan-Meier analysis revealed that cumulative mortality was higher in Em-TAVR patients than in El-TAVR patients, the Cox regression analysis revealed that Em-TAVR was not associated with cumulative mortality after TAVR. To the best of our knowledge, this is the first report on Em-TAVR from an Asian multicentre registry.
The authors summarised the principal findings on Em-TAVR obtained from this study, the study from the STS/ACC TVT Registry4 and the study by Frerker et al,5 detailing the patients’ characteristics, the prevalence of Em-TAVR, the acute device success rate of the TAVR procedure and the mortality rate in online supplemental table 5. Compared with the study from the STS/ACC TVT Registry, our study included patients with a higher Surgical Risk Score and showed similar mortality rates after Em-TAVR.4 As expected, the baseline conditions of patients with Em-TAVR were significantly worse than those with El-TAVR in our study. Although the cumulative mortality after Em-TAVR was higher than after El-TAVR, the clinical outcomes in Em-TAVR seemed to be acceptable in our study. Further, urgency did not negatively affect the mortality after TAVR (online supplemental table 1). Considering these findings, we believe that there is no need for hesitation when deciding to perform Em-TAVR. Prolonged hospitalisation due to observation treatment is inherently harmful to older patients because bed rest is associated with sarcopenia, infections and a greater length of stay.11 However, early mobilisation due to early intervention may result in a reduced length of stay and reduce the complications associated with bed rest. Thus, it may be better to plan the procedure ahead of time for patients with severe AS with congestive heart failure, especially in those using catecholamines and/or MCS. Although balloon aortic valvuloplasty (BAV) can be another treatment option in an emergent setting, Bongiovanni et al showed that El-TAVR following to emergent BAV was not superior to Em-TAVR without emergent BAV in terms of survival.6 BAV may be considered when TAVR is inappropriate due to anatomical problems.
This study showed that the predictors for the need for Em-TAVR were higher CFS, a history of PAD, hypoalbuminaemia, reduced LVEF and at least moderate preoperative MR (table 3). Although previous studies have shown that these factors are predictors of mortality after TAVR,12–20 it was unknown whether they were also the predictors for the need for Em-TAVR. CFS, hypoalbuminaemia and PAD have been accepted as a general indicators of a patient’s vulnerability and are highly associated with adverse health outcomes in the geriatric field.21–24 Our study showed that preoperative moderate or severe MR was associated with Em-TAVR. In both SAVR and TAVR, previous studies have shown a higher mortality following TAVR in patients with significant MR than in those without.17–20 Moreover, higher CFS, prior CABG, lower serum haemoglobin concentration and lower serum albumin concentration were associated with 1-year mortality after Em-TAVR (online supplemental table 4). The CFS, serum haemoglobin concentration and serum albumin concentration in our study were associated with the need for Em-TAVR and 1-year mortality after Em-TAVR. High CFS and low haemoglobin and albumin concentration level, together with, reduced LVEF or significant MR, could be signs encouraging clinicians to conduct TAVR earlier.
Regarding study limitations, a selection bias may exist in our study because the decision regarding the performance of Em-TAVR was at the discretion of the local heart team and the details of the reason for Em-TAVR were unknown. Due to the small number of the patients who underwent Em-TAVR, we could not perform multivariate analysis to identify independent predictors for 1-year mortality after Em-TAVR.
Conclusion
Em-TAVR was observed in 5.4% of patients in this study. The predictors for the need for Em-TAVR were identified as a higher CFS, PAD, hypoalbuminaemia, reduced LVEF and at least moderate MR. The multivariate Cox regression analysis revealed that Em-TAVR was not associated with cumulative mortality after TAVR, suggesting that Em-TAVR is a safe and reasonable treatment option.
Acknowledgments
The authors thank all the OCEAN-TAVI investigators.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors Study conception, design, analysis and interpretation, drafting of the manuscript: YE, MM and NT. Critical revision of the manuscript for important intellectual content: MT, MH, YW, TN, MY, SS, HU, KM, MT, KT, MY and KH. Overall responsible: YE.
Funding The OCEAN-TAVI registry is supported by Edwards Lifesciences, Medtronic, and Daiichi-Sankyo company.
Competing interests NT, MY, TN, SS, KM, HU, YW, and MT are clinical proctors for Edwards Lifesciences and Medtronic. KT and KH are clinical proctors of Edwards Lifesciences.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement The data in this research are deidentified participant data. The data and materials will not be available to researchers for purpose of reproducing the results or replicating the procedure.