Article Text

Abstract
Background and purpose Real-world data about treatment convenience and satisfaction in Asian non-valvular atrial fibrillation (NVAF) patients after switching from vitamin K antagonists (VKAs) to non-VKA oral anticoagulants were evaluated.
Methods In this non-interventional study involving 49 sites across five countries in Southeast Asia and South Korea, 379 stable NVAF patients who switched from VKA therapy to dabigatran during routine clinical practice were recruited and followed up for 6 months. Treatment convenience and satisfaction were evaluated using Perception on Anticoagulant Treatment Questionnaire-2 (PACT-Q2). Through post hoc analysis, factors associated with improved treatment convenience scores at visit 2 were described.
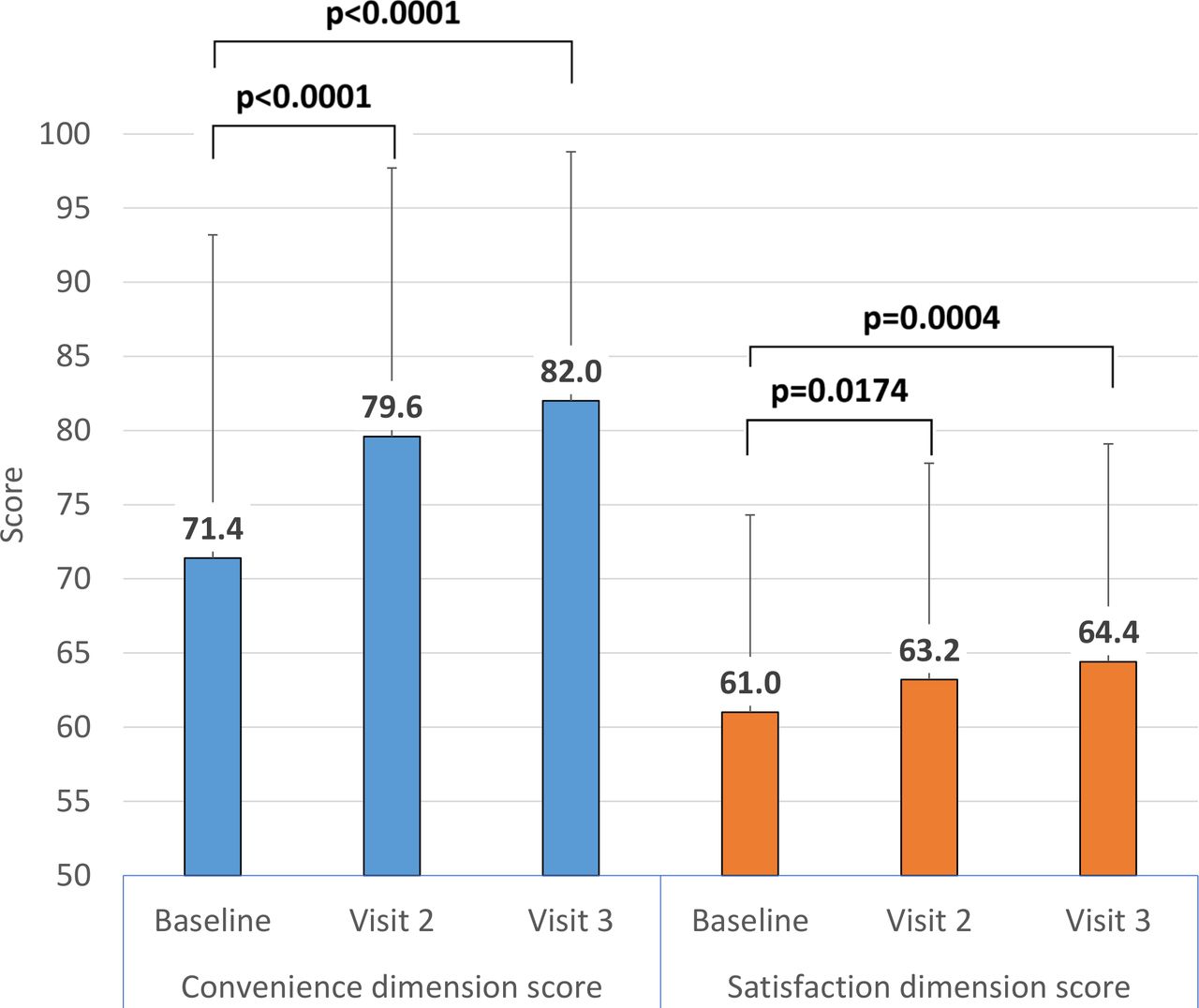
Results Treatment convenience and satisfaction significantly improved after switching from VKAs to dabigatran at visit 2 and visit 3 (convenience: p<0.001 each vs baseline; satisfaction: p=0.0174 (visit 2), p=0.0004 (visit 3) compared with baseline). Factors predictive of higher (>80th percentile) response on treatment convenience were female sex, younger age (<75 years), higher baseline stroke risk, higher creatinine clearance and absence of concomitant hypertension, stroke or gastrointestinal diseases.
Conclusion Dabigatran was associated with a significant improvement in treatment convenience and satisfaction after switching from VKAs when used for stroke prevention in NVAF patients from Southeast Asia and South Korea.
- stroke
- atrial fibrillation
- anticoagulation
- oral anticoagulants
- quality of care and outcomes
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known about this subject?
Non–vitamin K antagonist (VKA) oral anticoagulants (NOACs) are increasingly used for stroke prophylaxis in non-valvular atrial fibrillation (NVAF) patients.
The safety and efficacy of NOACs, as well as advantages they provide in terms of lower drug–drug and drug–food interactions, over VKAs, are well established.
However, data on patient-reported outcomes (such as treatment convenience and satisfaction) and factors influencing patients’ perception of NOACs when given for stroke prophylaxis in NVAF patients are not well characterised.
What does this study add?
This study evaluates the influence on the perception and satisfaction of stable NVAF patients when their anticoagulation therapy in routine clinical course is switched from VKA to dabigatran, an NOAC. Further, it characterises baseline factors predictive of significant changes in perception and satisfaction score.
When switched from VKAs to the NOAC dabigatran, patients’ treatment convenience and satisfaction significantly improved at follow-up visit (7– 124 days) compared with baseline scores.
The factors predictive of significant improvement include female gender, age <75 years, higher baseline stroke risk, higher creatinine clearance, and without baseline hypertension, stroke and gastrointestinal disorders.
Key questions
How might this impact on clinical practice?
Patient preferences are an important part of clinical decision -making.
The differential scores of patient perception and satisfaction after switching from VKA to an NOAC should form an integral part of patient–physician dialogue and will allow more informed decision -making for treatment of NVAF patients for stroke prevention.
Introduction
The burden of non-valvular atrial fibrillation (NVAF) among the Asian population is increasing.1–3 Intracranial haemorrhage leading to stroke is a prominent complication of NVAF,4 and the incidence of stroke and intracranial bleeding is higher among Asian patients with atrial fibrillation (AF) compared with non-Asians.5 6 Oral anticoagulants prevent ischaemic stroke in NVAF patients and therefore form an essential part of NVAF treatment. However, they also confer a risk of serious bleeding.7 The traditionally used vitamin K antagonists (VKAs), including warfarin, have additional disadvantages of numerous food and drug interactions, which require frequent patient monitoring.8
The non-VKA oral anticoagulants (NOACs) were first introduced for clinical use in 2008 for stroke prevention in patients with NVAF after many clinical trials established their safety, efficacy and non-inferiority in comparison with warfarin.9–12 Also, recent studies have demonstrated the safety and effectiveness of NOACs in real-world clinical practices.13 14 Currently, four NOACs, namely, apixaban, dabigatran, edoxaban and rivaroxaban, are licensed for use in the USA and Europe for this indication.15 The use of NOACs for stroke prevention in NVAF is recommended by several international guidelines,16–18 and is also a well-established clinical practice across the world.19
It has been reported that NVAF patients who are initiated on oral anticoagulants are increasingly being treated with NOACs when compared with the VKAs.20 However, there is lesser data on the switching of VKAs to NOACs in stable NVAF patients. Further, international guidelines recommend NOAC initiation over VKAs in NVAF but do not recommend routine switching of stable VKA users to NOACs.19 21
It is unclear whether such switching of anticoagulation in stable NVAF patients from VKAs to the direct thrombin inhibitor NOAC dabigatran etexilate (Pradaxa, Boehringer Ingelheim) would result in an improvement in the convenience and satisfaction in a real-world setting. The RE-LATE (real-world evaluation of long-term anticoagulation treatment experience) study explored the patient expectation, treatment convenience and satisfaction among NVAF patients from Southeast Asia and South Korea who are treated with dabigatran, using the PACT-Q (Perception on Anticoagulant Treatment Questionnaire) in a real-world setting.22 In the current paper, we aim to find predictors related to a higher treatment convenience and satisfaction among patients with AF who switched from warfarin to dabigatran for stroke prevention in the RE-LATE study.
Materials and methods
Study design, sites and institutional review board approval
This study was a part of the larger RE-LATE study, which explored the patient perception of long-term anticoagulation therapy with dabigatran in a real-world setup. RE-LATE was a multicentre, non-interventional study involving 49 centres across five countries in the region (South Korea: 33 centres, Thailand: 6 centres, Malaysia: 5 centres, Singapore: 3 centres and Indonesia: 2 centres) that prescribed both VKAs and dabigatran for stroke prevention in NVAF patients, according to the approved label of the respective country. The study protocol was approved by the institutional review boards (IRBs) of each individual centre, with the exception of Singapore where the Centralised Institutional Review Board (Domain C) approved the protocol for all the three participating centres. The detailed list of all the involved centres and IRBs is available from the corresponding author on reasonable request. The study was conducted between June 2016 and December 2017. All the study participants fitting the inclusion criteria were administered written informed consent prior to the initiation of the study (figure 1).

RE-LATE (real-world evaluation of long-term anticoagulation treatment experience) study design, VKA, vitamin K antagonist; PACT-Q1, Perception on Anticoagulant Treatment Questionnaire-1; PACT-Q2, Perception on Anticoagulant Treatment Questionnaire-2.
Patients
For the present study, consenting patients with NVAF of either sex, aged ≥18 years, who were already on VKA therapy for at least 3 months duration and subsequently switched over to dabigatran therapy, were recruited to this study. Patients having any contraindication for the use of dabigatran, patients already receiving any VKA or dabigatran for any other indication apart from stroke prevention in AF, patients participating in any other clinical trial at the same time, patients participating in any registry (such as the GLORIA registry programme) and non-consenting patients were excluded from the study.
Treatment details
The decision for switching from VKA to dabigatran was taken prior to and independently of enrolment into the study. Only after the treatment decision for a patient had been made, the investigators could check and decide if the patient could be enrolled in the study. The dosing of dabigatran (either 110 mg two times per day or 150 mg two times per day) was based on the clinician’s discretion and according to the approved country label. All concomitant medications were prescribed based on the underlying medical condition and on the discretion of the treating physician. No treatment was withheld from the patients.
Data collection
Patients were followed up for a median period of 6 months with data collection at three time points: visit 1 (baseline), visit 2 (7–124 days after recruitment) and visit 3 (125–365 days after recruitment). At the baseline visit, demographic details, HAS-BLED (hypertension, abnormal renal/liver function, stroke, bleeding history or predisposition, labile international normalised ratio, elderly (> 65 years), drugs/alcohol concomitantly) score for bleeding risk and CHA2DS2-VASc (congestive heart failure, hypertension, age ≥75 years (double score), diabetes, stroke or transient ischemic attack (TIA; double score), vascular disease, age 65–74 years, sex class) score for stroke risk were recorded. Baseline patient convenience and treatment satisfaction with the VKAs were recorded using the PACT-Q2, which is a validated, specific tool to measure quality of life among patients receiving anticoagulants. The PACT-Q2 is a 20-item questionnaire for assessing the treatment convenience and treatment satisfaction with ongoing anticoagulation therapy in patients with AF and also in DVT and PTE.22 23 Higher scores in PACT-Q2 indicate better convenience and higher treatment satisfaction.22 Validated translations of the PACT-Q2 questionnaires were provided to the patients in the language of their choice (namely, Chinese, English, Indonesian, Korean, Malay, Mandarin, Tamil and Thai). During both the two subsequent visits, the patients were administered PACT-Q2 questionnaire to capture the progressive changes in the patient convenience and treatment satisfaction. Also, any adverse reactions were recorded. Details of concomitant illness and therapies, creatinine clearance and weight were recorded during all three visits.
Data analysis
All data were recorded electronically. The mean PACT-Q2 scores at second and last assessments were compared with baseline scores using paired t-test. The mean PACT-Q2 scores of the last assessment were also compared with mean scores at the second assessment using paired t-test.
Post hoc analysis was performed to identify the patient factors associated with patients reporting good and poor improvement of convenience at visit 2, by using the standardised difference (SDf) of different factors between the super-responders (upper 20th) and poor responders (lower 20th percentile). Data from visit 2 were chosen instead of visit 3 because of the larger sample size during visit 2 than during visit 3. All statistical analyses were performed using SAS (version 9.3; SAS Institute, Cary, NC, USA). At least one of the authors had full access to all the data in the study and takes responsibility for data integrity and the analysis of data.
Results
A total of 49 participating sites from across the five countries were involved in the study, which enrolled a total of 389 patients with stable NVAF who were switching from VKA to dabigatran over a period of 18 months (from June 2016 to December 2017). A total of 379 patients were found to be eligible for the study, out of which 249 (65.7%) were male. The patients had NVAF for a median duration of 3.7 years and were on VKA therapy for anticoagulation for a median duration of 3.3 years. The baseline demographic details are summarised in table 1. A total of 258 patients (68.1 %) received dabigatran at low dose (110 mg two times per day), whereas the remaining 121 (31.9 %) received a higher dose of dabigatran (150 mg two times per day).
Baseline demographic details of patients recruited in the study
The treatment convenience and treatment satisfaction captured in the PACT-Q2 questionnaire significantly improved in visits 2 and 3 when compared with baseline. The improvement in treatment convenience and treatment satisfaction scores was not statistically significant between visit 2 and visit 3 (table 2, figure 2). The baseline PACT-Q2 scores were not available for 2 out of the 379 patients.
{kind=link}
{kind=link}
Mean Perception on Anticoagulant Treatment Questionnaire-2 scores of non-valvular atrial fibrillation patients showing statistically significant improvement in convenience and satisfaction after switching over from vitamin K antagonist to dabigatran.
PACT-Q2 scores of NVAF patients switching from VKA to dabigatran
In the subgroup analysis of PACT-Q2 scores among the patients divided according to the age group, patients aged under 65 years had the lowest mean convenience dimension scores during all three visits, when compared with older patients, suggesting that older patients were on average more positive with respect to treatment convenience than younger patients. The highest satisfaction dimension scores were observed in the patients belonging to the age group 65–75 years; these patients also had significant improvement in treatment satisfaction from baseline values (table 3).
Subgroup analysis of PACT-Q2 scores according to age group
The result of post hoc analysis to determine the factors predicting good and poor response in terms of change from baseline of PACT-Q2 treatment convenience score at visit two is summarised in table 4. Among 317 patients who had PACT-Q2 scores available at visit 2, the paired data of baseline and visit 2 PACT-Q2 scores were available for only 316 patients. Based on the observed SDfs, when compared with the poor responders (lower 20th percentile), the super-responders (upper 20th percentile) had a higher proportion of female patients (SDf=−0.1385), a lower proportion of patients age ≥75 years (SDf=0.2018), a higher proportion of patients with CHA2DS2-VASc score ≥2 (SDf=−0.2886), a higher proportion of patients without disease of the gastrointestinal (GI) system (SDf=−0.1792) and a lower proportion of patients with concomitant hypertension and stroke (SDfs 0.1879 and 0.2014, respectively). Also, the mean creatinine clearance was higher among the super-responders compared with the non-responders (SDf=−0.1759).
Demographic data and baseline characteristics by percentiles of change from baseline of PACT−Q2 convenience score at visit 2 and their standardised differences
Adverse drug reactions (ADRs) were reported by 44 patients (11.6%) overall. The vast majority of the ADRs (39/44) were non-serious, and the most frequent ADRs were GI disorders (34/44). Serious ADRs were observed in five patients overall, including one fatal event. ADRs lead to dose change in two patients and treatment discontinuation in 27 patients.
Discussion
We have described the perception of stable NVAF patients with respect to their treatment convenience and treatment satisfaction on anticoagulation therapy with VKA and how these changed after switching over to dabigatran, over a period of 6 months. This study collected data from a real-world setting in multiple centres across five countries in Southeast Asia using the PACT-Q2 questionnaire. To the best of our knowledge, this is the first study that has described the patient perception of oral anticoagulation in patients with NVAF in this geographical region.
The mean age was 69.7±9.0 years, and there was a male predominance (65.7%). Thus, the population of the present study was younger and had slightly higher male predominance than the population in the GARFIELD-AF (Global Anticoagulant Registry in the FIELD-Atrial Fibrillation) registry24 and the GLORIA-AF (Global Registry on Long-Term Oral Antithrombotic Treatment in Patients with Atrial Fibrillation) registry.25 The male predominance in our study was similar to that observed in the PREFER in AF (PREvention oF thromboembolic events–European Registry in Atrial Fibrillation) registry26; however, our study had a younger population. The average CHA2DS2-VASc scores and HAS-BLED scores in our study were slightly lower than the three registries.
We found that among patients who switched from VKAs to dabigatran, treatment convenience and satisfaction significantly improved from baseline to second visits, and the effect persisted to the third visit. These findings clearly suggest that NVAF patients perceive dabigatran better and more favourably than VKAs.
Starting from the 1980s and 1990s, the VKAs were considered as the gold standard for stroke prevention in NVAF patients.27 Since VKAs have a narrow therapeutic range, and since the international normalised ratio (INR) of patients undergoing anticoagulation therapy has to be maintained between 2 and 3, the use of VKA has been considered to be challenging. Further barriers to the usage of VKAs included a high interindividual variability in response to treatment, the need for regular monitoring of INR, a high number of food and drug interactions. Collectively, these factors lead to poor patient adherence to treatment and make optimal therapy with VKAs more challenging in practice for patients.28 Also, Asian patients have been observed to have a poor quality of anticoagulation control, as demonstrated by the low time in therapeutic range (TTR).29
Ever since the approval of the NOACs for anticoagulation in NVAF patients, the uptake of these by clinicians worldwide has been phenomenal, so much so that experts are predicting a gradual phasing out of the usage of VKAs for this indication.30 The NOACs do not have as many interactions as do the VKAs, and thus do not need routine monitoring of coagulation, unlike the VKAs, both of which eventually lead to better patient convenience and satisfaction as demonstrated in this study by higher PACT-Q2 scores after switching to Dabigatran from VKA therapy.
Guidelines worldwide now recommend the usage of NOACs over VKAs for treatment initiation. The 2016 ESC (European Society of Cardiology) guidelines also include a consideration of switching to a NOAC from VKAs due to patient preference.21 When NOACs were relatively new for practicing physicians, the PREFER IN AF registry substudy found that patients who switched over to NOACs from VKAs more often reported bruising or bleeding, dissatisfaction with the anticoagulant treatment, and reported mobility problems and anxiety/depressive traits than patients who were on stable VKA therapy.26 With the passing of time and increasing experience with the use of NOACs, the trend seems to have reversed, with the present study demonstrating an improvement of treatment satisfaction and treatment convenience after switching over from VKAs to dabigatran.
The 2016 ESC guidelines also recommend switching of anticoagulation from VKAs to NOACs if the TTR control is poor despite drug adherence.21 Contrary to this recommendation, however, a recently published study from Denmark has found that over 84% of patients were continued on VKAs despite poor TTR control of below 70%, and switching over to NOACs is practised less often.31 Further, Asian NVAF patients with a SAMe-TT2R2 score of ≥2 would have poor TTR control with warfarin, which suggests that they are good candidates for the initiation of NOAC therapy.18
The data on the percentage of patients switching over from stable use of VKAs to NOACs are varying across the world. A study from the USA published in 2013 reported that around 8% of patients switched over from VKA to dabigatran after 12 months of follow-up, and the switching was mainly driven by physician preference and patient preference.32 A study from Denmark reported that in 2015 only 29.6% of patients on VKAs were switched over to NOACs.20 A 2018 study from The Netherlands reported that up to 27% of patients who were prescribed NOACs between 2011 and 2016 had switched over from VKAs.33
By performing a subgroup analysis, we aimed to explore if any pattern can be observed for the improvements in convenience and satisfaction and patient age groups. While convenience and satisfaction showed a trend towards gradual improvement among all the age groups considered in the subgroup analysis, this improvement was statistically significant in comparison with the baseline, in the age group of 65–75 year patients. Further, the baseline values for convenience and satisfaction scores were the highest (indicating the poorest convenience and satisfaction with VKAs) in the same age group. This indicates that the patients belonging to the age group of 65–75 years demonstrate faster improvement in convenience and satisfaction after switching over to dabigatran when compared with those who are younger than 65 years and older than 75 years. Further research is needed to explore the specific reasons behind this observation.
The post hoc analysis revealed that patients belonging to the female sex, aged <75 years, having higher stroke risk (in terms of higher CHA2DS2-VASc score), higher creatinine clearance, not having a concomitant disease affecting the GI tract and not having concomitant hypertension and stroke were associated with better treatment convenience with dabigatran treatment. In line with previous studies, several factors affecting treatment response with dabigatran and other NOACs were reported.34 To the best of our knowledge, this is the first attempt to describe factors affecting the patient-related outcomes such as treatment convenience. Identification of predictors for convenience would help to tailor treatment options for stroke prevention. The safety data collected in our study are consistent with the existing safety profile of dabigatran and do not give rise to any new safety signals.
This study has several strengths including the real-life setting, patients from a multiple number of countries, non-restrictive entry criteria that permitted the enrolment of a broad patient population, the use of standardised and validated questionnaires translated to the language comfortable to the respondent, and a study design that allowed the collection of cross-sectional data at baseline and longitudinal follow-up data. The major limitation of this study is a relatively smaller sample size when compared with similar studies in the past. However, these studies with larger sample sizes were analyses of registry data, and ours being prospectively conducted, a longitudinal follow-up study has a stronger design. Second, analyses of factors predictive of better treatment convenience were post hoc and should be interpreted with caution.35 Further studies are warranted to confirm these findings using a planned prospective study. Third, the data of treatment satisfaction and convenience were considered from visit 2, which represents the immediate change from baseline, instead of data from visit 3, which might have represented a more sustained improvement in these parameters. Fourth, the selection bias at the site level cannot be ruled completely since a larger number of cardiologists rather than general practitioners or other specialists participated in the study. Finally, most patients who took part in this study came from reimbursed settings.
Conclusions
The RE-LATE study evaluated the perception of NVAF patients towards anticoagulant treatment for the prevention of stroke in Southeast Asia and South Korea. The perception of treatment in terms of treatment convenience and satisfaction was significantly better among patients who are switched from VKA to dabigatran. Patients belonging to the female sex, aged <75 years, having higher stroke risk, higher creatinine clearance and not having a concomitant GI disease were associated with better treatment convenience with dabigatran treatment.
Acknowledgments
Medical writing assistance was provided by MarksMan Healthcare Communications (India) and was funded by Boehringer Ingelheim.
References
Footnotes
Twitter @alankoay81
Contributors E-KC: Substantial contributions to the conception and design of the work, acquisition of data, analysis and interpretation of data, revising the work critically for important intellectual content. Y-SL: Substantial contributions to the conception and design of the work, acquisition of data, analysis and interpretation of data. AKCC: Substantial contributions to the acquisition of data, analysis and interpretation of data. PJ: Substantial contributions to the acquisition of data, analysis and interpretation of data. AC: Substantial contributions to the acquisition of data, analysis and interpretation of data. DAH: Substantial contributions to the acquisition of data, analysis and interpretation of data. PT: Substantial contributions to the conception and design of the work, analysis and interpretation of data, and having the work drafted and revised. DZ: Substantial contributions to the analysis and interpretation of data, and having the work drafted and revised. YSO: Substantial contributions to the conception and design of the work, acquisition of data, analysis and interpretation of data. All authors have approved the submitted version. All authors have agreed to be personally accountable for the work, and to ensure that questions related to the accuracy or integrity of any part of the work (even ones in which the authors were not personally involved) are appropriately investigated, resolved, and the resolution documented in the literature.
Funding Financial support for the conduct of this study and the preparation of this manuscript was provided by Boehringer Ingelheim.
Competing interests E-KC has received modest research support from Daiichi-Sankyo, BMS/Pfizer and Biosense Webster, unrelating to the current study. Y-SL reports no conflicts of interest relating to the current study. AKCC reports no conflicts of interest relating to the current study. Panyapat Jiampo has received modest research grants and honoraria from Boehringer Ingelheim, relating to the current study. AC has received modest research grants and honoraria from Boehringer Ingelheim, relating to the current study. DAH has received modest research grants and honoraria from Boehringer Ingelheim, relating to the current study. PT and DZ are employees of Boehringer Ingelheim. YSO has received significant research grants from Daiichi-Sankyo and Boehringer Ingelheim, relating to the current study.
Patient consent for publication Not required.
Ethics approval The study protocol was approved by the institutional review boards (IRBs) of each individual centre (49 centres across 5 countries in the South East Asian Region; Indonesia: 2 centres, Malaysia: 5 centres, Singapore: 3 centres, South Korea: 33 centres and Thailand: 6 centres), with the exception of Singapore where the Centralised Institutional Review Board (Domain C) approved the protocol for all the three participating centres. The detailed list of all the involved centres and IRBs is available from the corresponding author on reasonable request. All the study participants fitting the inclusion criteria were administered written informed consent prior to the initiation of the study.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.