Article Text

Abstract
Background Recent randomised clinical trials have suggested prognostic benefits of catheter ablation in highly selected patients with atrial fibrillation (AF) and heart failure (HF).
Objectives This study sought to identify the treatment effect associated with catheter ablation in a broad population of patients with AF and HF.
Methods Through nationwide administrative registers in Denmark, we estimated the 2-year average treatment effect (ATE) of catheter ablation for AF on a composite endpoint of HF readmission, stroke and all-cause mortality at 1-year and 5-year landmark analyses. The primary cohort was patients with AF before HF, and the second cohort of patients with HF before AF.
Results A total of 13 756 patients were included with 9904 patients in the primary cohort, and 3852 in the secondary. An ATE (95% CI) reduction of the composite endpoint of 7.0% (4.5% to 9.5%) was observed in the primary cohort and 11.8% (6.0% to 17.6%) in the secondary in the 1-year landmark analysis with a reduction in all-cause mortality of 5.8% (3.7%–7.8%) and 6.3% (0.9%–11.7%), respectively. At the 5-year landmark, catheter ablation was associated with reductions in the composite endpoint and all-cause mortality in the primary (4.7% (2.3% to 7.2%), and 3.6% (1.0% to 6.3%), respectively), but not in the secondary cohort.
Conclusions Ablation was associated with decreased risk of HF readmission, stroke and all-cause mortality in patients with AF and HF. The effect is most substantial in patients with AF before HF and with catheter ablation after 1 year from the diagnosis of both conditions.
- atrial fibrillation
- radiofrequency ablation
- stroke
- heart failure
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known about this subject?
Recent studies have shown a possible decreased risk of death with radiofrequency ablation in patients with atrial fibrillation and heart failure. Atrial fibrillation can lead to tachycardia-induced heart failure, but also heart failure increases the risk of developing atrial fibrillation.
What does this study add?
Our study shows a decreased risk of readmission with heart failure, stroke and all-cause mortality with radiofrequency ablation in both patients with atrial fibrillation before heart failure and in patients with heart failure before atrial fibrillation. This reduction was most prominent in patients with tachycardia-induced heart failure.
How might this impact on clinical practice?
Radiofrequency ablation should not only be seen as symptom-relieving but also as a potential mortality-reducing procedure in patients with atrial fibrillation and heart failure.
Introduction
Pharmacological treatment of atrial fibrillation (AF) in patients with concomitant heart failure (HF) poses a challenge in daily clinical practice.1 Medical therapy remains the first choice in the management of AF, but modest efficacy, adverse effects and contraindications are significant limitations to this strategy.2 Catheter ablation to restore sinus rhythm is, therefore, an intriguing additional treatment option, especially in patients with a tachyarrhythmia-induced cardiomyopathy.3 Small studies have suggested that catheter ablation may improve left ventricular function and functional capacity in patients with AF and HF,4–7 and recently randomised controlled trials reported that catheter ablation might reduce the risk of admission for HF and mortality.8 9
Considering the neutral result of the AF-CHF trial (Rhythm Control vs Rate Control for AF and HF), the mortality benefit observed in the CASTLE-AF trial (Catheter Ablation vs Standard Conventional Treatment in Patients with Left Ventricular Dysfunction and Atrial Fibrillation) was somewhat surprising.10 It has been hypothesised that small study size in CASTLE-AF (ie, type I error), lack of balancing of baseline variables, an uneven number of patients lost to follow-up, as well as bias due to an inherent open study design may explain the results.11 Finally, it is unclear how the results from too slow recruiting trials evaluating treatment effect in typical conditions (20%–40% of all patients with HF have AF) should be translated into clinical practice. For these reasons, patient selection for catheter ablation remains unclear in patients with AF and concomitant HF.
The present study sought to evaluate the real-life association between AF catheter ablation and a composite endpoint of stroke, admission for HF or all-cause mortality in a nationwide cohort of patients with AF and HF ≤75 years and all treated with oral anticoagulation. Analyses were done separately for patients with pre-existing AF before HF diagnosis and those with AF after HF diagnosis. The rationale for the two separate cohorts was the preconceived notion that patients with AF before HF would have tachyarrhythmia-induced HF and, therefore, more significant benefit from catheter ablation than patients with HF before AF, where structural myocardial heart disease and increased left ventricular filling pressures more likely would be the pathogenesis for AF.
Methods
Data sources
In this register-based cohort study, information on demographics, comorbidities, procedures, concomitant medication, and outcome variables were identified using three different nationwide Danish registers. These registers were cross-linked using the unique personal identification number given to all Danish citizens at the date of birth or date of migration to Denmark. The Civil Registration System holds data on age, sex and vital status of patients, where all deaths are registered within 14 days of occurrence. The Danish National Patient Register contains information on every hospital admission in Denmark since 1978, in which each hospitalisation is registered at discharge with one primary diagnosis and, if applicable, one or more secondary diagnoses according to the International Classification of Diseases; the 10th revision (ICD-10), since 1994. The Danish National Patient Register also holds information on operations and procedures, including catheter ablation. These procedures have been registered since 1996 and coded according to the Nordic Classification of Surgical Procedures (NCSP) by The Nordic Medico-Statistical Committee. Data on the date, quantity, strength, formulation and affiliation of the prescribing physician, all prescriptions dispensed from Danish pharmacies have been accurately registered in The Danish Registry of Medicinal Product Statistics since 1995 and coded according to the Anatomical Therapeutic Chemical classification system.
Prevalent AF was identified using ICD-10 code ‘I48’ in both inpatients and outpatients. Patients with HF were identified based on our hospital outpatient clinic discharge diagnostic codes. Prevalent HF was identified using the ICD-10 code ‘I50’, ‘I11.0’, ‘I13.0’ or ‘I13.2’, also in both inpatients and outpatients.12 13 Catheter ablation procedures for AF were identified using the NCSP procedure code ‘BFFB04’ for AF catheter ablation (online supplemental table 1).
Supplemental material
Study cohort
Patients were included between 2005 and 2017, age ranged between 18 and 75 years, no history of prior catheter ablation, or ischaemic stroke and were all treated with oral anticoagulants. The age and anticoagulation criteria were used to include a study population more likely to be referred to an AF catheter ablation. The analyses were done separately in two cohorts: the primary cohort contained patients who were diagnosed with AF before or the same day as HF, and the secondary cohort included patients with HF before AF.
Patients in the primary cohort were followed from the date of HF diagnosis, and for the secondary cohort date of AF diagnosis. This date is referred to as index date in the two cohorts, respectively.
Study endpoint
The primary endpoint was a composite of HF readmission, stroke and all-cause mortality, and secondary endpoints were the endpoints separately.
Patient and public involvement statement
The patients and public were not involved in the creation of the study design or statistical analysis. Patients were not consulted to develop patient-relevant outcomes or interpret the results. Patients were not invited to contribute to the writing or editing of this document for readability or accuracy.
Statistics
All analyses were performed separately, starting from two landmark time points set at 1 year and 5 years after study inclusion, respectively. Patients were included if they were alive and without events at landmark. The two landmark analyses were performed at 1 and 5 years in order to investigate whether potential benefits of catheter ablation would be present in both patients with long and short duration of AF and HF prior to the procedure. Patients were then subdivided according to whether they had received catheter ablation in the time between the index date and the landmark date. Patients who had an event included in the primary composite endpoint between the date of HF diagnosis and landmark date were excluded from the analyses, in order to avoid immortal time bias.
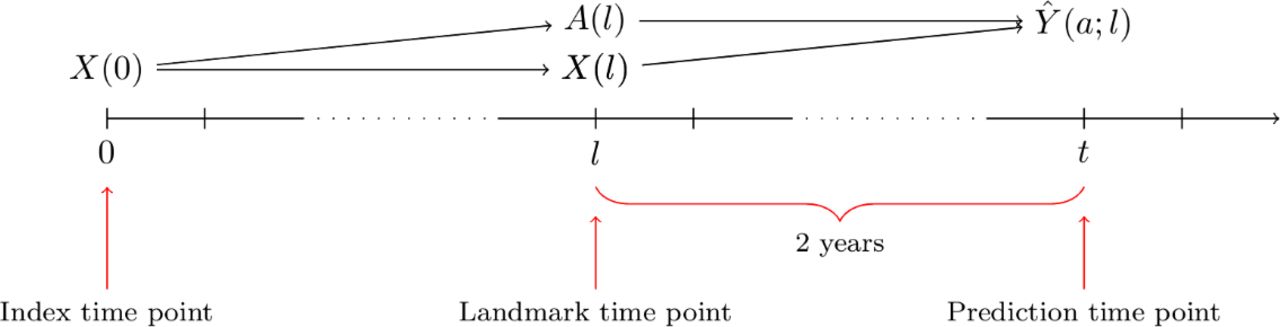
Patients were followed from the landmark time point until the composite endpoint, date of emigration or 1 January 2017, whatever came first (figure 1). The absolute personalised risks of the composite endpoint within the first 2 years after the landmark time point were estimated using Cox regression adjusted for patient characteristics evaluated at the landmark time point: catheter ablation status (yes/no) and the predictor variables of chronic obstructive pulmonary disease (COPD), chronic kidney disease (CKD), ischaemic heart disease (IHD), diabetes mellitus (DM), hypertension, outpatient HF diagnosis (yes/no), age and sex.
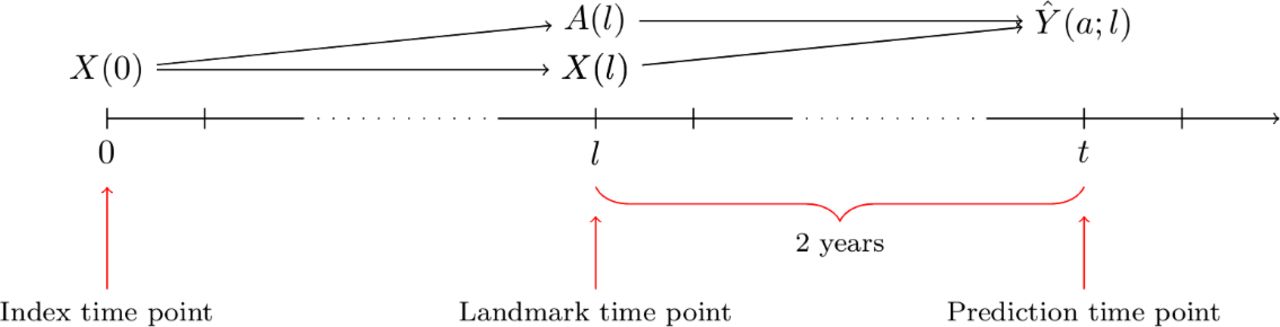
Flowchart of the landmark analyses. Patients were then followed from the landmark time point until the composite endpoint, date of emigration or 1 January 2017 whatever came first.
Average treatment effects (ATEs) were defined as differences between the standardised absolute risks of the combined endpoint occurring within 2 years after the landmark time.14 Analyses were repeated with all-cause mortality as an outcome instead of the composite endpoint. For the two outcomes readmission with HF and stroke, death without readmission for HF (without stroke) is a competing risk. We used the cause-specific Cox regression approach of Benichou and Gail15 to estimate the absolute personalised risks of HF readmission, respectively, admission with stroke, within 2 years after the landmark date (online supplemental figure 1).
Supplemental material
Categorical data were presented as counts with percentages, and the statistical difference was tested using χ2 tests. Continuous variables were presented as medians with IQRs, and the statistical difference was tested using Wilcoxon rank-sum tests. Logistic regression (propensity score model) was used to associate patient characteristics evaluated at the index date with the odds of receiving catheter ablation within the landmark date. Data management and statistical analyses were conducted using R statistics.16 A p value <0.05 and a 95% CI not containing 1 was considered significant.
Results
The total number of patients included in the study were 13 756 with 9904 (72%) in the primary cohort and 3852 (28%) in the secondary cohort. Of the 9904 patients in the primary cohort (AF before HF), 3677 (37.1%) were diagnosed with AF and HF on the same day
(figure 2). At baseline, the median (IQR) age was 67 (61–71) years, and 74.2% were men with no difference found between the two cohorts, but significantly more comorbidities were observed in the second cohort (table 1).
Baseline characteristics at index date
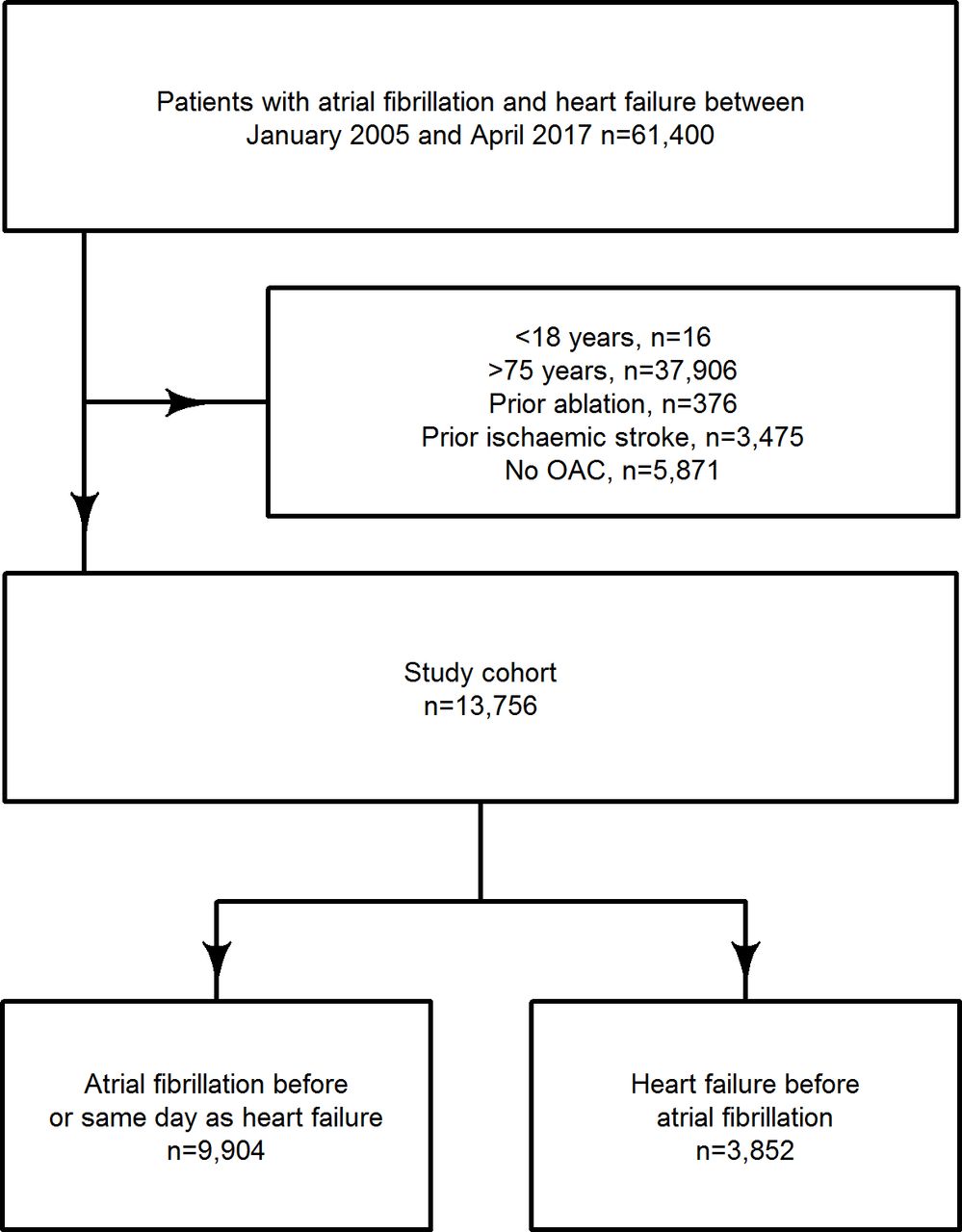
Flowchart of the study cohort selection. OAC, oral anticoagulation.
After 1 year, 259 (3.1%) and 50 (1.6%) patients had received a catheter ablation in the primary and secondary cohort, respectively. The total number of catheter ablations performed in the study period was 749 (5.4%), with 627 (6.3%) in the primary cohort and 122 (3.2%) in the secondary. Higher age, COPD, IHD, DM all significantly decreased the likelihood of a catheter ablation (table 2 and figure 3).
Patients eligible for 1-year landmark analysis

Propensity of predictor variables towards catheter ablation. AF, atrial fibrillation; COPD, chronic obstructive pulmonary disease; CKD, chronic kidney disease; DM, diabetes mellitus; HF, heart failure; HT, hypertension; IHD, ischaemic heart disease.
The absolute risk difference as defined by the ATE (95% CI) in patients who received catheter ablation compared with those who did not after 1 year was 7.0% (4.5%–9.5%) in the primary cohort and 11.8% (6.0%–17.6%) in the secondary cohort regarding the composite endpoint. The composite endpoint was mainly driven by all-cause mortality and readmission with HF in both cohorts. The ATE (95% CI) of all-cause mortality after 1 year was 5.8% (3.7%–7.8%) and 6.3% (0.9%–11.7%) for the primary cohort and secondary cohort, respectively.
After 5 years, 286 (7.1%) and 42 (3.3%) of the eligible patients had received catheter ablation in the primary and secondary cohort, respectively, with the same selection towards younger age and fewer comorbidities, as seen in the 1-year landmark analyses (table 3).
Patients eligible for 5-year landmark analysis
The ATE (95% CI) of catheter ablation on the composite endpoint was still significant, with 4.7% (2.3%–7.2%) in the primary cohort with an ATE (95% CI) of catheter ablation on all-cause mortality of 3.6% (1.0%—6.3%). Still, in the second cohort, a significant ATE was no longer observed 2.8% (−7.8% to 13.2%, figure 4).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Central illustration. ATE of catheter ablation on endpoints. In the 1-year analyses, 259 (3.1%) and 50 (1.6%) had an ablation in the primary and secondary cohort, respectively, this was 286 (7.1%) and 42 (3.3%) in the 5-year analyses. AF, atrial fibrillation; ATE, average treatment effect; HF, heart failure.
Discussion
Main findings
In this nationwide study, we found a significant association between AF catheter ablation and a reduced risk of the composite endpoint of HF readmission, stroke and all-cause mortality. Five years after the index date, the effect of was attenuated, and AF catheter ablation was no longer associated with a reduced risk of HF readmission or stroke.
Real-life effect versus the clinical trial effect of catheter ablation in HF
In the CASTLE-AF trial, a 16.1% (28.5% vs 44.6%, p value=0.007) absolute risk reduction of death from any cause or hospitalisation for worsening HF was found with catheter ablation versus medical therapy after a median follow-up of 3 years.9 In our real-life study, we observed an estimated ATE of 7.0% after 2 years follow-up and 4.7% after 5 years in the primary cohort and 11.8% and 2.8% (non-significant) in the secondary cohort. Several factors may explain this discrepancy. Stroke was not included as an endpoint in the in CASTLE-AF study. The median age in CASTLE-AF was 64 years compared with 70 in our study, 86% were men compared with 74% in our cohort, and the number of patients with IHD was 46% in CASTLE-AF compared with 37% in our study. We included patients with HF with both preserved and reduced left ventricular ejection fraction and patients without an implantable cardioverter-defibrillator (ICD). In the CASTLE-AF study, only patients with HFrEF (HF with reduced ejection fraction) and ICD were included.
In the CABANA trial, the primary endpoint was a composite of death, disabling stroke, severe bleeding or cardiac arrest. In the intention-to-treat analysis of the subgroup with congestive HF (15% of the total cohort), a non-significant 5.7% reduction of the primary endpoint occurred in the catheter ablation group (12.1% vs 17.8%, p value=NS) versus the medical therapy group over a median follow-up of 4 years.17 The findings in the CABANA trial are closer to the conclusions of our observational study, although we found a significant difference between the two groups. The median age in the trial was 68 years, with 62.8% men, so again the population differed in the study population with older and more men than in our study. These discrepant findings between the CABANA trial and our study could, therefore, be explained by both differences in cohort selection and difference in definition of endpoints.
Comorbidities and likelihood of catheter ablation in HF
Based on data from our administrative registries, we identified clinical variables associated with the probability of undergoing catheter ablation. Being a younger male without comorbidities with a previous admission for HF seems to be the phenotype that is most likely to receive this treatment in Denmark. Except for having HF diagnosed in-hospital, all variables associated with being ablated were also associated with a better outcome. This should be kept in mind when interpreting our analyses since confounding by indication can never be eliminated in an observational study. In theory, the real-life effect of catheter ablation maybe even smaller.
Methodological considerations
The strength of the present study is the inclusion of >10.000 consecutive patients ≤75 years of age, all treated with anticoagulation without anyone lost to follow-up during a long period. The rationale for the exclusion of patients >75 years was avoiding controls with a low likelihood of being offered AF catheter ablation.18 Investigating the two phenotypically different patient types AF before HF and HF before AF also contributes with new information regarding benefits of catheter ablation, since no significant difference in ATE was found between the two groups; hence our hypothesis regarding the larger benefit of catheter ablation in the AF before HF groups was not supported by the data. A high specificity of the used diagnostic codes in our registry and vital status on all patients are also strengths.12
Limitations
The present study is based on administrative codes and misclassification of HF and AF can, therefore, not be fully excluded. Further, important echocardiographic and clinical variables used for referral of patients with HF to AF ablation is neither available, and we were not able to differentiate between patients with HF and reduced versus preserved ejection fraction. Our results should be evaluated with that in mind. Unmeasured confounding due to lack of information on important clinical variables such as functional class, NT-proBNP and left ventricular ejection fraction—and residual confounding—for example, renal function is estimated based on a diagnostic code for CKD—cannot be excluded in our study. Information about the burden of AF after catheter ablation is also lacking, and if AF was paroxysmal, persistent, long-time persistent or permanent was unknown. We have no information on catheter ablation procedure details, reason for referral, nor on how they have changed over time at different centres. Finally, our study is observational, and our findings are associations and not necessarily due to causality. However, considering all the mentioned strengths of our study, the observed treatment effect size is biologically plausible. It may give a realistic real-life estimate of the effect of AF catheter ablation in HF.
Conclusions
Catheter ablation in patients with AF and HF was associated with reduced risk of a composite endpoint of HF readmission, stroke and all-cause mortality. This was true in both patients with AF before HF and HF before AF at 1 year after index date, respectively. Clinical outcome trials are needed to explore if these findings are causal.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @jannik @CopCard @Pallisgaard_MD
Contributors JLP and MS helped in planning, conduction, reporting and were guarantors of the study. TAG and AM helped in planning and conduction. Reviewing was done by MLH, A-MS, AJ, FG, GHG, CT-P, PKJ, SLK and LK.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests FG is an advisor for Abbott, Carmat; Corvia (unpaid) speaker: Novartis, Astra, Orion Pharma; and investigator for Alnylam.
Patient consent for publication Not required.
Ethics approval In Denmark, retrospective register studies do not require approval from the ethics committees. The Danish Data Protection Agency approved this study (ref. no.: 2007-58-0015/GEH-2014-016 I-Suite no.: 02734), and data were made available in an anonymised format such that specific individuals could not be identified.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data may be obtained from a third party and are not publicly available.