Article Text

Abstract
Objective To conduct a landscape assessment of public knowledge of cardiovascular disease risk factors and acute myocardial infarction symptoms, cardiopulmonary resuscitation (CPR) and automated external defibrillator (AED) awareness and training in three underserved communities in Brazil.
Methods A cross-sectional, population-based survey of non-institutionalised adults age 30 or greater was conducted in three municipalities in Eastern Brazil. Data were analysed as survey-weighted percentages of the sampled populations.
Results 3035 surveys were completed. Overall, one-third of respondents was unable to identify at least one cardiovascular disease risk factor and 25% unable to identify at least one myocardial infarction symptom. A minority of respondents had received training in CPR or were able to identify an AED. Low levels of education and low socioeconomic status were consistent predictors of lower knowledge levels of cardiovascular disease risk factors, acute coronary syndrome symptoms and CPR and AED use.
Conclusions In three municipalities in Eastern Brazil, overall public knowledge of cardiovascular disease risk factors and symptoms, as well as knowledge of appropriate CPR and AED use was low. Our findings indicate the need for interventions to improve public knowledge and response to acute cardiovascular events in Brazil as a first step towards improving health outcomes in this population. Significant heterogeneity in knowledge seen across sites and socioeconomic strata indicates a need to appropriately target such interventions.
- coronary artery disease
- emergency medicine
- resuscitation
- acute coronary syndrome
- delivery of care
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known about this subject?
Cardiovascular disease is the leading cause of morbidity and mortality worldwide accounting for 366 million disability-adjusted life years and 17.8 million deaths in 2017.
Modifying cardiovascular disease risk factors, promoting prompt recognition of acute myocardial infarction symptoms and providing timely and appropriate medical response are necessary to address this public health issue.
What does this study add?
This study provides baseline information on current public knowledge of cardiovascular disease risk factors, symptom recognition and healthcare-seeking behaviour in Brazil. It demonstrates that lower education and socioeconomic status are consistent predictors of lower knowledge of cardiovascular disease and response to acute cardiac events.
How might this impact clinical practice?
This study identifies the need for further public education regarding cardiovascular disease risk factors, symptoms and appropriate response. These results can help guide future public health and health care initiatives in Brazil, a country undergoing an epidemiological transition.
Introduction
Cardiovascular disease (CVD) is the leading cause of disability and premature mortality globally, responsible for 366 million disability-adjusted life years (DALYs) and 17.8 million deaths in 2017.1 Furthermore, ischaemic heart disease (IHD) accounts for the majority of health lost to CVD in all regions of the world.2 The burden of CVD disproportionately affects those living in low/middle-income countries (LMIC), where cardiovascular conditions and risk factors are on the rise as a result of an ongoing epidemiological transition.2 Additionally, the mortality rate from CVD in LMIC is significantly above that in high-income countries.3 In Brazil alone, CVD is responsible for nearly one-third of total deaths and 14% of total DALYs.1
In response to the growing health impact of CVD, the WHO has set a target of a 25% reduction in CVD-associated premature mortality by 2025.4 Achievement of this target requires countries to make improvements along the entire continuum of care. This includes efforts to improve primary prevention by addressing CVD risk factors, timely and appropriate treatment of acute cardiovascular events such as acute coronary syndromes and evidence-based secondary prevention programmes to limit adverse long-term outcomes.5–7 Within this continuum, public knowledge of CVD risk factors, symptoms of acute cardiac events and appropriate bystander response is key to modifying health behaviours and improving health outcomes.8 9
Building on a similar programme in the USA,10 the Global HeartRescue project is a public health initiative that aims to improve access to and quality of care, and health outcomes, for acute cardiovascular events such as acute myocardial infarction (AMI) and sudden cardiac arrest. HeartRescue intends to foster local ownership of each country programme by engaging multisector stakeholders, including governments, medical professional societies, local healthcare providers, patients and families. The programme focuses on minimising critical delays to treatment by coordinating performance and outcomes measurement, education, training and the application of evidence-based best practices.
To inform the development of high-impact interventions in underserved communities in Brazil, a baseline survey was completed in three municipalities in eastern Brazil. This paper presents findings from the HeartRescue landscape assessment of public knowledge of CVD risk factors and AMI symptoms as well as cardiopulmonary resuscitation (CPR) and automated external defibrillator (AED) awareness and training. Results of a similar landscape assessment in three megacities in China and India have been previously published.11
Methods
Study design, setting and population
A cross-sectional population-based survey of knowledge, attitudes and practices pertaining to CVD risk factors, AMI symptoms, CPR and AED knowledge and training, and emergency service utilisation was conducted in three Brazilian municipalities: Padre Paraíso (PP), Poções (PC) and Vitória da Conquista (VC). VC was selected a priori as a potential HeartRescue intervention site in Brazil given the presence of willing and interested government and non-governmental partners. PP and PC were selected based on existing partnerships with local health leaders, policy-makers and research institutions. Summary of site-specific sociodemographic characteristics is presented in table 1.
Summary of site-specific sociodemographic characteristics
Data were collected from a non-institutionalised sample of adults aged 30 years and older, of both sexes, living in urban or rural areas of the selected municipalities through a structured household survey. Those physically or mentally unable to complete the surveys were excluded from the study. The research took place between October 2017 and December 2017 in PP and PC and between April 2019 and June 2019 in VC. The conduct and reporting of this study followed Strengthening the Reporting of Observational Studies in Epidemiology guidelines.12
Household survey
The study aimed to survey 962 individuals in PP, 1109 in PC and 1054 in VDC. The sample size for each location was defined using a formula for a single proportion from a finite population. The calculation took into consideration the population size, a 95% CI, an estimated error of 3% and a conservative expected proportion of an attribute of 50%. This proportion indicates a level of maximum variability observed in the population and yields the largest sample size given the different outcomes assessed in the survey.13
In VC, participants were selected in a three-stage sampling process. First, 40 census tracts (out of 152) were selected using probability proportional to size. In the second stage, households within each census tract were selected by systematic random sampling. Finally, an adult was randomly selected from a list of eligible residents built at the moment of interview with assistance of one of the household members, without regard to sex or age strata. In PP and PC, all census tracts were surveyed and interviewees were selected in a two-stage sampling strategy: random selection of households, considering the proportional distribution of households among each of the census tracts according to the 2010 Brazilian Census, followed by the selection of individuals within the households. In all three sites, up to three attempts at contacting the respondent were conducted. In case of refusal or failed attempts, a replacement household was selected at random within the same census tract.
The questionnaire used in the survey was developed by a core group of researchers and is published elsewhere.14 It was translated into Portuguese and pretested for content, design, readability and comprehension in neighbouring municipalities in Minas Gerais and Bahia. Modifications were made as necessary so that the questions were simple to understand and answer. In each municipality, trained research assistants conducted the surveys in the local language using computer-assisted personal interviewing software.
Variables
Outcomes
CVD and AMI knowledge were assessed through open-ended questions. The respondent’s ability to identify CVD risk factors (ie, smoking, excess weight, physical inactivity, excessive alcohol consumption, high cholesterol, hypertension and elevated blood glucose) and AMI symptoms (ie, jaw, back, neck, shoulder, arm, hand pain/numbness; chest pain/discomfort; vomiting/nausea; shortness of breath; sweating; weakness/fatigue/dizziness; and loss of consciousness/impaired cognitive function) was evaluated. Responses coded as ‘other’ were not analysed in the current study.
Participants were considered to be aware of CPR if they had heard of CPR prior to the interview. Those who recognised an AED picture and reported that it could be used for restoring the heart to its normal rhythm with an electric shock were considered knowledgeable about AEDs.
Predictors
Predictors included gender (male/female), age group (30–39; 40–49; 50–59; and ≥60), highest level of education (no formal education; primary or secondary school; and high school or higher) and economic classification (lower, middle and upper). Economic class was determined using the Brazilian criteria of economic classification, a composite index based on household ownership of capital goods, number of household servants, head of the household education level, sources of household water and whether the street the residence was located on was paved.15
Analysis
Data on CVD risk factors, AMI symptoms, CPR awareness and AED knowledge are described as survey-weighted percentages of the sampled populations. Survey weights were calculated to account for differential selection probabilities and a poststratification procedure was performed to approximate the age, sex and rural/urban composition of data included in the 2010 Brazilian National Census, and to account for non-response.
Models were created to assess the sociodemographic determinants of CVD, AMI, CPR, and AED knowledge. For CVD and AMI knowledge, a Poisson model with a log link function was used to assess knowledge based on the number of risk factors (0–7) and symptoms (0–7) reported by each participant. Logistic regression models were used to examine the determinants of CPR awareness and AED knowledge since these were coded as dichotomous variables. Separate models were run for each municipality. The results of these models are reported in online supplementary tables 1-S4. Missing data were excluded from analysis. Online supplementary table S5 lists the number of missing responses for each variable included in the study.
Supplemental material
Statistical analyses were conducted in Stata SE V.13.116 using the svyset command, with a significance level of 5%. Figures were produced in R V.3.4.417 using the ggplot2 package.18
Patient and public involvement
This study served as one mechanism to obtain information from the public as it pertains to future HeartRescue interventions. There was no substantive community engagement prior to study implementation with the exception of some sensitisation activities to ease surveyor entry/acceptance into households.
Results
Demographics
Overall, 3035 surveys were completed; 962 in PP, 1019 in PC and 1054 in VC. table 2 shows the demographic and health characteristics of the study participants. Gender and age distributions were similar across sites. Greater than half of respondents were female (65.1% in PP; 69.8% in PC; 67.3% in VC) and about one-third of respondents were 60 years of age or more (37.9% in PP; 35.9% in PC; 33.1% in VC). Compared with the entire population aged 30 or older, men and middle-aged individuals were under-represented in the study in all municipalities. Approximately half of the respondents had the lowest level of education in PP (51.3%) and PC (48.1%), while in VC this proportion was considerably lower at 22.6%. Most of the participants in PP (71.9%) and PC (58.6%) were classified as lower socioeconomic class whereas the largest proportion of respondents in VC were categorised as middle socioeconomic class (44.7%). Of the study population in each location, around 12% were smokers. Prevalence of self-reported hypertension varied from 35.3% in PC to 40.3% in PP, and prevalence of self-reported diabetes ranged from 8.7% in PP to 13.3% in VC (table 2).
Sociodemographic and clinical characteristics of participants
CVD risk factors
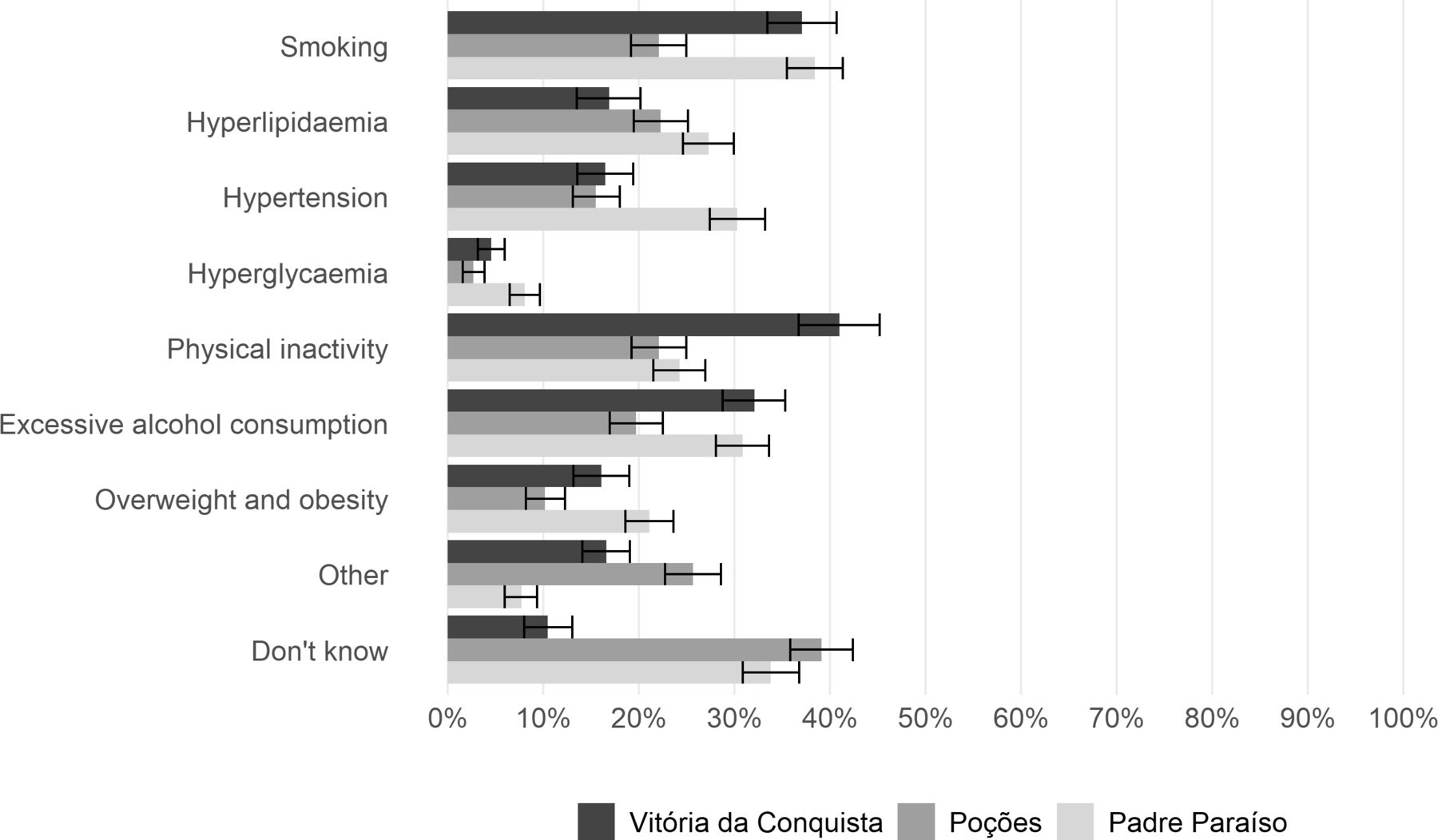
Approximately one-third of respondents across all sites were not able to identify at least one key CVD risk factor. Participants in PC were less knowledgeable compared with the other locations—45.6% were unable to report any risk factor for heart disease. Overall, 46.3% indicated one to two, 23.3% three to four and 2.7% five or more risk factors. In general, the most common risk factors identified were physical inactivity, smoking and excessive alcohol consumption. Hyperglycaemia and obesity were the least-reported CVD risk factors across all study sites (figure 1).

Risk factors for cardiovascular disease identified by respondents.
Multivariate regression analysis (online supplementary table S1) indicated that education level was independently associated with CVD risk factor knowledge in all sites (p<0.05). Higher levels of education were associated with a statistically significant increase in ability to name a larger number of CVD risk factors, with the most pronounced effect for those with a high school/university diploma in PC (incidence-rate ratio (IRR) 2.52, 95% CI 1.90 to 3.32). Older age correlated with naming fewer risk factors in VC (IRR 0.69, 95% CI 0.58 to 0.81) and middle and upper socioeconomic status were associated with increased knowledge of CVD risk factors in PC.
AMI symptoms
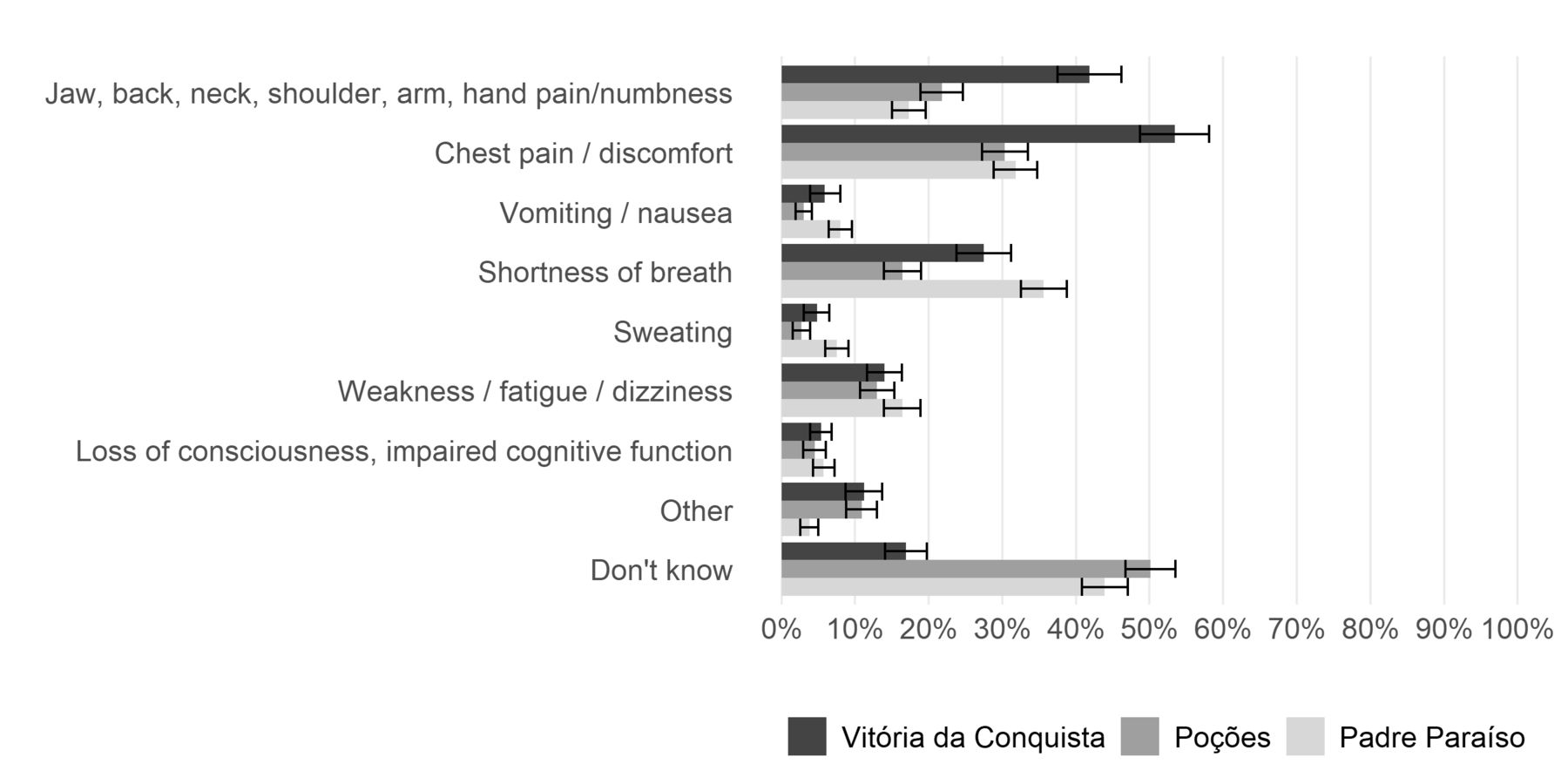
Across sites, 75% of respondents were able to name at least one AMI symptom, with the largest proportion seen in VC (80.5%), followed by PP (54.2%), and PC (48%). Out of all participants, 26.3% were able to report one, 33% two and 15.8% recognised three or more symptoms. Chest pain, shortness of breath and referred pain/numbness were the most commonly identified symptoms of AMI in all sites. In VC, over 58% of respondents identified chest pain as an AMI symptom, and just under half (41.8%) identified referred pain/numbness. These proportions were significantly higher than those in PP and PC. In PC, only 16% of participants indicated shortness of breath as a symptom, compared with 35.6% in PP and 27.4% in VC. Other symptoms such as vomiting/nausea, sweating and loss of consciousness/impaired cognitive function were mentioned least frequently in all locations (figure 2).
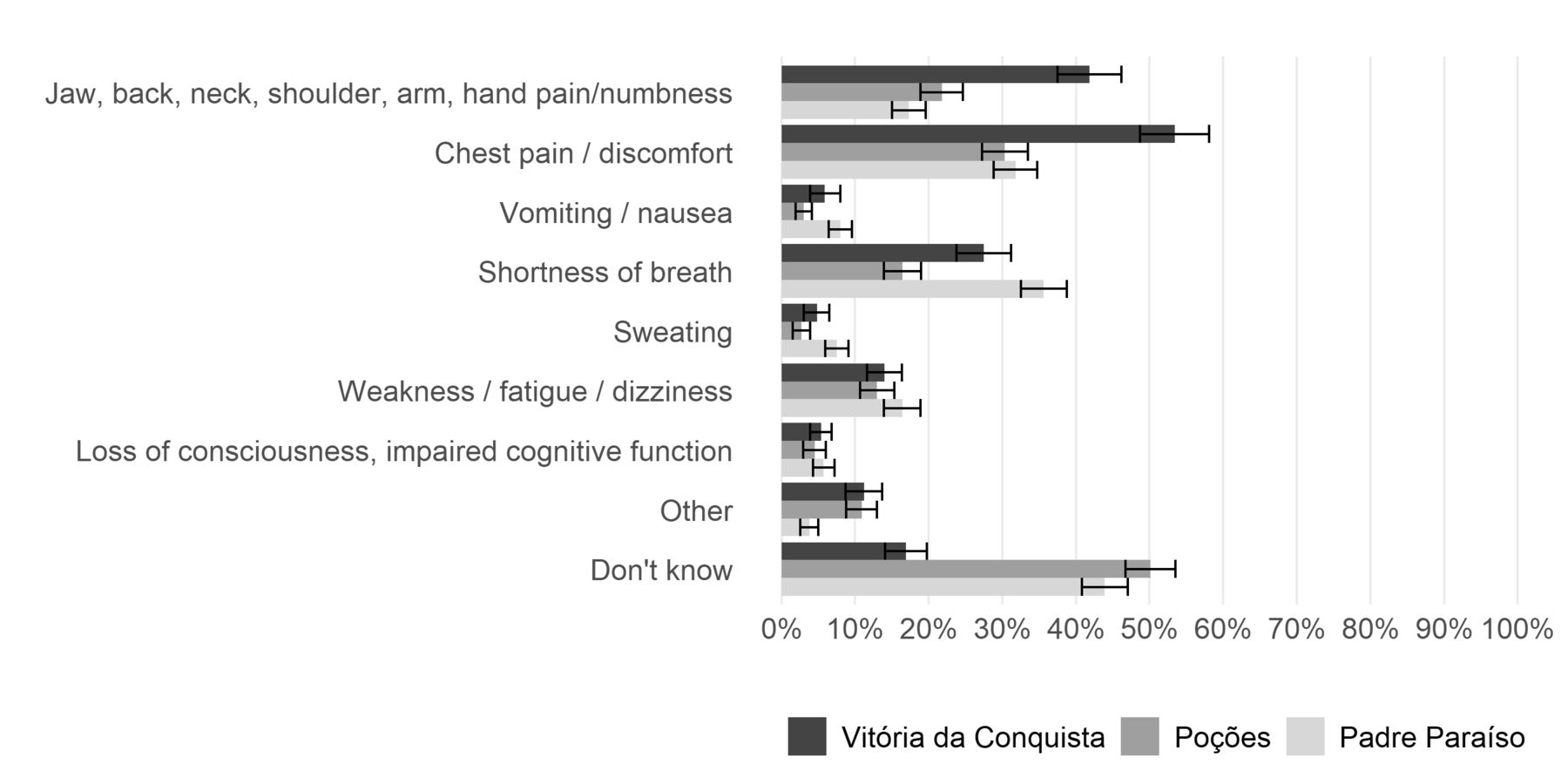
Heart attack symptoms identified by respondents.
Education was independently correlated with AMI knowledge in all three cities. High school or college education was associated with the ability to name a greater number of AMI symptoms, especially in PC (IRR 2.34, 95% CI 1.78 to 3.08). Those in middle and upper socioeconomic classes were also able to name more symptoms in PC and VC, but not in PP. Female gender was associated with increased knowledge of AMI symptoms in VC only (IRR 1.24, 95% CI 1.13 to 1.37; online supplementary table S2).
CPR awareness and training
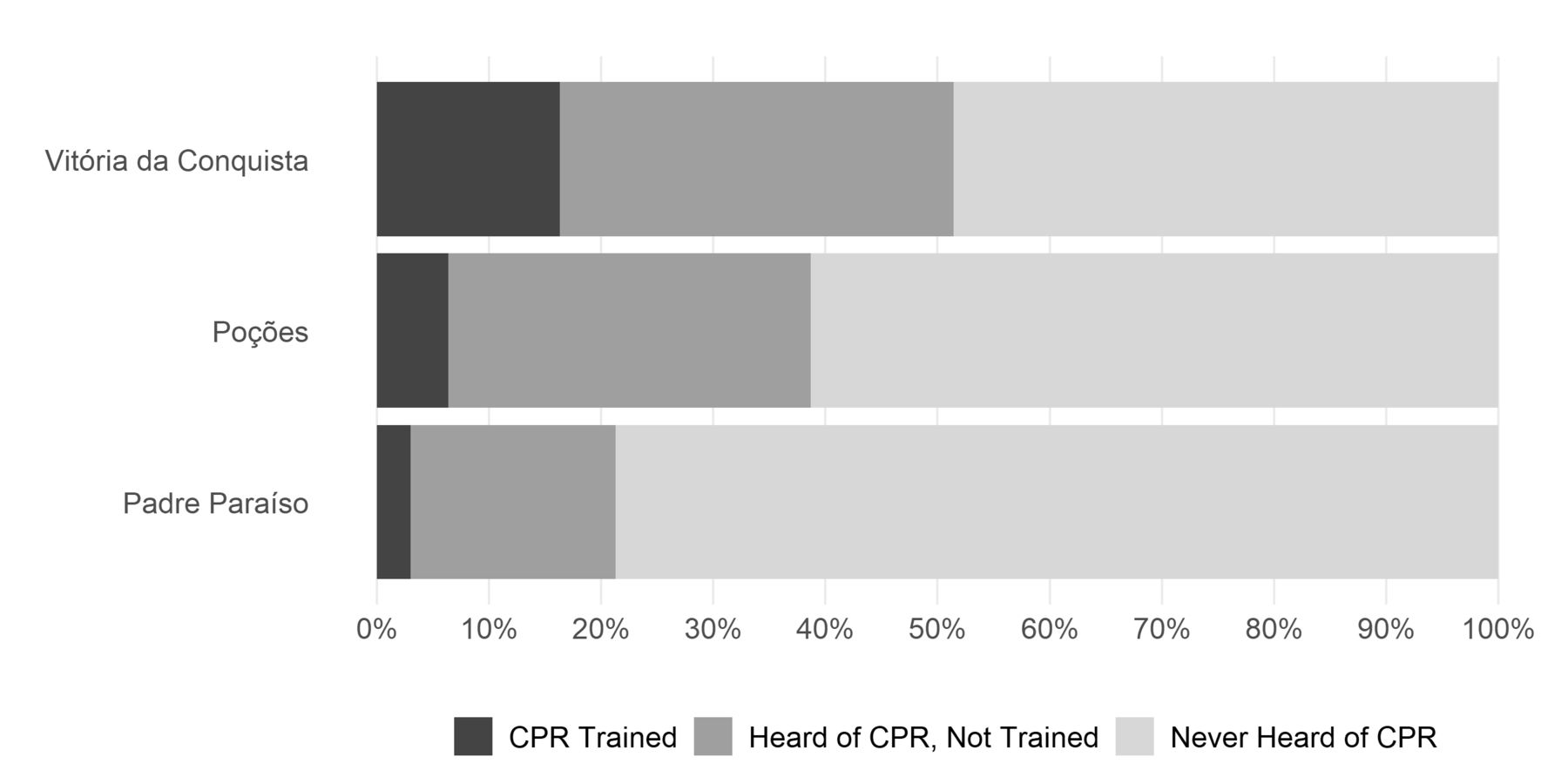
The proportions of CPR-aware and CPR-trained individuals were greatest in VC, where 51.4% had heard of CPR and 16.3% had received CPR training. In PP and PC, the majority of respondents had never heard about CPR prior to the interview (78.7% and 61.3%, respectively). Only 3% of participants in PP and 6.4% in PC reported any prior CPR training (figure 3). Those with a high school or university diploma were more likely to have heard about CPR in PP (OR 2.55, 95% CI 1.39 to 4.70) and PC (OR 2.43, 95% CI 1.44 to 4.08). Controlling for other sociodemographic variables, higher socioeconomic levels were associated with CPR knowledge in PP and VC, but not in PC. Women from PC were less likely to be aware of CPR (OR 0.71, 95% CI 0.52 to 0.98; online supplementary table S3).
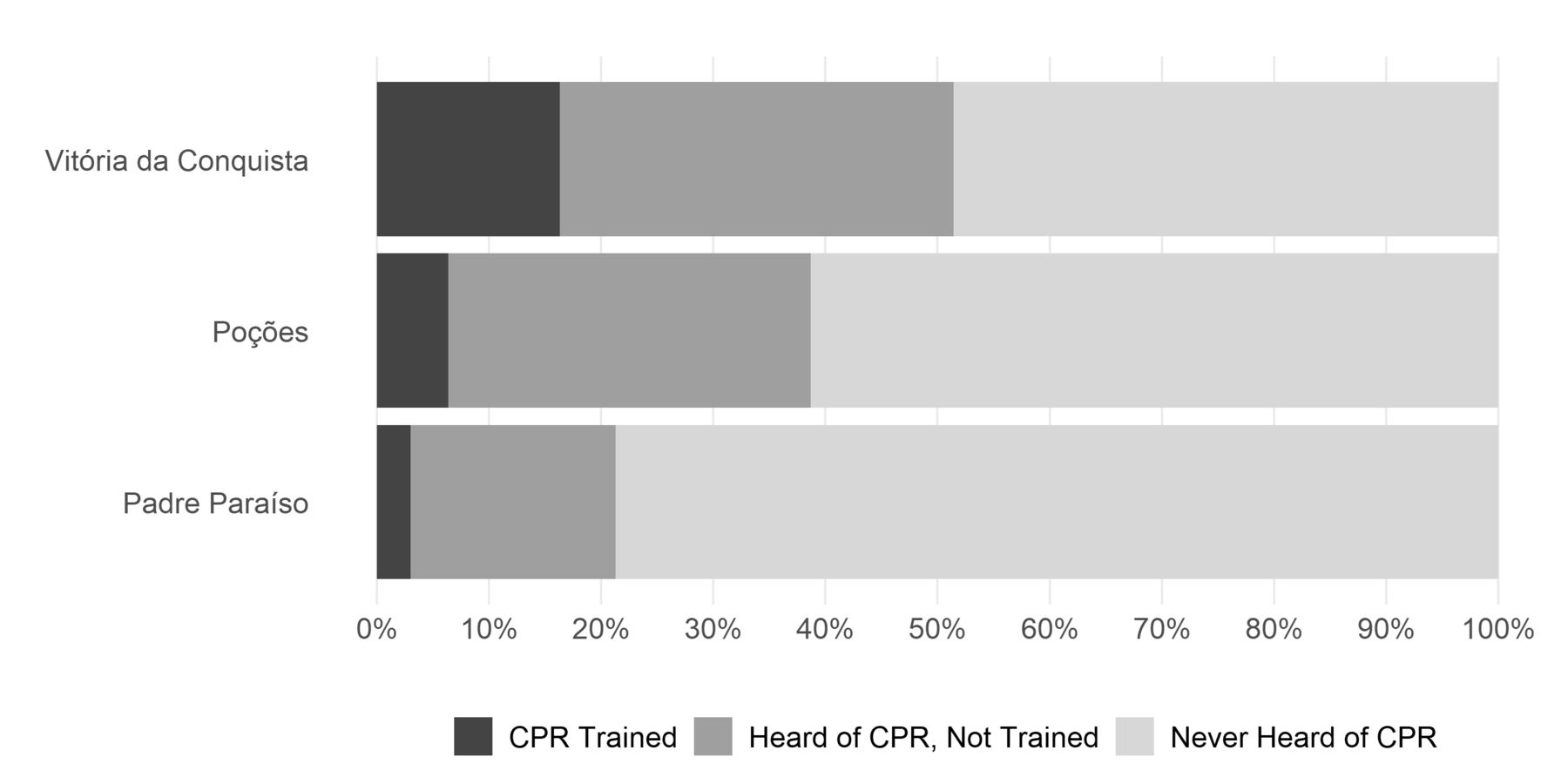
Cardiopulmonary resuscitation (CPR) awareness and training.
AED knowledge
In all cities, less than half of respondents were able to recognise an AED after seeing a picture of the device—22.1% in PP, 24.8% in PC and 44.6% in VC (figure 4). However, of those who could recognise an AED, the majority of respondents at all sites were able to indicate that an AED is used to return the heart to its normal rhythm with an electric shock.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Automated external defibrillator (AED) recognition and knowledge of proper use.
Results from the logistic regression (online supplementary table S4) indicated that female sex, age ≥60 years, no formal education and lower economic classification were associated with lower likelihood of recognising an AED in all locations.
Discussion
This is the first published survey of public knowledge of CVD risk factors, AMI symptoms and response to acute cardiac events in Brazil. Overall, we found low public knowledge of CVD risk factors and AMI symptoms in addition to low rates of CPR and AED knowledge and training at all study sites.
Compared with public knowledge of CVD risk factors and AMI symptoms in both developed and developing countries, respondents in this study were overall less likely to have knowledge of any CVD risk factor, and generally less knowledgeable of common CVD risk factors, including hyperglycaemia, smoking, physical inactivity and overweight/obesity.11 19 20 Furthermore, CPR knowledge was lower than what has been reported in Beijing, Shanghai,11 and other international contexts.9
An important finding from this investigation is that lower levels of education and lower socioeconomic status were consistent predictors of lower knowledge across all categories included in this survey. This is important as accurate knowledge is a key component of health behaviour change and appropriate care seeking.21 Furthermore, the association between lower education and socioeconomic status with less knowledge of CVD risk factors,19 AMI symptoms9 22–24 and CPR and AED use9 is consistent with prior international studies. With regards to knowledge of CPR and AEDs, it was interesting to note that the majority of respondents who could recognise an AED also knew its use, while a much smaller proportion of those who had heard of CPR had received CPR training. This may reflect a difference in local education programmes and resources and merits further investigation.
These results provide important insights into the challenges faced by a country undergoing an epidemiological transition. Along with a growing burden of chronic conditions, the sites included in this study present significant heterogeneity in socioeconomic status, rural versus urban living environment and public knowledge of CVD risk factors, symptoms and bystander response. For example, the overall rates of knowledge of CVD risk factors was low compared with high-income country settings; however, the knowledge levels of AMI symptoms in VC exceeded those of disadvantaged groups within the USA.25 The variation seen among sociodemographic groups across different locations indicates the need for location-specific data and contextual information in order to identify gaps in the cascade of care and design locally relevant mechanisms and interventions.26
Although this study does not identify mechanisms for improving health outcomes for individuals who suffer acute cardiac events such as AMI, it clearly notes that improvements need to be made on the demand side to improve recognition of both disease risk and acute cardiac events as a first step in the treatment cascade. Many potential interventions exist, including the creation of educational programmes and support groups, which could be implemented in a variety of settings, such as primary and secondary schools, worksites, healthcare facilities and religious organisations.3 8 21 27 In these Brazilian sites, specifically, where a longstanding community-based healthcare structure and Community Health Worker (CHW)-led service provision is in place through the Family Health Program (FHP), home visits can also be an effective platform for education and intervention.28 CHW is reported to be trusted and effective in reaching families and providing ongoing technical assistance while also having a unique understanding of the experience, language, culture and socioeconomic reality of the communities that they serve.29 However, further work is needed to understand the capacity of the FHP and other potential educational venues, including supportive technologies for public health interventions, to address the observed knowledge gap and associated CVD epidemic in the selected resource-constrained sites.
The study results should be considered in the context of certain limitations. The population included in this study may not be representative of other Brazilian populations, particularly of larger metropolitan areas. As well, this study does not address current emergency services utilisation by the population or the preparedness of the healthcare system in this region to provide timely and high-quality acute care, inpatient care or rehabilitation services for patients suffering from IHD. Further work is therefore needed to evaluate the quality of care available and the capacity of the system to provide adequate services along the chain of survival for IHD.
Conclusions
Overall public knowledge of CVD risk factors and symptoms, as well as knowledge of appropriate CPR and AED use was low in selected Brazilian municipalities. Chest pain was the most commonly identified symptom of a heart attack. Higher education and socioeconomic status were consistent predictors of public knowledge of CVD risk factors, symptoms and appropriate response. To address the burden of morbidity and mortality caused by IHD in Brazil, further work is needed to identify effective avenues for intervention along the continuum of prevention, symptom recognition and bystander response.
References
Footnotes
Twitter @EBartlettMD
Contributors HCD and LSF conceptualised the study and developed the survey instrument. LSF, DVC, CKJ and SW contributed to development of the survey instrument, data collection, and data management, verification and analysis. DSM and FACV managed data collection activities. ESB and LSF performed the analysis. ESB wrote the first draft of this manuscript. All authors read, contributed to and approved the final manuscript.
Funding Funding was provided by the Medtronic Foundation.
Disclaimer The funder had no role in study design, data collection, data analysis, decision to publish or preparation of the manuscript.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval Ethical approval was obtained from the University of Washington and local institutional review boards in Padre Paraíso (University Hospital of the University of Minas Gerais), Poções (Federal University of Bahia), and Vitória da Conquista (Federal University of Bahia). Written informed consent was obtained prior to participating in the study and recorded in the survey software. Illiterate patients had consent information presented orally and oral consent was documented in the presence of a witness.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Deidentified participant data are available upon reasonable request from the Institute for Health Metrics and Evaluation at the University of Washington.