Article Text

Abstract
With rising focus on interventional treatment of the tricuspid valve (TV), the need for good echocardiographic imaging increases. Aim of this study was to develop a scoring system describing how accurate three dimensional (3D) echocardiographic imaging of TV and its anatomical structures is.
Methods and results In this retrospective exploratory cohort study, we analysed data from consecutive patients undergoing transoesophageal echocardiography (TOE) and transthoracic echocardiography (TTE). 3D sequences were stored using eight different views. In each view, scoring focused on visualisation of five (in TOE 6) anatomical structures with a maximum of three points per structure for excellent imaging quality. We compared the scores of patients with and without relevant tricuspid regurgitation (TR) (cut-off effective regurgitant orifice 0.4 cm² measured in two-dimensional (2D) TTE using velocity time integral and proximal isovolumetric velocity area). 108 consecutive patients were examined, 40.7% presented with relevant TR. With the exception of coaptation, a higher score was achieved for all structures in TOE than in TTE. TV ring (TVR) was easiest to visualise with TOE in four-chamber view (4 CV) (2.42±0.67 points) presenting the highest score independent of anatomical structure and view. Posterior leaflet had best imaging scores in TOE in 4 CV (2.0±0.86) compared with TTE in 4 CV (1.64±0.80), p=0.001. Patients with relevant TR had significantly better 3D imaging scores in 4 CV compared with patients without relevant TR (TTE p<0.013, TOE p<0.002).
Conclusion 4 CV delivers the most detailed information in TTE, whereas multiple views deliver good scores in TOE. As TVR is easiest to visualise, most of the patients would be suitable for a ring-based echocardiography-guided intervention. The score enables a standardised comparison of image quality.
- echocardiography
- tricuspid valve disease
- three dimensional
- transoesophageal
- transthoracic
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known about this subject?
Up to now, there is no possibility to measure the echo quality especially in relation to the tricuspid valve and three-dimensional (3D) quality in echocardiographic imaging. However, the need for good 3D imaging is enormous regarding the increasing catheter-based and echoguided interventions on the tricuspid valve.
What does this study add?
This study presents a score that could be a tool to solve this problem. It identifies the anatomical structures that are most easily displayed in 3D echocardiography and which views provide the best 3D images. It brings objectivity to the subjective domain of echocardiography.
How might this impact on clinical practice?
The consistent application of the score enables a structural screening of patients with tricuspid valve insufficiency in preparation for a catheter-based intervention. It also makes echo quality measurable and comparable.
Introduction
Severe tricuspid regurgitation (TR) is known to be associated with increased morbidity, reduced functional capacity and is also considered an independent risk factor for mortality.1–3
The prevalence of severe TR in hospitalised patients is approximately 10.3% and up to 30% in case of relevant mitral regurgitation.4 5
For inoperable patients, various interventional therapeutic concepts have been developed in recent years to treat the tricuspid valve (TV). These require optimal echocardiographic visualisation of the TV and its individual anatomical structures.6 When planning a percutaneous echoguided intervention, it must be decided whether image quality is sufficient.
In contrast to two-dimensional (2D) echocardiography, three-dimensional (3D) imaging offers advantages in visualisation of the TV, especially when evaluating leaflets, TV ring (TVR) and Koch triangle.7 8 Visualisation of Koch triangle is crucial to avoid its puncture during an intervention.
Currently, there is no definition or score assessment whether visualisation is accurate enough for an interventional procedure. Therefore, we assessed which echocardiographic view offers the best imaging quality for single anatomical structures, which leaflet may easiest be visualised and whether 3D transthoracic echocardiography (TTE) may be superior to 3D transoesophageal echocardiography (TOE).
Aim of this study was to create a score for assessing the 3D echocardiographic imaging quality of the TV and its anatomical structures helping to decide whether interventional echoguided treatment is possible.
Methods
In this retroprospective exploratory cohort study, we analysed data from 108 consecutive patients undergoing TOE and TTE as enrolement criteria.
Patients with very bad 2D imaging in TTE, with atrial fibrillation and a heart rate above 120/min, were excluded (online supplementary figure). We stored four 3D live views, each from a transthoracic and transoesophageal approach. The study was conducted in accordance with the provisions of the Helsinki Declaration. All data relevant to the study are included in the article or uploaded as online supplementary figure.
Supplemental material
Score description
Transthoracic score for 3D imaging
By using a three point system, following anatomical structures were scored: TVR, septal leaflet (SL), posterior leaflet (PL) and anterior leaflet (AL), coaptation of the leaflets. The following criteria were used for scoring (figures 1A and 2A):
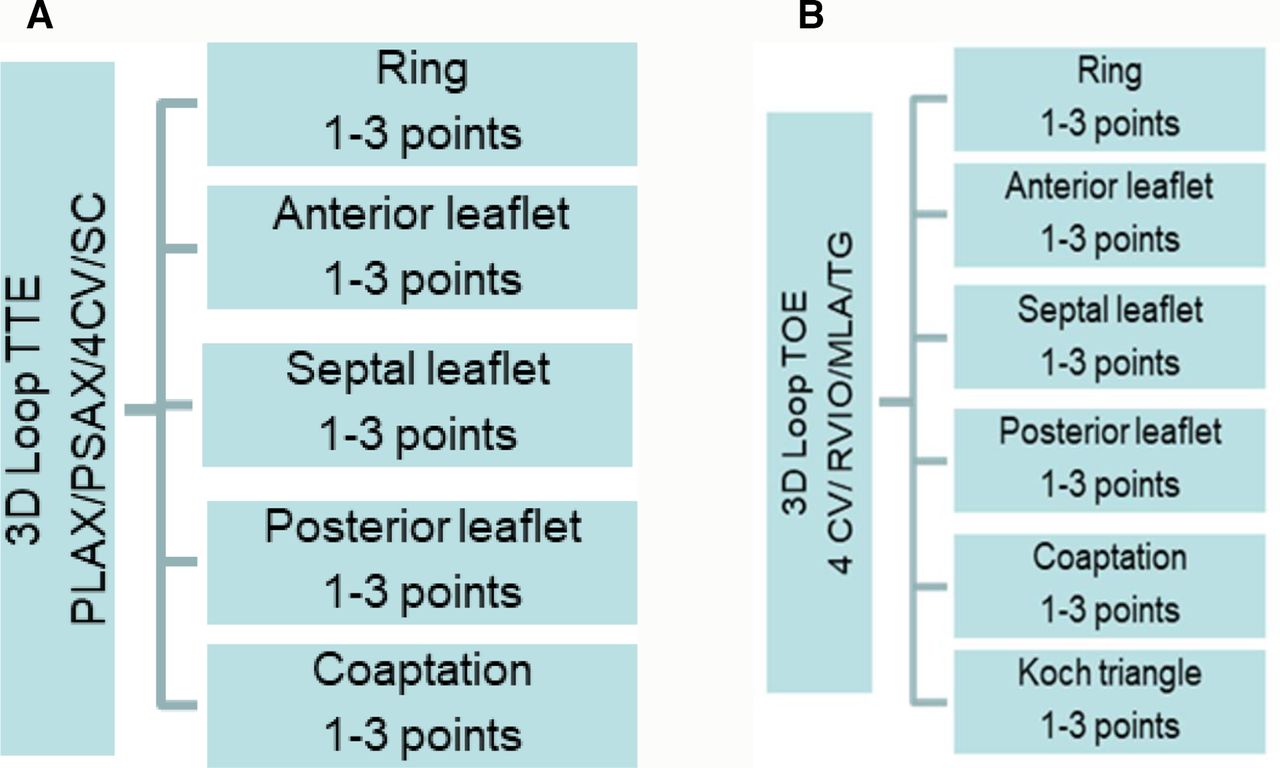
Score description in (A) TTE and (B) TOEE. 4 CV, four chamber view; 3D, three dimension; MLA, modified long axis; PLAX, parasternal long axis; PSAX, parasternal short axis; RVIO, right ventricular inflow and outflow; SCV, subcostal view; TG, transgastric view; TOE, transoesophageal echocardiography; TTE, transthoracic echocardiography.

(A) Transthoracic score for three-dimensional (3D) imaging and (B) transoesophageal score for 3D imaging.
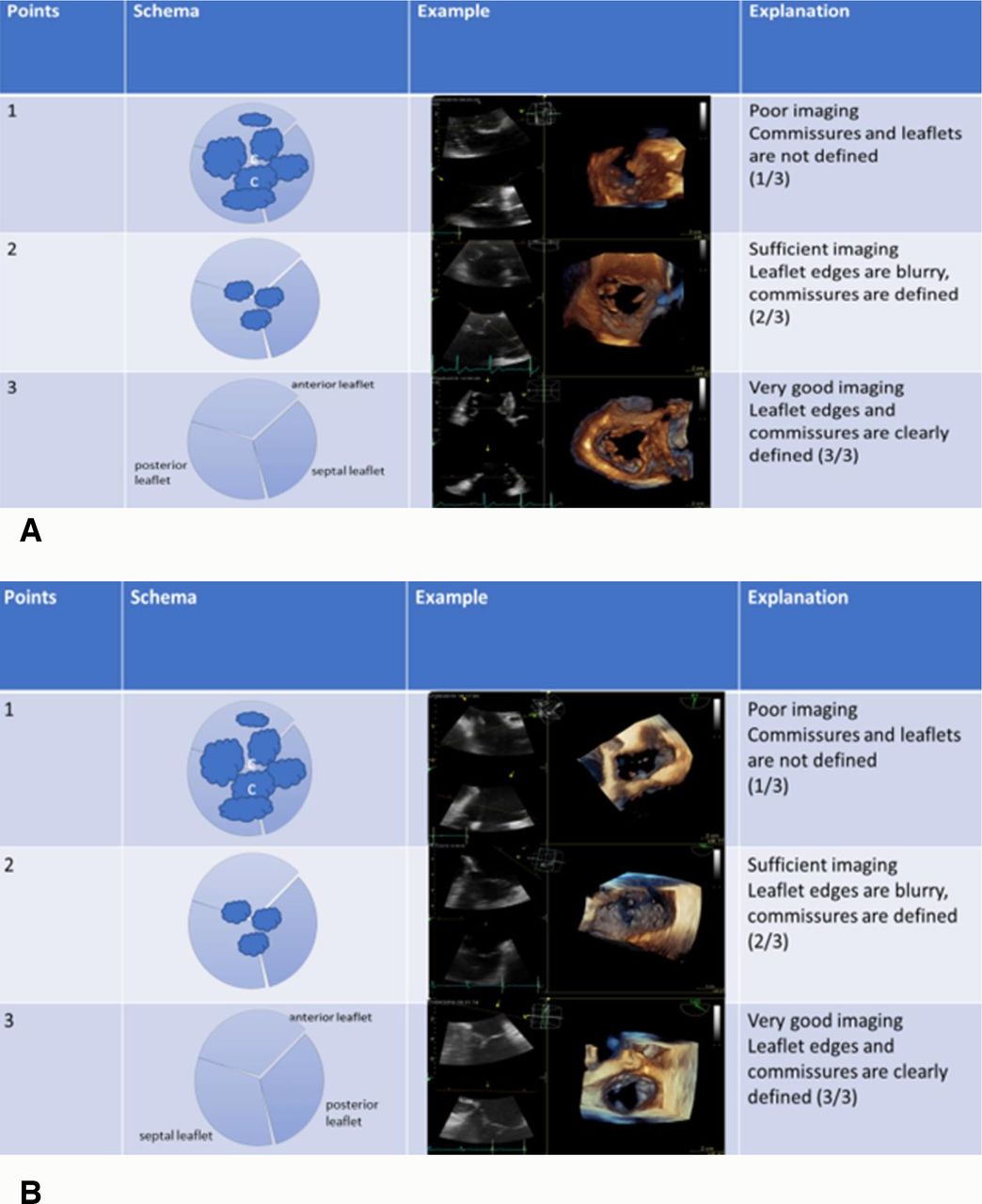
Three points: excellent imaging, leaflet edges are clearly defined.
Two points: sufficient imaging, leaflet edges are difficult to see, but commissures are clearly defined.
One point: poor imaging, leaflets edges and commissures cannot be clearly defined.
Adding all points (additive score), a maximum score of 15 points represents best visibility of all detailed structures, 5 points the worst. For analysis, we classified a score of 12–15 as excellent image quality, score of 8–11 as sufficient image quality and less than 8 points as poor image quality. The score was applied on four different views: parasternal long axis, parasternal short axis, apical four-chamber view (4 CV) and subcostal view. We stored 3D live imaging loops in each view.
Transoesophageal score for 3D imaging
During TOE, following single views were scored: (4 CV, 0° midoesophageal), right ventricular in and outflow (RVIO, 30° midoesophageal), long modified axis (LMA, 150° midoesophageal) and transgastral (30°). The scoring refers to the imaging of each single structure: TVR, each leaflet, imaging of the coaptation and of the Koch triangle (figure 1B).
In TOE imaging criteria such es clearly defined leaflet edges and commissures were used for the scoring of each single anatomical structures in a three-point system (figure 2B), similar to TTE.
By adding the score for each anatomical structure, the maximum possible score was 18 points. Accordingly, the minimum score was six points (one point for each structure). For analysis, we defined a score of 15–18 as excellent image quality, 10–15 as sufficient image quality and less than 10 as poor image quality.
Patients were examined with a Vivid E95 echocardiography system (GE Healthcare, 100 results way, Marlborough, Massachusetts, USA). To ensure comparable image quality, all patients were examined using the same platform. Due to the planned TOE with application of midazolam, examinations were performed in bed in left lateral decubitus. Examinations and all score calculations were performed by two experienced clinical specialists in echocardiography.
Statistical analysis was performed using IBM SPSS (V.20.0, USA) and GraphPad Prism (GraphPad Software V.6.0, USA). Continuous data are presented as mean±SD. To calculate significances, the Wilcoxon rank sum test was performed. p values <0.05 were considered as statistically significant.
After calculating the score, we compared patients with and without relevant TR. As a cut-off for significant TR, we used an effective regurgitant orifice (velocity time integral and proximal isovolumetric velocity area) of ≥0,4 cm² measured in 2D TTE.
Patients or the public were not involved in the design, or conduct, or reporting or dissemination plans of our research.
Results
We included 108 patients with a mean age of 70±12 years. The majority was men. 40.7% of patients presented with relevant TR. Patients with TR were significantly older. Detailed characteristics are found in table 1.
Patient characteristics in patients with relevant TR compared with those without relevant TR
Scoring results of all patients
Single anatomical structures: highest scores
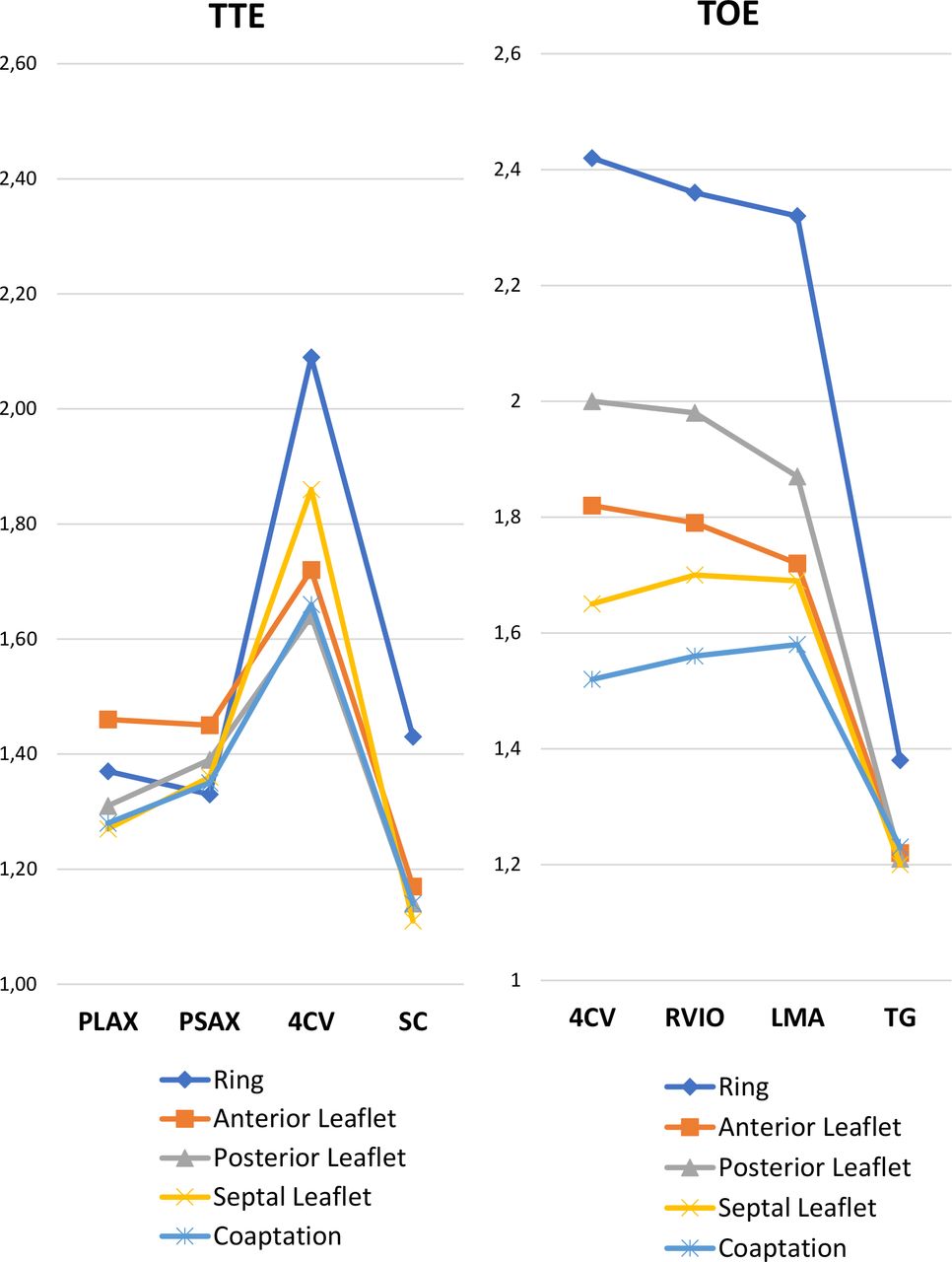
Table 2 shows the average scores for each anatomical structure. Highest scores were found for TVR, with TOE showing higher scores compared with TTE. The highest score for TVR was achieved in TOE in 4 CV (2.42±0.67) compared with TTE (2.09±0.66), p=0.003. Highest leaflet scores were found for PL in TOE in 4 CV (2.0±0.86). As shown in figure 3, PL was easier to visualise compared with SL and AL, regardless of the view.
Average scores of each anatomical structure and final additive score for each view
{kind=link}
{kind=link}
{kind=link}
Imaging scores for each single anatomical structure (maximum of three points) for TTE versus TOEE. 4 CV, four chamber view; LMA, long modified axis; PLAX, parasternal long axis; PSAX, parasternal shirt axis; RVIO, right ventricular in and outflow; SC, subcostal view; TG, transgastric view; TOE, transoesophageal echocardiography; TTE, transthoracic echocardiography.
Single anatomical structures: lowest scores
Coaptation had the lowest scores and was the only anatomical structure with better values in TTE compared with TOE (1.52±0.069), p=0.186. Highest scores for coaptation were found in TTE in 4 CV (1.66±0.84). Regarding the leaflets, SL had the lowest scores and therefore appeared to be the hardest to visualise.
Highest additive score for all anatomical structures
The highest scores for imaging of the TV, adding all points for each anatomical structure, were seen in TTE in 4 CV. In TOE, the highest average scores were found in 4 CV, RVIO and LMA. 3D TOE imaging was superior to TTE in almost all views (figure 3A,B). Further results are seen in table 2.
Figure 2A,B provides the examples for excellent, sufficient and poor image quality.
Comparison: relevant versus non-relevant TR
Forty-four patients presented with relevant TR. Indices for right ventricular function and right heart dilatation differed significantly between patients with and without relevant TR (table 1).
Single anatomical structures with highest scores
Table 3 shows the scoring results for each anatomical structure in patients with and without relevant TR. As for the complete cohort, TVR and PL had best results, regardless of TR severity. However, imaging of Koch triangle had significantly higher scores in 4 CV in TOE in patients with relevant TR (p<0.001). Especially in 4 CV in TOE all anatomical structures could be better visualised in patients with relevant TR. These results cannot be confirmed for other views.
Comparison of anatomical single structure scores between patients with relevant TR and without relevant TR in TOE views
Highest additive scores
Table 4 shows the average additive scores for each view in comparison between patients with and without relevant TR. The additive score in 4 CV in TOE showed significantly better results in patients with relevant TR (12.52 vs 10.3/p=0.002). Also, average additive scores for TTE were non-significantly higher in patients with relevant TR compared with those without TR.
Comparison of additive scores of patients with relevant TR and without relevant TR
Image quality: score distribution in patients with relevant TR
Most patients with relevant TR had at least one view with excellent (65%) or sufficient imaging quality (26%). Only four patients (9%) had no sufficient score in any view.
Only 6 out of 44 patients showed an overall good score in all TOE views.
TTE versus TOE
Table 5 shows the results of 4 CV in TTE versus TOE. Especially the scores of TVR and PL leaflet were significantly higher in TOE than in TTE. Imaging of the SL was non-significantly higher in TTE compared with TOE.
Comparison of mean scores of each anatomical structure in 4 CV in TTE and TOE in all patients
Discussion
We aimed to create a score for 3D imaging quality of the TV. The score enabled us to compare patients with and without relevant TR. 3D TTE and TOE imaging, both basic preprocedural examinations are recommend by various studies.2 9 10 Patients with insufficient visualisation are not suitable for an interventional procedure. Currently, sufficient literature on preferred views for certain anatomical structures of the TV is missing.
Imaging of TV compared with mitral valve is much more difficult due to less tissue thickness,11 which might lead to artefacts in the area of the leaflets. TV interventions can be divided into two groups: ‘anulus-based’ and ‘leaflet-based’ systems. Anulus-based systems such as Edwards cardioband tricuspid systems (Edwards Lifesciences, Irvine, California, USA)12 require sufficient visualisation of the TV ring. Via transvenous catheter technique, a band is attached to the ring from the RA side of the valve, aiming to reduce the ring circumference and ensure a better coaptation of the leaflets. While the TVR visualisation is crucial, visualisation of leaflets is not necessarily needed. Our data show that TVR is easiest to visualise, especially in 3D, probably due to thicker tissue and its location on the border of the valve with less movement. 49 of 108 (45%) examined patients had maximum scores of three points for single anatomic structures. Regarding patients with relevant TR, even more had best scores (25/44 in TOE 4 CV). Therefore, most of our patients were found suitable for an anulus-based intervention. Considering that moderate overall imaging is enough for an ‘anulus-based’ intervention, even 91% would be suitable. (40/44 in 4 CV in TOE).
The MitraClip XT System (Abbott, Abbott Park, Illinois, USA) is the most common ‘leaflet-based’ system.12 13 Via transvenous access, a clip that connects two leaflets is applied from the right atrial side of TV (edge to edge repair). Therefore, imaging of the leaflet edges is crucial. Successful grasping of leaflets requires optimal positioning perpendicular to the leaflet edges with enough tissue material in the clip, otherwise severe tissue damaging is being risked. Imaging of the leaflet edges is much more challenging, due to their thickness and permanent movement. It depends on the individuals’ imaging quality and can be assessed by our score. As all anatomical structures need to be perfectly visualised, only the minority of patients with a high additive score appear to be suitable for a ‘leaflet-based’ procedure. Our data show that 65% of patients with relevant TR have excellent imaging scores in at least one view. Under the assumption that a single view is not enough, excellent quality in all views should be assumed, which we could observe only very rarely. Only 6 out of 44 patients showed high scores in each view of TOE. The rare overall good imaging quality underlines the need for a structured individual screening process in preparation for echoguided intervention.
According to our data, the best views for 3D imaging of TV were 4 CV in TTE and 4 CV, RVIO and LMA in TOE. When scoring each anatomical structure individually, TVR appears to be the simplest structure to visualise. When assessing the leaflets, the PL had best scores in TOE, the SL was easier to visualise in TTE. As transgastric and SCs have lowest scores, the data indicate that these views are not suitable for 3D imaging. This does not imply that 2D data sets are not helpful for intervention steering.
Interestingly, we could identify that the 4 CV in TTE delivers scores comparable to the ones in TOE. All other views are inferior to 4 CV. To evaluate coaptation of leaflets and define relevant gaps, TTE 4 CV appeared even superior to TOE. TOE, however, was superior for the evaluation of the single leaflets, ring and Koch’s triangle.
Since there was a correlation between the extent of TR and imaging quality, we hypothesised that enlarged right ventricles and right atriums, the state of decompensation and fluid overload might enable a better view onto the TV. Hahn 7 postulated that due to the anterior position of the right heart, 3D TTE might be equal or even better than 3D TEE.9 Our findings confirm similar scores for the 4 CV in TTE. Furthermore, SL and coaptation may be easier to visualise in TTE. For all other anatomical structures, there is a clear advantage for TOE imaging.
Our study is a first approach in order to standardise imaging quality and enable comparability. The proposed score enables to measure image quality, an important prerequisite for carrying out an interventional treatment. We identified TVR and PL as easiest to visualise.
In summary, the score may help decide whether a patient is suitable for an echocardiography-guided intervention. Moreover, the score may help identify which procedures appear feasible in which patient. Using the score offers a standardised approach to examine the tricuspid valve and its anatomical structures.
Limitations
The average additive scores reflecting overall visibility of 3D TTE imaging were, except of the ones for 4 CV, very low. As all patients were planned for TOE with application of sedative, TTE was performed in a bedside setting. Usually, TTE is performed on special examination tables, which is crucial for excellent imaging. 3D acquisition depends on an excellent 2D image, which might be more difficult to obtain in this setting. Furthermore, tricuspid interventions are performed in general anaesthesia on the back which might change imaging quality again. Despite standardised examinations interobserver variability cannot be excluded. Reproducibility of the score by different examiners still needs to be investigated. The results need to be confirmed in a larger patient cohort and should be evaluated for interobserver and intraobserver variability.
Conclusion
TVR and PL achieve the highest scores and are therefore statistically easiest visualised in 3D TV imaging. This means that a ring-based intervention is suitable for more patients with relevant TR from an echo point of view. In order to screen patients for interventional treatment, a structured examination of the TV is necessary, which is achieved by applying the score. The score makes the subjective field of echocardiography more objective and comparable.
Footnotes
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The study was approved by the ethics committee of Brandenburg Medical School (E-01.20180730).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request. All data relevant to the study are included in the article or uploaded as supplemental information. Data (measurements) are stored anonymised and might be found and identified as echo data when needed.