Article Text

Abstract
Objective The association between the use of renin–angiotensin–aldosterone (RAAS) inhibitors and the risk of mortality from COVID-19 is unclear. We aimed to estimate the association of RAAS inhibitors, including ACE inhibitors (ACEi) and angiotensin II receptor blockers (ARBs) with COVID-19 mortality risk in patients with hypertension.
Methods PubMed (MEDLINE) SCOPUS, OVID, Cochrane Library databases and medrxiv.org were searched from 1 January 2020 to 1 September 2020. Studies reporting the association of RAAS inhibitors (ACEi or ARBs) and mortality in patients with hypertension, hospitalised for COVID-19 were extracted. Two reviewers independently extracted appropriate data of interest and assessed the risk of bias. All analyses were performed using random-effects models on log-transformed risk ratio (RR) estimates, and heterogeneity was quantified.
Results Fourteen studies were included in the systematic review (n=73,073 patients with COVID-19; mean age 61 years; 53% male). Overall, the between-study heterogeneity was high (I2=80%, p<0.01). Patients with hypertension with prior use of RAAS inhibitors were 35% less likely to die from COVID-19 compared with patients with hypertension not taking RAAS inhibitors (pooled RR 0.65, 95% CI 0.45 to 0.94). The quality of evidence by Grading of Recommendations, Assessment, Development and Evaluations was graded as ‘moderate’ quality.
Conclusions In this meta-analysis, with prior use of RAAS inhibitors was associated with lower risk mortality from COVID-19 in patients with hypertension. Our findings suggest a potential protective effect of RAAS-inhibitors in COVID-19 patients with hypertension.
PROSPERO registration number The present study has been registered with PROSPERO (registration ID: CRD 42020187963).
- hypertension
- antihypertensive drugs
- meta-analysis
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known about this subject?
SARS-CoV-2, responsible for the recent COVID-19 pandemic, interfaces with the renin–angiotensin–aldosterone system (RAAS) through ACE2. Recent studies have questioned whether RAAS inhibitors are safe in patients with COVID-19. However, observational studies involving patients hospitalised with COVID-19 that report the association of RAAS-inhibitors and COVID-19 severity or mortality risk have often yielded conflicting findings.
What does this study add?
The findings of this systematic review and meta-analysis suggest that prior use of RAAS inhibitors is associated with a lower risk of mortality by 35% in patients with hypertension hospitalised for COVID-19 (risk ratio 0.65, 95% CI 0.45 to 0.94).
How might this impact on clinical practice?
Patients taking RAAS-inhibitors to manage their hypertension should continue to do as per current treatment guidelines.
Introduction
severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), responsible for the recent COVID-19 pandemic, interfaces with the renin–angiotensin–aldosterone system (RAAS) through angiotensin-converting enzyme 2 (ACE2).1 2 The current hypotheses related to the influence ACE2 may have in facilitating virus severity and mortality have been inconclusive. The increased expression of ACE2 is thought to potentially catalyse infection with SARS-CoV-2, and therefore, increase the severity and risk of death.3On the contrary, it has been found that ACE2 may be protective against acute lung injury.4
ACE2 is an 805-amino-acid, homologous to the human ACE1, with 40% identity and 61% similarity.5 SARS-CoV-2 binds to the ACE2, which serves as host cell entry receptor.1 Prior research has suggested that ACE-inhibitors (ACEi) and angiotensin-II blockers (ARBs), which are commonly used in patients with hypertension, diabetes, chronic kidney disease and congested heart failure, may upregulate ACE2 expression and thus could increase the risk of severe SARS-CoV-2 infection.6 Although ACE1 and ACE2 are two different enzymes with different active sites, there are reports that ACEi affect the expression of ACE2 in the heart and kidneys.7 Furthermore, ARBs alter ACE2 expression, both at the mRNA and protein levels.7 8 ACE2 is upregulated in both the renal vasculature tissue and cardiac tissue as a result of RAAS inhibitor exposure.9
Individuals with cardiovascular disease including hypertension are at increased risk of death from COVID-19,10 and yet majority depend on RAAS inhibitors for hypertension control. Despite these theoretical uncertainties regarding whether pharmacological regulation of ACE2 may influence the infectivity of SARS-CoV-2, there is clear potential for harm related to the withdrawal of RAAS-inhibitors in patients in otherwise stable condition. Therefore, the potential influence of ACEi and ARB on the susceptibility of SARS-CoV-2 infection requires urgent exploration for a clarification.
To date, observational studies involving patients hospitalised for COVID-19 that report the association of RAAS-inhibitors and COVID-19 severity or death have yielded conflicting findings. Some studies report potential harmful associations of exposure to ACEi or ARBs with an increased risk of severity in COVID-19,11 and others have failed to confirm such findings of potential harmful association.12 13 Of note, these studies have significant unaddressed sources of bias that limit conclusions drawn from them. In this this systematic review and meta-analysis, the authors aim to delineate the association of RAAS-inhibitors use and mortality in patients with COVID-19. We hypothesise that RAAS-inhibitors may increase mortality rates from the novel coronavirus that causes COVID-19.
Methods
Search strategy and study selection
This study is being reported in accordance with the reporting guidance provided in the Preferred Reporting Items for Systematic Reviews and Meta-Analyses statement and Meta-analysis of Observational Studies in Epidemiology in online supplemental table 1.14 15 The authors state that all supporting data are available within the article and its online-only data supplement. We explored PubMed (MEDLINE) SCOPUS, OVID, Cochrane Library databases and medrxiv.org, using search criteria provided in online supplemental material text 1. We included all studies published from 1 January 2020 to 1 September 2020 that reported on the use of RAAS inhibitors (ACEi or ARBs) in patients hospitalised with COVID-19. We identified papers reporting the mortality risk in patients with and without exposure to RAAS-inhibitors. The following Medical Subject Heading and keywords were used for the literature search of PubMed and other databases: “receptors, angiotensin” OR “angiotensin” OR “angiotensin receptors” OR “angiotensin-converting enzyme inhibitors” “renin angiotensin aldosterone system” OR “angiotensin receptor blocker” OR “ace inhibitor” OR “angiotensin converting enzyme inhibitor” AND “SARS-CoV-2” OR “COVID-19” OR “coronavirus”. Two reviewers (ESH and AES) initially screened the titles and abstracts of all papers for eligibility. We included articles that reported the rates of death in COVID-19 patients with and without taking RAAS inhibitors. No limitations were applied on study design, country of publication or language. We excluded case reports or case series with less than 10 patients, studies not conducted on humans, review papers, meta-analyses, literature reviews and commentaries. Excluded studies were documented with reasons for their exclusion.
Supplemental material
Data extraction
Two reviewers (ESH and AES) then screened full-text articles. If necessary, a third reviewer (PS) was consulted in order to reach a consensus. Data extracted included the author, year of publication, country of publication, sample size, the number of patients in the RAAS inhibitor group that did or did not die, and the risk ratio (RR) estimates and 95% CI of mortality in the RAAS-inhibitor group compared with the non-RAAS inhibitor group, the mean or median age with their corresponding SD or IQR, respectively, the proportion that is male, and the covariates adjusted for in each study. We gave priority to adjusted RR estimates if available.
Study quality assessment and confidence in cumulative evidence
Two reviewers (ESH and AES) independently assessed the quality of the included studies. The Newcastle-Ottawa Scale (NOS) was used for the quality assessment of included studies.16 NOS rates observational studies based on three parameters: selection, comparability between the exposed and unexposed groups, and exposure/outcome assessment. This scale assigns a maximum of four stars for selection, two stars for comparability and three stars for exposure/outcome assessment. Studies with less than five stars were considered low quality, studies receiving five through seven stars were considered moderate quality, and those receiving more than seven stars were classified as high quality. We assessed the quality of evidence (QoE) using the Grading of Recommendations, Assessment, Development and Evaluations (GRADE) framework using four levels of QoE: very low, low, moderate and high.17 The following domains were used for the assessment: risk of bias, imprecision, inconsistency, indirectness and publication bias.18 We reported the overall strength of evidence of the outcome of interest.
Data analysis
The primary outcome of interest was mortality in patients with hypertension hospitalised for COVID-19. The exposure of interest was the prior use of RAAS-inhibitors. We used the reported RR, HR OR as the measures of the association between exposure to RAAS-inhibitors and the risk of mortality in COVID-19. For studies without measures of associations, we applied a generalised linear mixed model to calculate the RR using the number of events and the sample size of each study group.19 We invoked a random-effects model to pool study results for the association between exposure to RAAS-inhibitors and the risk of mortality using the metagen function from the R package meta.20 The DerSimonian and Laird method was used to estimate the pooled interstudy variance (heterogeneity).21 We constructed forest plots to display pooled estimates. We assessed interstudy heterogeneity using I2 statistics, expressed as % (low (25%), moderate (50%) and high (75%)) and Cochrane’s Q statistic (significance level <0.05).22 23
Due to the potential differences in the study population in terms of sociodemographic characteristics and the possible confounding in the studies with unadjusted estimates (studies we calculated RR), we expected to see large variations in the effect estimates. Therefore, subgroup analysis comparing studies with and without adjusted estimates was done. We hypothesised that the studies with unadjusted estimates will yield larger effect sizes compared with studies with adjusted estimates. Furthermore, outlier and influence diagnostics sensitivity analysis was undertaken to explore the effect of each individual study on the overall pooled estimate.24 Additional sensitivity analysis was conducted where we included additional studies whose sample size was not limited to the population with hypertension. We did not conduct meta-regression analysis to explore sources of variation due to lack of sufficient number of studies (less than 10 for the main analysis). For the similar reasons, we did not create funnel plots or conduct Egger’s test.25 All statistical analyses were performed with R software, V.3.4.3 (R, College Station, Texas, USA).
Results
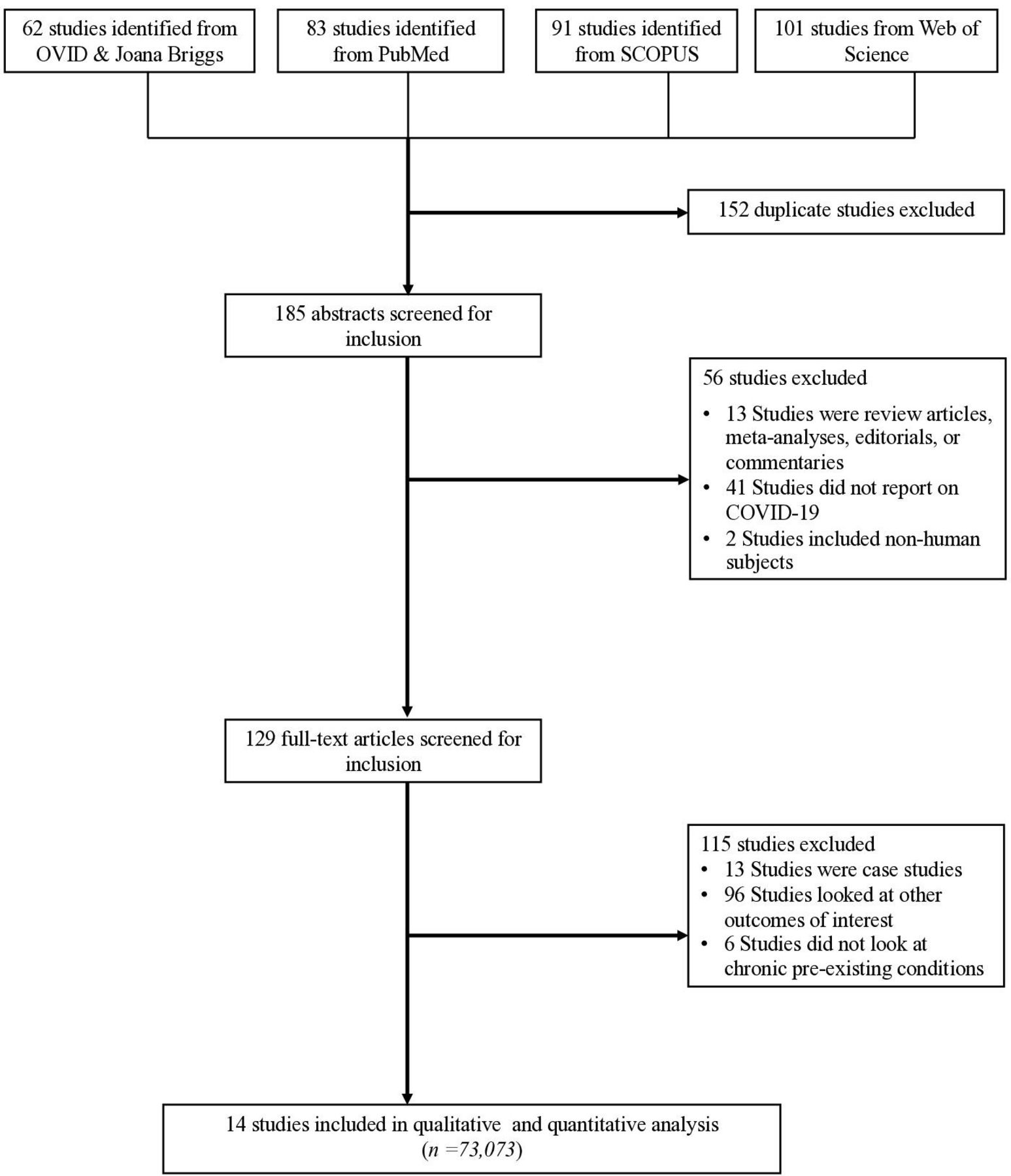
As shown in figure 1, we identified a total of 337 studies from the five databases. We excluded 152 studies because they were duplicates, leaving 185 studies. When screening titles and abstracts, we excluded 56 studies and another 115 based on full text, which left us with 73,073 patients with and COVID-19 from 14 studies for qualitative analysis and 72,981 patients from 12 studies for the quantitative analysis (table 1).11 12 26–37 The mean age was 61 years and 53% were male. The QoE by GRADE for the deaths was graded as ‘moderate’ quality (table 1). The median study quality score for studies was 8 out of 9 (range=7–9, table 1). Study-specific details and references are given in table 1.
Characteristics for studies included in the systematic review and meta-analysis
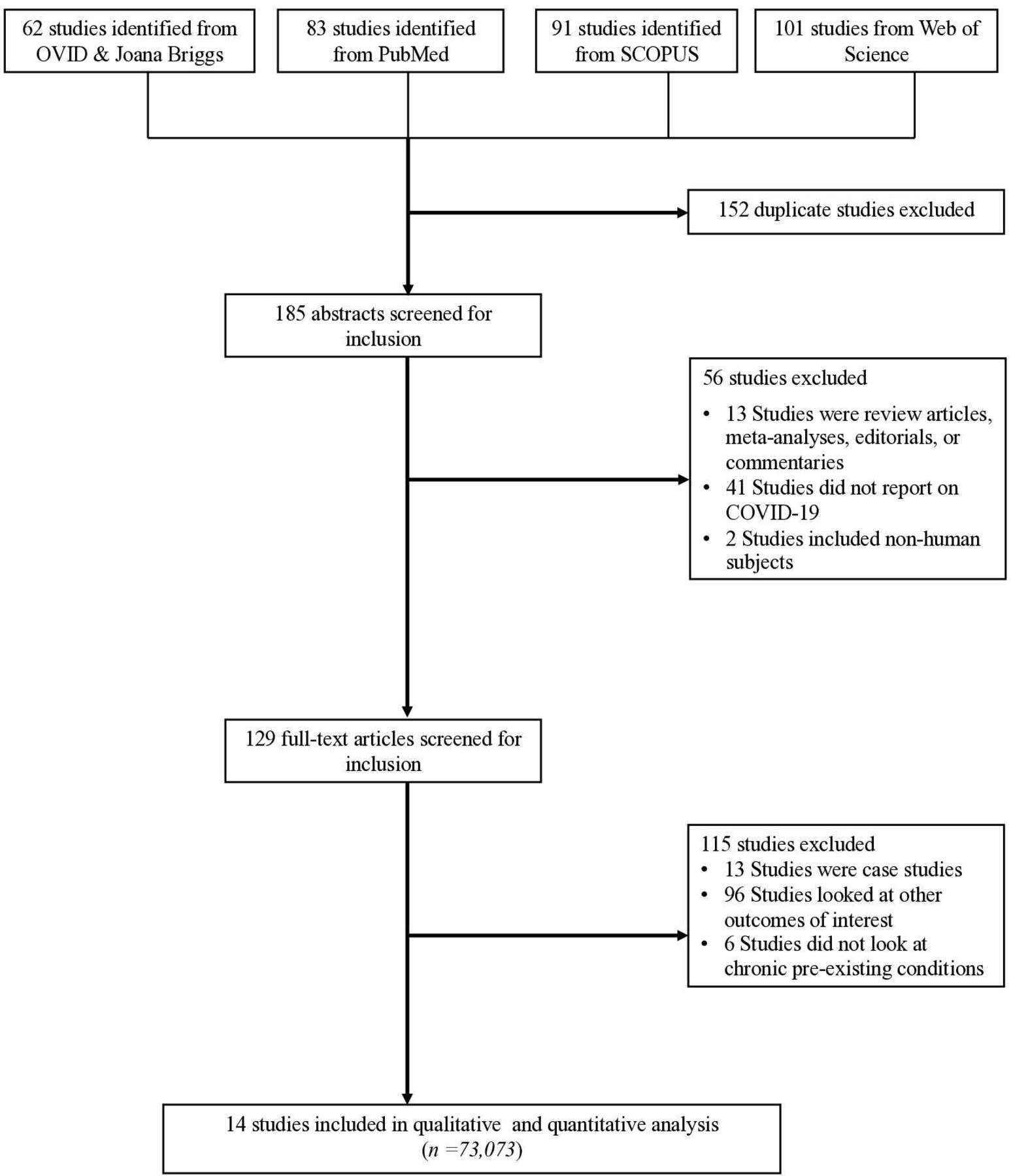
PRISMA flow diagram. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
The association between taking RAAS inhibitors and COVID-19 mortality
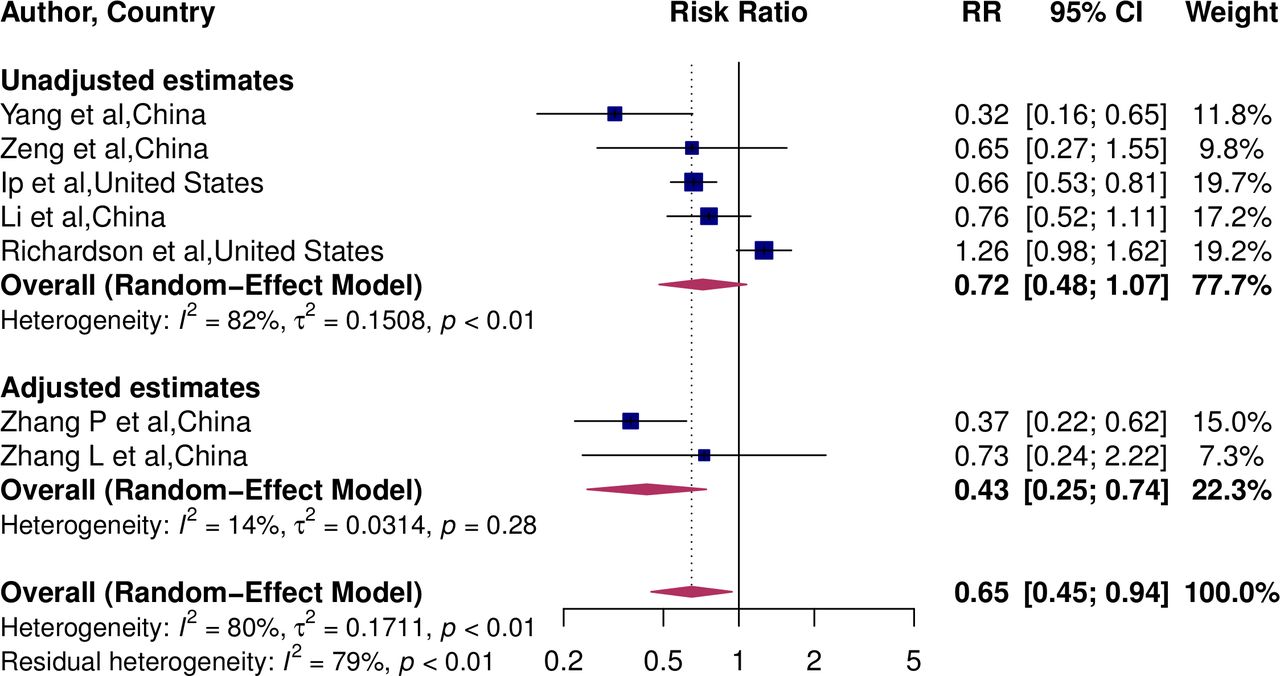
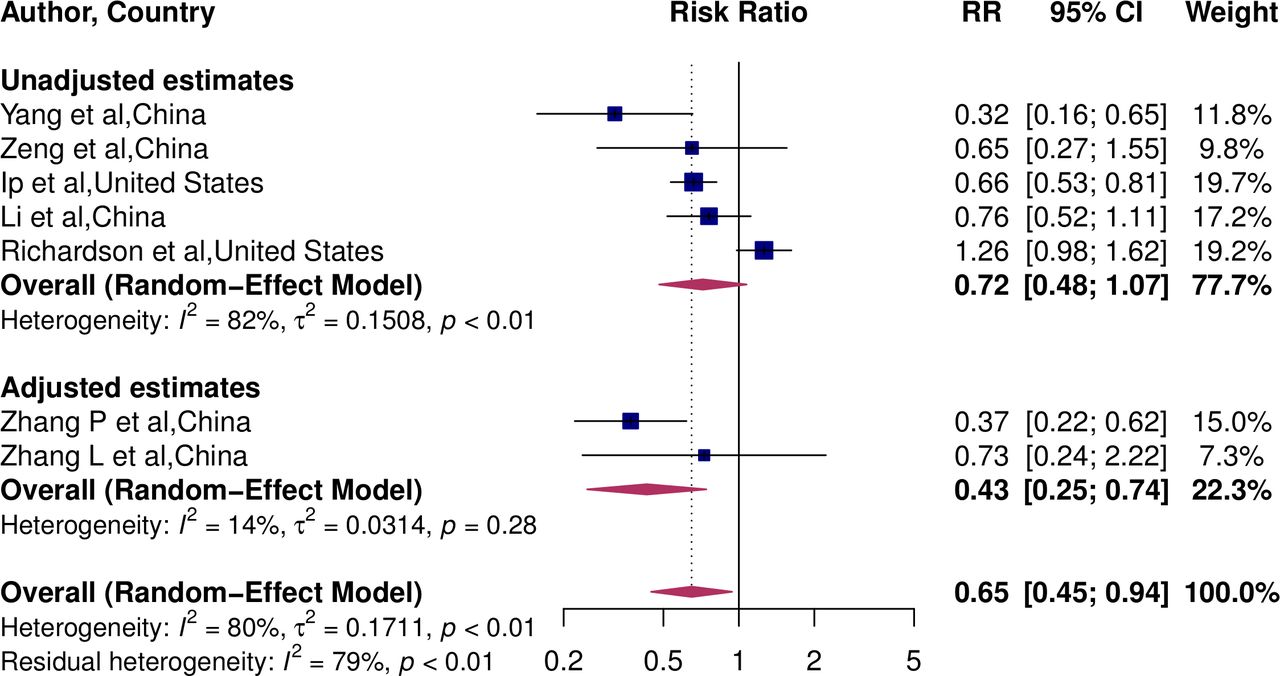
Of the seven studies,11 12 31 34–36 included in the meta-analysis exploring the association between COVID-19 mortality and RAAS exposure in patients with hypertension, three reported a significantly lower risk with mortality (figure 2).12 34 36 No studies reported a significantly higher risk of mortality. The overall pooled estimates showed a 35% lower risk of mortality (RR 0.65, 95% CI 0.45 to 0.94). Between-study heterogeneity was high (I2=80%, p<0.01).

Pooled RR for the association of RAAS-inhibitors and COVID-19 mortality. RAAS, renin–angiotensin–aldosterone.
Subgroup analysis
We conducted subgroup analysis to explore whether there is a difference in pooled RR between studies that did and did not have adjusted RR estimates. The pooled RR of studies with adjusted estimate was 0.43 (95% CI 0.25 to 0.74), implying a 57% lower risk of death (figure 3). However, the pooled RR of studies with unadjusted estimates was 0.72 (95% CI 0.48 to 1.07), implying a lack of association with mortality risk (p for interaction=0.14).
{kind=link}
{kind=link}
{kind=link}
Pooled RR estimates of studies by covariate adjustment.
Sensitivity analyses
We conducted influential sensitivity analysis in which we excluded and replaced one study at a time from the meta-analysis and calculating the pooled RR for the remaining studies. No substantial changes from pooled RR were observed when other studies were removed in turn. The pooled RR ranged from 0.57 to 0.72 (p<0.0001 for all) (online supplemental figure 1). Next, we calculated the pooled estimates by including all studies (main analysis from seven studies shown in figure 2 plus five studies whose sample size was not limited to the population with hypertension).26 28 32 33 37 The pooled RR including all studies was 0.77 (95% CI 0.63 to 0.95). However, pooled RR was lower in studies with population not limited to patients with hypertension 0.87 (95% CI 0.68 to 1.10) compared with studies consisting of only patients with hypertension (online supplemental figure 2).
Discussion
Principal findings
This systematic review and meta-analysis of cohort studies consisting of 73 073 patients with a global representation suggests that the treatment of hypertension with RAAS-inhibitors is associated with a lower risk of mortality in patients with COVID-19. This finding is important, for the association between RAAS-inhibitor exposure and mortality in COVID-19 patients has been inconclusive thus far. This topic has been heavily debated, and some studies even have interpolated a risk of taking RAAS-inhibitors using data from previous coronavirus outbreaks and preclinical studies.6
Comparison with other studies
This review provides up-to-date results for the contribution of RAAS-inhibitor use on the lower risk of mortality in patients with hypertension hospitalised for COVID-19 by synthesising a large number of recently published studies. The study yielded a large number of individuals from countries representing Europe, North America and Asia. Our study findings are similar to results from a previously published systematic review, suggesting a lower mortality in patients with hypertension hospitalised for COVID-19.38 Guo et al evaluated studies published until 13 May 2020, and included 3936 patients from nine studies.38 They found a 43% (95% CI 0.38% to 0.84%) lower risk in mortality in patients with hypertension hospitalised for COVID-19. In the current meta-analysis, the risk of mortality was approximately 35% lower in patients with COVID-19. Furthermore, a large-scale retrospective study demonstrated that in-hospital use of ACEi/ARBs was associated with a lower risk of 28-day death among hospitalised patients with COVID-19 and coexisting hypertension (adjusted HR 0.32, 95% CI 0.15 to 0.66).12 These data suggested that patients with hypertension might obtain benefits from taking ACEi/ARBs compared with the non-ACEi/ARBs in the setting of COVID-19. In addition to what is reported in published studies, this systematic review and meta-analysis incorporated evidence from the most recent studies, and a large sample size.
Potential mechanisms
RAAS-inhibitors have been found to mitigate the risk of severe lung injury by reducing the activation of the RAAS through the inactivation of angiotensin II4 and the generation of angiotensin (1–9)5 and angiotensin (1–7).39 Angiotensin (1–7) binds to the G protein-coupled receptors Mas to mediate various physiological effects including vasorelaxation, cardioprotection, antioxidation and inhibition of angiotensin II-induced signalling. This is one hypothesised mechanism illustrating how the treatment of chronic conditions with RAAS-inhibitors may be beneficial in COVID-19 patients. Alternatively, it is hypothesised that the biological mechanisms of RAAS inhibitors may predispose COVID-19 patients to severe disease and even mortality. These hypotheses are based on the observation that SARS-CoV-2 binds to the ACE2, which serves as host cell entry receptor. Animal models suggest that ACEis and ARBs increase membrane-bound ACE2 receptors, which then increases the availability of cells for SARS-CoV-2 to bind and cellular entry.7 This hypothesis has sparked a debate in populations, for many individuals taking RAAS inhibitors have grown concerned that their medications may be predisposing them to developing COVID-19, and later dying from it.40 Our meta-analysis supports the notion that RAAS inhibitor exposure does not increase COVID-19-related mortality but rather shows a possible beneficial effect. Future studies should continue to explore the association between COVID-19 and the use of RAAS-inhibitors to further ascertain these findings.
Implications for research and clinical practice
The majority of patients with pre-existing cardiovascular disease, hypertension, diabetes, chronic kidney disease and congestive heart failure use RAAS blockers to manage their conditions. Our findings suggest that patients taking RAAS-inhibitors to manage their chronic diseases may continue to do as per current treatment guidelines and based on the clinical judgement of their healthcare providers
Strengths and limitations
Limitations of our study include possible selection bias in the published literature as a result of the strict COVID-19 testing algorithm employed in the early stages of the pandemic. This may have resulted in missed COVID-19 cases or deaths. Nevertheless, this is the largest quantitative synthesis of evidence on the association between RAAS-inhibitor exposure and COVID-19 mortality. The regions with the highest burden of COVID-19, including Asia, Europe and North America, were represented thus increasing the external validity of our findings. The sample size included in this study was also quite large, allowing us to thoroughly cover a large population.
Conclusion
In this meta-analysis, prior use of RAAS inhibitors was associated with a lower risk mortality from COVID-19 in patients with hypertension. Our findings suggest a potential protective effect of RAAS-inhibitors in COVID-19 patients with hypertension. Patients taking RAAS-inhibitors to manage their chronic diseases may continue to do as per current treatment guidelines and based on the clinical judgement of their healthcare providers.
Acknowledgments
We would like to acknowledge Melissa Butt for reviewing and proving helpful feedback.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @annassentongo
AES, PS and ESH contributed equally.
Contributors AES, PS, ESH and VMC conceived the study. AES, ESH and PS conducted the literature search. AES and PS completed data analysis. AES, DL, PD, VMC, AL, JSO, ESH and PS interpreted the data. AES, ESH and PS wrote the manuscript. All authors agreed to the manuscript in its final form.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval This is a systematic review and meta-analysis and individual patient was not used. Therefore we did not need IRB or an ethics board approval.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as online supplemental information.