Article Text

Abstract
Objective To evaluate how common echocardiographic metrics of aortic stenosis (AS) influence the proportion of patients who may be categorised as having severe stenosis and therefore considered for valve replacement.
Methods Retrospective analysis was performed of all echocardiograms with aortic valve area (AVA) ≤1.2 cm2 and peak jet velocity (Vmax) ≥3 m/s from 1 December 2014 through 30 October 2017 at a single academic medical centre. Echocardiographic indices collected include AVA, Vmax, left ventricular ejection fraction, stroke volume and annotated aortic stenosis severity.
Results Among 807 patients with AVA ≤1.2 cm2 and Vmax ≥3 m/s (44.0% female, median age 74 years (IQR: 66–81)), 45.6% had Vmax ≥4 m/s, while 75.8% had AVA ≤1 cm2. 40.0% of patients had concordant indices (Vmax ≥4 m/s and AVA ≤1 cm2), and 35.8% had discordant indices (Vmax <4 m/s and AVA ≤1 cm2) of severe AS. Compared with those with concordant indices, patients with discordant indices were more commonly female (54.0% vs 44.3%, p<0.05) and less commonly characterised as severe (42.6% vs 93.8%, p<0.001). Patients with paradoxical low-flow, low-gradient severe AS by echocardiography were disproportionately female (61.5% vs 41.8%, p<0.001), and their disease was characterised as severe only 49.5% of the time.
Conclusions Patients with discordant indices, who are disproportionately female, are commonly described in clinical echocardiography reports as having less than severe AS. Given the potential benefit of AVR in patients with AVA ≤1 cm2 regardless of Vmax, this could have important clinical implications.
- aortic valve disease
- echocardiography
- epidemiology
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known about this subject?
Patients with aortic stenosis are generally referred for aortic valve replacement (AVR) when their stenosis is considered ‘severe’, but discordance between aortic valve area and peak jet velocity (Vmax) can cause confusion regarding the severity of stenosis.
What does this study add?
This analysis of echocardiography data from 807 patients reveals that there is a large population of patients with discordant indices of aortic stenosis (AS) who are disproportionately female and less commonly characterised as having severe AS on an echocardiography report despite meeting echocardiographic criteria for severe AS.
How might this impact on clinical practice?
Echocardiographers may be reluctant to characterise patients with discordant indices as having ‘severe AS’. Clinicians are reluctant to refer patients without ‘severe AS’ for consideration of AVR, yet there is a potential benefit of AVR in these patients. Perhaps, the echocardiography report ought to indicate that these patients may require further evaluation and testing (eg, valve calcium scoring by CT) to determine whether AS is severe so that referral for valve replacement is not unnecessarily delayed.
Introduction
Aortic stenosis (AS) accounts for approximately 15 000 deaths in North America each year, and the only effective treatment is surgical or transcatheter aortic valve replacement (AVR).1 Currently, AVR is recommended in patients with severe, symptomatic AS and in some cases in those with severe, asymptomatic AS.2 Determination of AS severity relies primarily on the haemodynamic indices of peak jet velocity (Vmax) or mean transvalvular gradient across the aortic valve, and secondarily on decreased aortic valve area (AVA).3 Commonly, patients are considered to have severe AS when they meet both the AVA criteria (≤1 cm2) and haemodynamic criteria (Vmax ≥4 m/s or mean gradient ≥40 mm Hg).2 However, the guidelines also indicate that patients with Vmax 3.0–3.9 m/s and AVA ≤1 cm2 (‘discordant AS’) may have severe AS if certain criteria apply.2 A number of prior studies have demonstrated that such a discordance between these indices is common and suggested that patients with discordant AS would see a survival benefit from AVR.4–9 Nonetheless, this discordance can yield uncertainty regarding the severity of AS, which influences clinical management.6 7
Herein, using echocardiographic data obtained in clinical practice, we evaluated how these indices of severe AS (Vmax ≥4 m/s and AVA ≤1.0 cm2, both individually and together) influence the proportion of patients who may be categorised as having severe AS. For each of these groups potentially categorised as having severe AS, we evaluated how often the AS was qualitatively described as ‘severe’ in the clinical echocardiographic report. We were particularly interested in the relationship between sex and categorisation of AS severity.
Methods
Clinical transthoracic echocardiogram reports from 1 December 2014 to 30 October 2017 were retrospectively extracted from the Synthetic Derivative, a de-identified mirror of the electronic health record at Vanderbilt University Medical Center,10 using previously described approaches that include regular expressions and natural language processing.11 12 These echocardiographic reports were generated in the course of clinical practice in the Vanderbilt University Medical Center echocardiography laboratory, where readers are instructed to follow society guidelines for characterisation of the severity of AS.2 3 For each patient, the report with the smallest AVA calculated by the velocity time integral continuity equation was identified, and all data were extracted from this report. No patient was analysed twice, and in no cases were data from two separate reports combined. Records missing data were excluded. Patients with AVA ≤1.2 cm2 and Vmax ≥3 m/s were analysed to include the spectrum of severe AS disease phenotypes. Patients with a severe Vmax may have AVA >1 cm2 in cases of aortic regurgitation, leading to our 1.2 cm2 criterion, and the AHA/ACC guidelines specifically state that patients with AVA ≤1 cm2 but >0.8 cm2 should have a Vmax ≥3 m/s to be considered severe, thus forming the inclusion criteria for our study.2 Patient records with either a procedural code for AVR prior to the echocardiography date or an ICD9/10 code for obstructive cardiomyopathy at any time were excluded.
At the time of echocardiography, measurements were taken in accordance with the guidelines of the American Society of Echocardiography.3 Left ventricle outflow tract (LVOT) diameter and Doppler tracings were made by a sonographer and confirmed or remeasured by the echocardiographer interpreting the study. The echocardiogram was the only basis for severity characterisation. Severity is stratified between ‘mild’, ‘moderate’ and ‘severe,’ with combinations commonly used (ie, ‘mild–moderate’ and ‘moderate–severe’). All charts with no AS characterisation identified after natural language processing were reviewed manually.
Echocardiographic metrics were compared between male and female patients using Mann-Whitney U test. Binned data were compared using χ2 test. All statistical analysis was performed using the statistical programming language R, V.3.5.2.13 The data used in this study are available to others for replication of our findings or further analyses and can be obtained by contacting the corresponding author.
Patient and public involvement
We did not directly include patient and public involvement in this study, but community representatives are involved in oversight of the database used in the study (the Synthetic Derivative) through the Vanderbilt Institute for Clinical and Translational Research.
Results
Among 807 patients (44.0% female) who had a recorded AVA ≤1.2 cm2 and Vmax ≥3 m/s, the median AVA was 0.86 cm2 (IQR: 0.70–1.00) and median Vmax was 3.87 m/s (IQR: 3.41–4.38) (table 1). Based on the Vmax ≥4 m/s criterion, 45.6% of the cohort was classified as having severe AS (table 2). In contrast, based on the AVA ≤1.0 cm2 criterion, 75.8% was classified as having severe AS. This represents a relative 66.3% increase in the proportion of patients who would be classified as having severe AS when using the AVA criteria instead of the Vmax criteria, and would particularly increase the proportion of female patients considered to have severe AS (44.9% vs 96.7% relative increase in the proportion of male vs female patients) (table 2). Using an indexed AVA (AVAi) cut-off of ≤0.6 cm2/m2, 94.1% of the cohort would be classified as having severe AS, including 99.0% of those with an AVA ≤1.0 cm2.
Cohort characteristics
Aortic valve area and peak jet velocity as indices of severe aortic stenosis
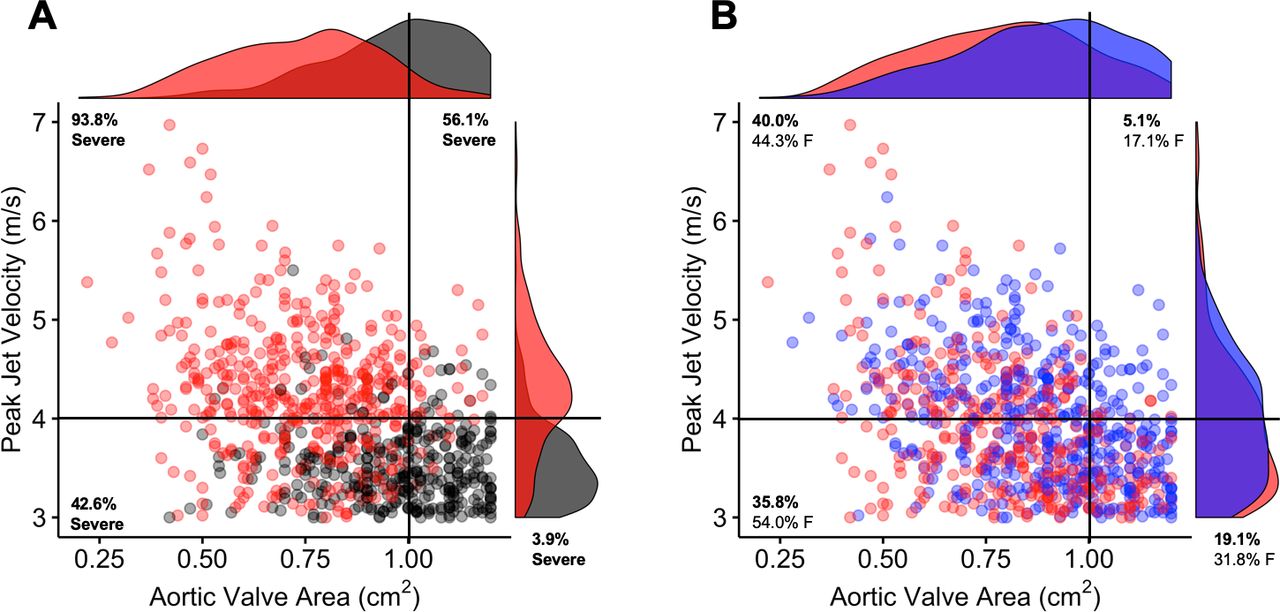
Patients with discordant indices of severe AS (Vmax <4 m/s and AVA ≤1 cm2) made up 35.8% of the study cohort, and those with concordant indices of severe AS (Vmax ≥4 m/s and AVA ≤1 cm2) comprised 40.0%. Compared with those with concordant indices, those with discordant indices were more likely to be female (54.0% vs 44.3%, p=0.02) and less likely to have their AS characterised as ‘severe’ on the clinical echocardiography report (42.6% vs 93.8%, p<0.001) (table 2). This difference persisted when expanding the ‘severe’ group to include those characterised as ‘moderate–severe’ (71.6% vs 98.8%, p<0.001). Replacing Vmax with mean gradient yields similar results with identical conclusions (online supplementary table 1, online supplementary figure 1). When AVAi ≤0.6 cm2/m2 replaced AVA ≤1 cm2, patients with discordant indices were again less often characterised as ‘severe’ on the echocardiography report than those with concordant indices (32.2% vs 90.3%, p<0.001). Figure 1A shows data plotted by Vmax and AVA, colour coded by the AS characterisation on the echocardiography report. The percentages reported as severe for each quadrant defined by an AVA of 1.0 cm2 and Vmax of 4 m/s are also shown. In figure 1B, data are plotted and colour coded by sex, and each quadrant shows the proportion of the population represented and the percentage female.
Supplemental material

{kind=link}
The relationships of recorded severity and sex with AVA and peak jet velocity. (A) All patients in the cohort are plotted in both one and two dimensions by AVA and peak jet velocity, and colour-coded by clinician characterisation as severe (red) or non-severe (grey). The percentage of patients characterised as severe is annotated for each quadrant. (B) This same cohort is plotted coloured by female (red) and male (blue) sex. The percentage of the cohort in each quadrant, as well as the percentage of each quadrant that is comprised of female patients, is noted. AVA, aortic valve area.
We further investigated these trends by comparing patients with discordant AS who were characterised as having either ‘severe’ or ‘non-severe’ disease (table 3). There were no differences between the groups with respect to body size or LVOT dimension. Although all patients had an AVA and AVAi below the threshold for severe AS, those characterised as ‘severe’ on the echocardiography report had lower AVA and AVAi and a higher transvalvular gradient than those characterised as ‘non-severe’. To identify any subgroups that may be underdiagnosed, we divided patients with discordant AS into stages as defined by AHA/ACC recommendations (table 4).2 Among those with AVA ≤1.0 cm2, AVAi ≤0.6 cm2 and Vmax <4 m/s, patients with ejection fraction (EF) <50% (potentially stage D2 patients depending on the results of a dobutamine echocardiogram) comprised 7.3% of the total study cohort (20.8% of those with discordant indices) and were infrequently female (27.1%), and patients with EF ≥50% comprised 27.8% of the study cohort (79.2% of those with discordant indices). Among this latter group, those with paradoxical low-flow, low-gradient AS (stroke volume index <35 mL/m2, stage D3 by echocardiography) represented 11.3% of the study cohort (32.2% of those with discordant indices), were disproportionately female (61.5% vs 41.8%, p<0.001), and were characterised as having ‘severe’ AS only 49.5% of the time. Online supplementary figure 2 shows data plotted by Vmax and AVA, colour coded with ‘low-flow’ status by stroke volume index (≥35 mL/m2 vs <35 mL/m2) in all patients. Left ventricular internal diameter was also assessed for characterisation of those with discordant AS, and within each sex there were no significant differences between those with non-severe, severe and discordant severe AS (online supplementary table 2).
Characteristics of patients with discordant aortic stenosis characterised as either severe or non-severe
Left ventricle metrics and characterisation of echocardiography in patients with discordant aortic stenosis
Discussion
Using data from clinical echocardiography reports of patients with AVA ≤1.2 cm2 and Vmax ≥3 m/s, we found that shifting from a specific definition of severe AS (Vmax ≥4 m/s) to a sensitive definition (AVA ≤1 cm2) resulted in a 66% relative increase in the number of patients with potentially severe AS, with a 97% relative increase in female patients. This observed increase is similar to previously reported data,8 9 but it also provides quantitative insight into how this move would affect female patients in particular. Furthermore, while patients with concordant indices of AS severity by echocardiography are usually characterised as having severe AS (94% of the time in our study), discordant indices are common (observed almost as commonly as concordant indices among those with AVA ≤1 cm2), disproportionately observed in female patients, and yield a characterisation of ‘severe’ AS a minority of the time (43%).
To our knowledge, this is the first study to demonstrate how echocardiographic data are integrated by an echocardiographer when reporting the overall AS severity in a clinical report. This has important implications, as those who receive and read an echocardiography report (particularly if they do not have expertise in valve disease or reading raw echocardiography images) may not be inclined to refer a patient with anything less than ‘severe AS’ for AVR consideration. In this sense, the summary statement of AS severity on the clinical echocardiography report often drives subsequent clinician behaviour.
With this in mind, the fact that less than half of the patients with discordant AS—including less than half of those who meet the definition of paradoxical low-flow, low-gradient severe AS—are reported as having ‘severe AS’ on the clinical echocardiography report is consequential. Multiple recent studies, although retrospective and non-randomised, report a survival advantage from AVR for those with AVA ≤1 cm2 regardless of Vmax.4–6 Berthelot-Richer et al reported improved survival with AVR over medical therapy for those with Vmax 3–4 m/s, transvalvular mean gradient 25–40 mm Hg and AVA≤1 cm2,4 and Dayan et al reported improved survival with AVR for the same group, even when assessing specifically the subgroup with preserved stroke volume index (normal-flow, low-gradient AS).5 Notably, these studies did not include, for example, valve calcium scoring to clarify the severity of AS when indices were discordant, and they included the resting echocardiographic indices alone (as in our study). Thus, regardless of additional testing or measures of ventricular performance, patients with these discordant indices of AS severity seem to benefit from AVR. Since the guidelines recommend AVR only for patients with ‘severe AS’ and patients with discordant indices of AS severity are commonly characterised as having less than severe AS on echocardiography reports, this undoubtedly influences clinical management decisions and leads to less and later referrals for AVR as prior studies have shown.4 6 7 14
This particularly affects female patients who were disproportionately represented among those with discordant AS in our analysis. Indeed, female patients seem to suffer from disproportionate delay of referral for AVR.14 The prevalence of discordant AS in female patients could be due to several factors including differences in valve calcification and flow. Previous studies have shown that while AS is driven primarily by calcification in male patients, there is a more dominant fibrotic component in female patients.15 Between these, calcification was seen to be associated with higher gradients.15 Female patients also tend to have a lower stroke volume than male patients, which is associated with lower transvalvular gradients.16
The frequent characterisation of patients with discordant AS indices as having less than severe AS is likely due to two primary reasons. First, it is likely influenced by the explicit prioritisation in the guidelines of Vmax and transvalvular mean gradient over AVA in the assessment of AS severity.2 17 18 While updates in the guidelines have increasingly allowed for subgroups of patients to be classified as having severe AS despite a Vmax <4 m/s, the long-standing paradigm of prioritising Vmax over AVA leads to clinicians reluctant to classify a patient as having severe AS with Vmax <4 m/s. However, the rationale for prioritising Vmax over AVA in the diagnosis of severe AS is based on small studies that neither examine hard clinical events nor compare prompt AVR versus clinical surveillance at various Vmax or AVA thresholds.19 20 Second, in cases of discordant measurements, additional testing with nitroprusside,21 dobutamine,22 or aortic valve calcium scoring is increasingly performed to clarify whether AS is severe.23 24 Previous work has highlighted the need for such additional testing in discordant AS.25 Knowing this, echocardiographers may be reluctant to over-call ‘severe AS’ when they know these additional tests may help clarify the diagnosis. However, to readers of echocardiography reports who do not commonly care for patients with AS, the diagnosis of anything other than ‘severe AS’ on the echocardiography report may simply be interpreted as a signal to ‘continue watching’ that patient rather than to perform an adjunctive test to clarify the true severity of stenosis.
Systems-level changes may be warranted to address these challenges, which likely have adverse clinical consequences. So as not to potentially delay referral for valve replacement in patients with discordant indices of AS severity, if the echocardiographer is not going to characterise discordant AS indices (AVA <1 cm2 and Vmax <4 m/s) as ‘severe’ on the clinical report, then it may be appropriate to include the following on the report: ‘possibly severe AS, but additional evaluation or testing is needed.’ This would enable the echocardiographer to not ‘over-call’ severe AS when they believe further testing is needed, but also help ensure that these patients with discordant indices are not passively watched but instead further evaluated and, as appropriate, referred for AVR in a timely manner. In addition, quality improvement efforts in echocardiography laboratories could reinforce that a Vmax ≥4 m/s is not required for the diagnosis of severe AS.
Limitations
In this cross-sectional study based solely on echocardiography data, we do not have information on clinical presentation, symptoms, referral to AVR or long-term outcomes. Furthermore, we do not have data from dobutamine echocardiograms or valve calcium scores from CT studies. Our focus was on relating the haemodynamic indices of AS obtained on an echocardiogram to how echocardiographers assimilate that information and report a summative characterisation of AS severity. Using the resting echocardiographic indices alone is consistent with the fact that most of the studies on the relationship between AS severity and outcomes simply rely on these resting echocardiographic haemodynamic indices (AVA, Vmax) and not on adjunctive information from stress testing or valve calcium scores. Additionally, we did not assess for measurement error or attempt to validate sonographer measurements. Importantly, we are not commenting here on the underlying biology or pathology. Instead, we have evaluated the cardiologist’s qualitative read given these values. Finally, these data were collected from a single academic medical centre, which may not be representative of other echocardiography laboratories.
Conclusions
The proportion of patients and relative percentage of female patients potentially categorised as having severe AS is markedly influenced by the echocardiographic indices of severe AS used. Clinical echocardiography reports usually characterise discordant indices of AS severity, which are common and disproportionately observed in female patients, as less than severe, which could have adverse clinical consequences. When discordant indices of AS severity are encountered and characterisation of AS severity is uncertain, notation in the clinical echocardiography report of the need for additional evaluation or testing may minimise the number of patients who experience a delay in referral for AVR.
References
Footnotes
Twitter @MichaelR21, @merrymanlab
Contributors Study conception and design: MAR, BRL and WDM. Acquisition and technical analysis of the data: MAR, EF and QSW. Data interpretation: MAR, HMG, BRL and WDM. Manuscript preparation: MAR, HMG, BRL and WDM.
Funding This work was funded by the NIH (R35-HL135790, F30-HL147464 and T32-GM007347) and Fondation Leducq. The data sets used for the analyses described were obtained from Vanderbilt University Medical Center’s BioVU and Synthetic Derivative, which are supported by numerous sources: institutional funding, private agencies and federal grants. These include the NIH-funded Shared Instrumentation grant S10RR025141, and CTSA grants UL1TR002243, UL1TR000445 and UL1RR024975. The views expressed are those of the authors and not necessarily those of the National Institutes of Health, Fondation Leducq, Vanderbilt University or Vanderbilt University Medical Center.
Competing interests BRL has received research grants from Edwards Lifesciences and Roche Diagnostics; served on scientific advisory boards for Roche Diagnostics and has been a consultant to Medtronic and Roche Diagnostics.
Patient consent for publication Not required.
Ethics approval Use of the Synthetic Derivative is classified as non-human research by Vanderbilt University’s Institutional Review Board (IRB), and approval was given for this study (IRB #180320).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Deidentified data are available upon reasonable request by contacting david.merryman@vanderbilt.edu.