Article Text

Abstract
The use of fractional flow reserve (FFR) in guiding revascularisation improves patient outcomes and has been well-established in clinical guidelines. Despite this, the uptake of FFR has been limited, likely attributable to the perceived increase in procedural time and use of hyperaemic agents that can cause patient discomfort. This has led to the development of instantaneous wave-free ratio (iFR), an alternative non-hyperaemic pressure ratio (NHPR). Since its inception, the use of iFR has been supported by an increasing body of evidence and is now guideline recommended. More recently, other commercially available NHPRs including diastolic hyperaemia-free ratio and resting full-cycle ratio have emerged. Studies have demonstrated that these indices, in addition to mean distal coronary artery pressure to mean aortic pressure ratio, are mathematically analogous (with specific nuances) to iFR. Additionally, there is increasing data demonstrating the equivalent diagnostic performance of alternative NHPRs in comparison with iFR and FFR. These NHPRs are now integral within most current pressure wire systems and are commonly available in the catheter laboratory. It is therefore key to understand the fundamental differences and evidence for NHPRs to guide appropriate clinical decision-making.
- coronary pressure
- fractional flow reserve
- coronary physiology
- coronary intervention (PCI)
- angina - unstable
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- coronary pressure
- fractional flow reserve
- coronary physiology
- coronary intervention (PCI)
- angina - unstable
Introduction
Ischaemic heart disease remains a leading cause of morbidity and mortality.1 Myocardial revascularisation is an important treatment modality for patients with obstructive coronary artery disease (CAD), with use of invasive and non-invasive functional modalities improving the selection of patients that would most likely benefit. The use of invasive pressure-based functional assessment has now permitted identification of lesion-level ischaemia to better guide revascularisation strategies. Fractional flow reserve (FFR) is the most established of these tools and permits the measurements of pressure gradients across a lesion. FFR measurements are acquired during hyperaemia to minimise the influence of the coronary microcirculation. Despite a robust body of evidence supporting its use, clinical uptake of FFR remains low and highly variable between healthcare systems.2 Reasons for poor uptake include the perceived additional procedural cost and time, as well as the discomfort to patients with administration of hyperaemic agents.3 This has led to the development of alternative invasive non-hyperaemic pressure ratios (NHPR) that may improve the uptake of physiologically-guided revascularisation.
The instantaneous wave-free ratio (iFR; Philips Volcano Corporation, San Diego, California, USA) is a diastolic-only index and was the first specific NHPR to become commercially available (figure 1). While there was some initial scepticism that an NHPR could perform as well as FFR,4 two large randomised controlled trials have demonstrated its non-inferiority to FFR in the assessment of intermediate lesions.3 5 An increasing body of evidence has supported its clinical utility and iFR was recently incorporated into the European guidelines on myocardial revascularisation for use in the functional assessment of patients with stable angina (class I recommendation, level of evidence A).6 Following the arrival of iFR to market, other NHPRs have since been developed by competing companies and are now commercially available (figure 2).7 8 However, there are fundamental differences between each of these indices, relating to the sampling period of the cardiac cycle from which they are derived and data justifying their use, which has largely been provided by demonstrating non-inferiority and equivalence to iFR. This review aims to assist cardiologists in understanding the NHPRs available and the data supporting their use to guide appropriate clinical decision-making. This review also describes the methodological considerations and clinical interpretation in their use in different lesion and patient subsets.
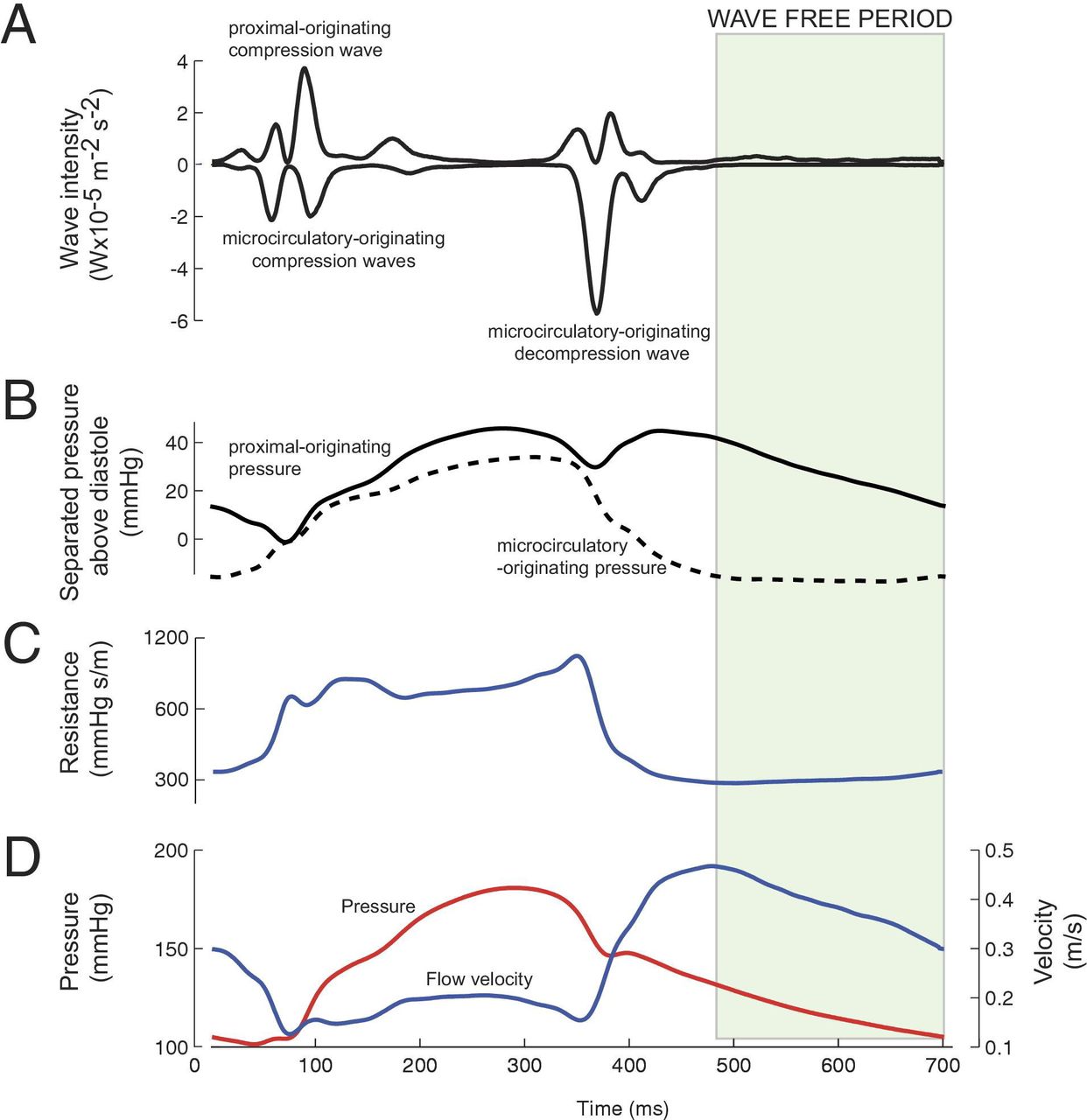
The physiological derivation of the wave-free period (WFP). Wave intensity analysis (A) demonstrates a WFP (green shaded area), a segment in the cardiac cycle when there is minimal microcirculatory originating pressure (B), minimal and constant coronary resistance (C) and therefore, coronary flow velocity (blue) and pressure (red) are both linearly related (D). Reproduced from Sen et al.21

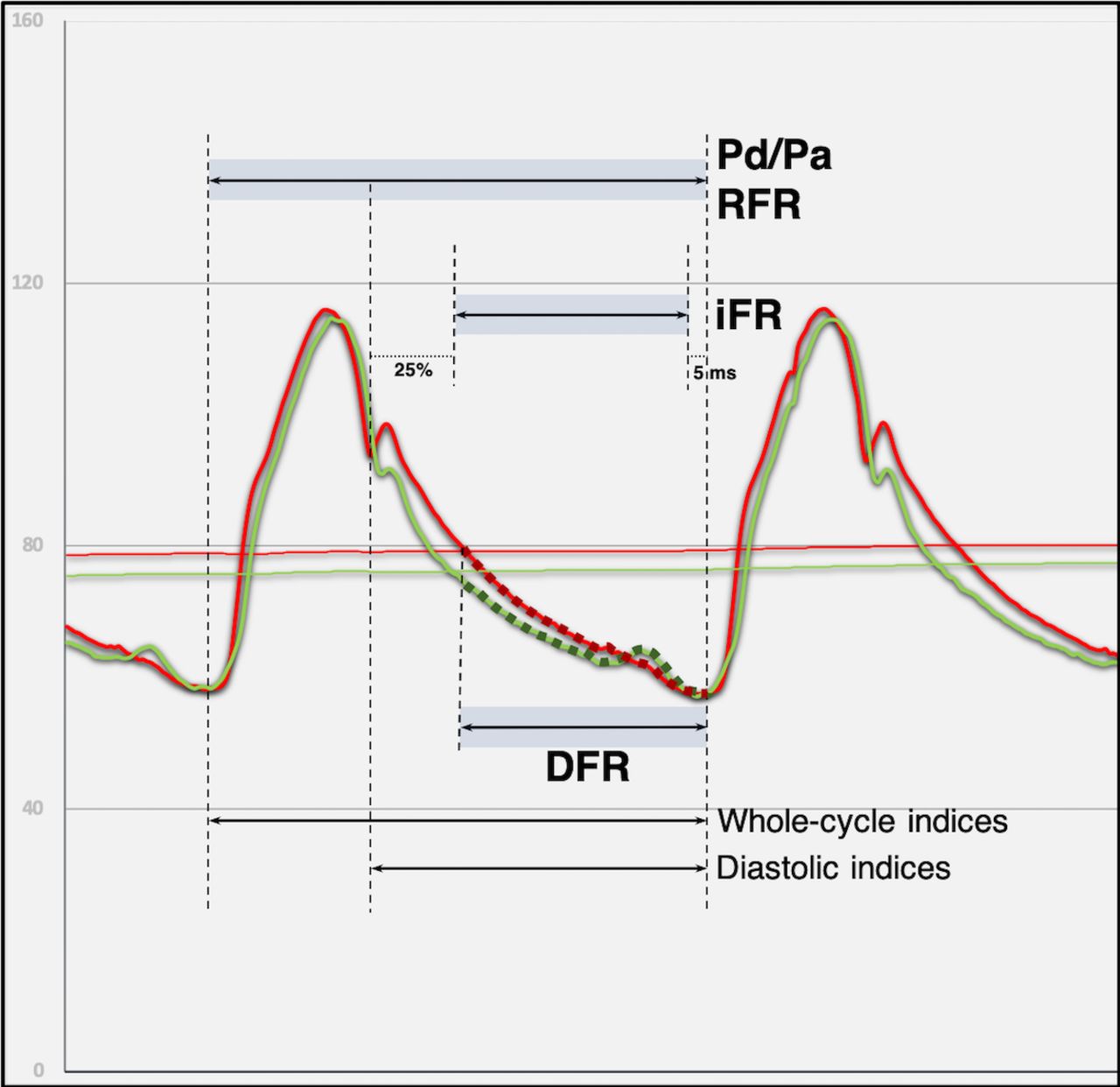
Schematic representation of the commonly available non-hyperaemic pressure ratios and the periods of the cardiac cycle from which they are calculated. DFR, diastolic hyperaemia-free ratio; iFR, instantaneous wave-free ratio; Pd/Pa, ratio of mean distal coronary artery pressure to mean aortic pressure in the resting state; RFR, resting full-cycle ratio.
Physiological basis of resting pressure-based indices
FFR is an invasively determined index, derived as a method for assessing the functional impact of coronary stenosis. It is defined as the maximal blood flow to the myocardium in the presence of a stenosis in the supplying coronary artery, divided by the theoretical normal maximal flow in the same distribution.9 This can be calculated by measuring the ratio of the mean distal coronary artery pressure (Pd; distal to the stenosis) to the mean aortic pressure (Pa) during maximal microvascular vasodilatation. Maximal vasodilatation using hyperaemic agents minimises and maintains constant microcirculatory resistance. During these conditions, pressure is proportional to coronary flow—thus allowing the measurement of pressure gradient across a lesion without being confounded by pressure changes in the distal microcirculatory bed. FFR was brought into clinical practice after its validation by Pijls and colleagues9 and has been robustly validated and tested in the subsequent two decades.10–16 Today it is considered the ‘gold standard’ and is a class IA recommendation in revascularisation guidelines.6
Rise of diastolic non-hyperaemic indices—wave intensity analysis and the concept of iFR
Coronary microvascular resistance fluctuates in a phasic pattern, due to the variable interaction between the myocardium and microvasculature, with the latter being compressed and decompressed during the cardiac cycle.17 18 Study into the relationship between coronary pressure and flow led to the identification of a ‘wave-free period’ (WFP)—a specific period during diastole that is free from the effects of forward and backward wave energies. This WFP permitted the measurement of coronary pressure during a period where microcirculatory resistance is constant—and not necessarily minimal—as was previously considered necessary.19–21 Physiologically, this mimics the constant microcirculatory resistance induced by adenosine during hyperaemic state whereby measured pressure is proportional to flow. Application of these principles paved an opportunity for a hyperaemia-free index and the subsequent development of iFR.
iFR and other NHPRs
A recent post-hoc analysis compared iFR against other defined resting indices using raw data from pressure waveforms, including diastolic and whole-cycle indices.22 Indices compared included diastolic pressure ratio (mean Pd/Pa over the entire diastolic period), ratio of mean Pd to mean Pa (Pd/Pa) and Pd/Pamin (defined as the minimum value of the filtered point by point ratio of Pd and Pa for a single heart cycle). The investigators found the Spearman’s correlation coefficient for all diastolic indices against iFR to be >0.99, leading the authors to conclude that all diastolic resting indices were numerically identical irrespectiveof restriction to the WFP. Similarly, the correlations between resting Pd/Pa and Pd/Pamin were 0.95 and 0.97, respectively.
New NHPRs which exploit these correlations have since become commercially available (table 1). This includes diastolic hyperaemia-free ratio (DFR; Boston Scientific, Natick, Massachusetts, USA) and resting full-cycle ratio (RFR, Abbott Vascular, Santa Clara, California, USA). DFR uses the mean Pd/Pa calculated over the period in diastole defined as that during which arterial pressure is negatively sloped and below the mean arterial pressure. This method allows approximation of diastole without the need to identify the dichrotic notch, which can be technically challenging in damped traces.8 23 In contrast, RFR is derived from 4 to 5 consecutive cardiac cycles by calculating the minimum Pd/Pa within the cardiac cycle, after smoothing of the instantaneous Pd/Pa trace.7 In the RFR validation study, this point was located within diastole in 88% of cases.7
Currently available non-hyperaemic pressure ratios (NHPRs)
There are now several large studies which demonstrate that the strong correlations between iFR and other NHPRs present numerically identical results and therefore a widely shared view is that a class effect should be considered.8 22 24 However, it merits consideration that apart from iFR, other NHPRs have not been scrutinised in prospective trials.
Methodological considerations
There are some practical considerations that are important to account for when using NHPRs. While modern pressure wires provide high fidelity measurements, pressure drift can be a source of error which may inadvertently result in the misclassification of lesions. Since FFR mandates the use of hyperaemic agents, transtenotic pressure gradients are greater than those measured using NHPRs. This means that small pressure drifts are likely to have a greater impact on NHPRs than they would on FFR. Thus, stringent measures of all NHPRs should be taken in order to minimise drift and lesion misclassification. This includes adherence to the standardised practice, for example, ensuring no guide catheter dampening, no blood leaking (causing pressure loss) around the introducer and no contrast medium within the guiding catheter.
Another potential consideration in using NHPR is heart rate (HR) during pressure wire assessment. Increasing the HR likely affects all indices (usually by lowering the readings) which may result in the misclassifications of lesions.25 The period in the cardiac cycle from which NHPRs are derived may be additionally relevant in tachycardic patients, as it may adversely affect diastolic-only indices to a greater extent due to the relative shortening of diastole.
Notwithstanding all the above considerations, there are error margins with all invasive pressure indices, which may result in the reclassification of lesions. Evidence has demonstrated a risk continuum where lower FFR values are associated with higher rates of clinical events.26 Therefore, as with hyperaemic pressure indices, NHPRs should not simply be treated as dichotomous tools, but rather clinical judgement should be exercised in their interpretation.
Current evidence for the use of available technologies
Instantaneous wave-free ratio
The validation of iFR originated from multiple studies demonstrating concordance between iFR and FFR for the assessment of intermediate severity coronary artery stenosis. An iFR cut-off ≤0.89 was shown to best predict FFR ≤0.80.27–30 However, the VERIFY II trial did challenge the correlation of iFR with FFR (r=0.73, p=0.001) finding a misclassification rate of 21% in lesions using iFR compared against FFR (area under the receiver operating characteristic curve [ROC AUC] 0.85); warranting studies to assess clinical outcomes associated with iFR.31 Consequently, non-inferiority of iFR compared with FFR was demonstrated in two large prospective randomised trials: DEFINE-FLAIR and SWEDEHEART.3 5
DEFINE-FLAIR randomly allocated participants in a 1:1 ratio to undergo either iFR-guided or FFR-guided revascularisation. The study included both stable and non-culprit vessels in patients presenting with acute coronary syndromes (ACS). The primary endpoint of major adverse cardiac events at 1 year was not different between the two groups (6.8% vs 7.0%, HR=0.95, p=0.78). Expectedly, the procedural time was significantly shorter in the iFR group (40.5 vs 45.0 min, p<0.001) and the number of patients reporting adverse procedural symptoms was significantly higher in the FFR group secondary to vasodilator use (3.1% vs 30.8%, p<0.001). The SWEDEHEART trial randomised a large cohort to iFR versus FFR guided revascularisation with similar results at 1-year follow-up. The primary endpoint of major adverse cardiovascular events (MACE) occurred in 6.7% of iFR-guided versus 6.1% in FFR-guided percutaneous coronary intervention (PCI; HR=1.12, p=0.53). Adverse procedural symptoms were again higher in the FFR cohort (3.0% vs 68.3%, p<0.001). A subgroup analysis from the DEFINE-FLAIR trial explored the risk of left anteriordescending artery (LAD) lesion deferral based on iFR.32 The results from this substudy suggested iFR-guided deferral in the LAD led to a lower MACE rate at 1-year follow-up compared with FFR (2.44% vs 5.26%, HR 0.46, p=0.04). This composite endpoint was driven by statistically higher unplanned revascularisation and numerically higher myocardial infarction related to the LAD in the FFR arm. However, this post-hoc analysis was underpowered to validate differences among subgroups. This study also did not individually explore the outcomes of the circumflex and right coronary artery (RCA). The two studies were limited by low-risk patient demographics; with an average age below 70 years and the majority of patients undergoing intervention for stable CAD. Furthermore, both RCT’s were powered only to evaluate non-inferiority between the modalities as approximately 80% of iFR and FFR results are concordant.
There is no long-term randomised data available on iFR outcomes at this stage, with the above trials being limited by a follow-up period of 1 year. Nonetheless, the 2018 European Society of Cardiology guidelines on myocardial revascularisation have incorporated a level 1A recommendation for the use of iFR in the haemodynamic assessment of intermediate-grade stenosis.6
Resting full-cycle ratio
RFR uses the maximal relative pressure difference over the entire cardiac cycle and is not limited to diastole. RFR was recently shown to be diagnostically equivalent to iFR in the VALIDATE-RFR study.7 This retrospective study derived an optimal cut-off ≤0.89 using receiver operator curve analysis with the clinically accepted FFR cut-off ≤0.80. Using this cut-off, RFR correlated very highly with iFR (R2=0.985, p<0.001) with high diagnostic equivalence (mean difference −0.002, p=0.03). Both RFR and iFR moderately correlated with FFR (R2=0.557 vs 0.540 with p<0.001 for both correlations). Subsequently, RE-VALIDATE RFR provided prospective analysis of RFR compared with iFR, showing similar levels of equivalence.33
While coronary perfusion is predominantly diastolic, it is recognised that the RCA perfuses in systole to a greater degree than in the left coronary artery.34 35 This may be attributable to the thinner-walled right ventricle which results in less systolic compression compared with the left ventricle. In addition, compared with the left coronary artery, the RCA has a smaller ‘diastolic suction wave’ which is responsible for accelerating diastolic coronary blood flow. In VALIDATE-RFR it was observed that the lowest Pd/Pa ratio was outside of the diastolic period in 12.2% of patients.7 This observation was greater in the RCA than the left coronary system; with the sensitivity of both RFR and iFR notably lower in the RCA. A reduced sensitivity of iFR compared with FFR has previously been observed in the RCA (figure 3).36 37 This raises the important question as to whether NHPRs and in particular diastolic-only indices are physiologically less-suited for assessment of lesions in the RCA. Further research is warranted to evaluate if there is a benefit to using whole-cycle NHPRs such as RFR or Pd/Pa in the assessment of RCA lesions.
{kind=link}
{kind=link}
{kind=link}
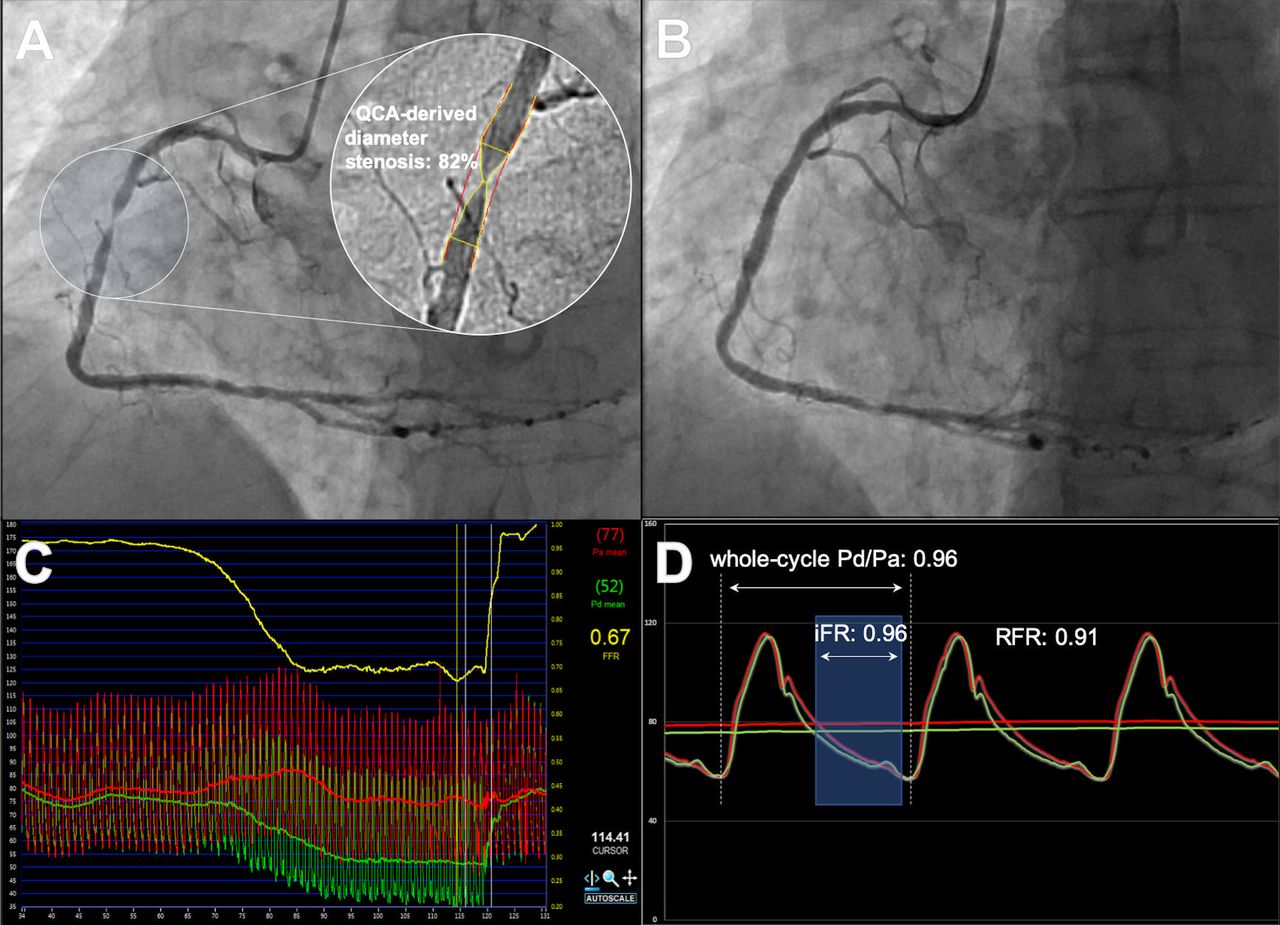
Representative case of significant discordance between hyperaemic and non-hyperaemic pressure ratios (NHPRs). Pressure wire study was performed in a severe stenosis in the right coronary artery (A) which was subsequently treated with 3.5 mm×12 mm everolimus-eluting stent (B). There was a notably positive fractional flow reserve at 0.67 (C) with negative NHPRs (D) including resting full-cycle ratio (RFR; 0.91), whole-cycle Pd/Pa (0.96) and instantaneous wave-free ratio (iFR; 0.96). Reproduced from Michail et al37. Pd/Pa, ratio of mean distal coronary artery pressure to mean aortic pressure in the resting state.
Diastolic hyperaemia-free ratio
DFR is a diastolic index that uses average Pd/Pa within an approximated diastole over five consecutive cycles. In a post-hoc analysis of 833 patients from the VERIFY II and CONTRAST studies, DFR has been shown to be numerically equivalent to iFR across 893 lesions (combined difference with iFR for DFR −0.006±0.011, R2=0.993, accuracy 97.6%).8 Another study similarly demonstrated significantly high correlations between both DFR and RFR with iFR.24 In this study, deferred vessels with retrospective iFR, DFR and RFR ≤0.89 all showed significantly higher rates (iFR, 9.5% vs 2.1; DFR, 7.5% vs 2.2%; RFR 6.4% vs 2.2%; p<0.001 for all) of the composite endpoint (cardiac death and target vessel failure).
Resting whole-cycle Pd/Pa
In view of the recent interest in NHPRs, there has been a resurgence of interest in the use of resting Pd/Pa as it is not vendor-specific, is widely available and has been shown to strongly correlate with FFR. The RESOLVE study initially showed both iFR and resting Pd/Pa (using the accepted cut-off value of ≤0.91) to have an overall accuracy of approximately 80% using FFR as the gold standard.27 The diagnostic accuracy of resting Pd/Pa compared with FFR was further confirmed on meta-analysis.38 Another study has shown resting whole cycle Pd/Pa to correlate highly with iFR (r=0.970, p<0.001) and with increases in anatomic and haemodynamic severity.39 The authors demonstrated that patients with resting Pd/Pa≤0.91 had significantly higher rates of 2-year MACE (8.7% vs 1.5%, p=0.003). However, iFR appears to be more sensitive to the differences in stenosis severity.29 While resting whole-cycle Pd/Pa has excellent agreement with iFR, its overall strength lies in its universal availability independent of specific vendors.
Special patient and lesion subgroups
Serial lesions
In the setting of serial lesions, the accurate physiological assessment of each individual stenosis is challenging due to haemodynamic interdependence.40 Each lesion increases the total vessel resistance with a consequent reduction in flow. Furthermore, each stenosis can lead to a change in local flow conditions by causing laminar flow to become turbulent, which in turn further reduces the pressure at that point. It is suggested that hyperaemia augments these altered flow conditions by increasing the pressure-velocity gradient across each lesion.41 In contrast, at rest flow is maintained at a constant and the interplay between stenoses is lessened. As such, it has been proposed that NHPRs may be less prone to error than hyperaemic indices in the evaluation of serial stenoses and diffuse disease.42
The utility of iFR in the setting of serial lesions was demonstrated in a study of 32 coronary arteries that were interrogated using an automated iFR pullback. Virtual stenting was performed to the areas of high iFR intensity loss and an expected post-PCI iFR calculated. There was a small mean difference and strong correlation between the expected and observed post-PCI iFR (r=0.97, p<0.001).43 The ability of iFR pullback to reliably predict post-PCI physiology was also demonstrated in the primary results of the international multicentre iFR GRADIENT registry.44 Among the 134 vessels with tandem or diffuse CAD tested, the mean difference between the predicted and actual post-PCI iFR values was 0.011±0.004 with a strong correlation (r=0.73, p<0.001). Additionally, the ability of the iFR pullback to detect the individual contribution of each stenosis to the distal iFR resulted in a change in PCI strategy in 31% of vessels (compared with angiography-based decision making).44 The discrepancy between angiographically and physiologically defined targets for PCI were also highlighted in the results of the recently published DEFINE-PCI trial.45 Investigators in this study performed blinded iFR following PCI procedures that were deemed angiographically successful and found that one quarter of patients had residual ischaemia as defined by an iFR≤0.89. Given the association of adverse outcomes with post-PCI residual ischaemia,46 these findings signal the need for increase in physiologically-guided revascularisation. The upcoming DEFINE GPS study will aim to identify whether intervening on focal lesions identified by iFR pullback as responsible for residual ischaemia post-PCI reduces future adverse outcomes. Although the physiological principles relating to serial lesion assessment can potentially be extended to other NHPRs given their close correlations with iFR, there is currently no data to directly support this approach at present. The perceived advantages of using NHPRs in this setting has led to the commercialisation of ‘iFR Scout’ which provides the user with a pullback profile of the vessel to enable informed decision-making.
Left main coronary artery
Despite the well-recognised visual-functional mismatch between angiography and FFR in left main coronary artery (LMCA) lesions,47 these patients have often been excluded from the large physiological validation trials.3 16 While long-term data suggest that deferring revascularisation of LMCA lesions on the basis of FFR is safe,48 this data are not available for iFR. Furthermore, discordance between iFR and FFR has been shown to be greatest in LMCA and proximal LAD lesions.49 A recent study examining the correlation between iFR and FFR in 91 angiographically intermediate LMCA stenoses found a significant correlation (AUC=0.84; p<0.001) with classification agreement in 81% of cases.50 The iLITRO study which is estimated for completion in 2025 will aim to assess the concordance of FFR and iFR in LMCA lesions as well as to compare clinical outcomes between patients who have FFR-guided and iFR-guided treatment. Given the high incidence of downstream disease acting as serial stenoses, proponents of NHPR have suggested that LMCA lesions may best be assessed with NHPRs although outcome data for their use in this setting is required.
Acute coronary syndromes
The use of invasive physiological assessment is less established in patients presenting with ACS.51 Up to half of patients presenting with ST-elevation myocardial infarction are identified to have angiographically significant multi-vessel disease,52 53 highlighting the potential role of intracoronary physiology to enhance the evaluation and treatment of non-culprit lesions. Although there are concerns regarding a blunted hyperaemic response to adenosine following an acute myocardial infarction,54 the assessment of non-culprit ACS lesions with FFR has been shown to be reliable when assessed during the index procedure.55 56 Several randomised trials have also demonstrated that a strategy of FFR-guided revascularisation of non-culprit lesions in ACS significantly improves clinical outcomes compared with only treatment of the infarct-related artery.57 58
In non-culprit ACS lesions, conflicting studies exist on the validity of NHPR. Choi et al found iFR values were similar in non-culprit ACS lesions compared with patients with stable CAD and similar stenosis severity.59 More recently, several comprehensive physiological studies have demonstrated that resting coronary flow in non-culprit ACS lesions is significantly higher than patients with stable CAD.60 61 This may be due to localised adenosine release in response to myocardial ischaemia, which results in a partial hyperaemic response.62 This may have important implications on the accuracy of NHPR in patients with ACS, as an increase in resting flow could potentially exaggerate the pressure loss across a lesion, overestimating its functional significance. Consequently, several studies have observed a 0.01–0.02 increase in iFR from the acute event to follow-up,54 63 highlighting the need for caution in interpreting iFR in the setting of large myocardial infarctions or values around the diagnostic threshold (≤0.89).
A subanalysis of the DEFINE-FLAIR and iFR-SWEDEHEART trials demonstrated that while overall outcomes between FFR and iFR were comparable, deferral with FFR in the ACS subgroup associated with a higher rate of clinical events compared with FFR deferral in stable CAD.64 In contrast, deferral with iFR yielded similar outcomes regardless of clinical presentation.64 The limitations of subgroup analysis prevent drawing definitive conclusions on the utility of one physiological tool over the other. The ongoing prospective, multicentre iFR Guided Multi-Vessel Revascularization During Percutaneous Coronary Intervention for Acute Myocardial Infarction trial will provide further insight into the clinical value of iFR guided revascularisation in non-culprit lesions of patients with acute STEMI.
Aortic stenosis
The use of pressure-based invasive indices in patients with severe aortic stenosis (AS) is an evolving field. Between 25% and 50% of patients with severe AS have coexisting CAD and while transcatheter aortic valve replacement (TAVR) has become an increasingly common treatment modality, the management of concomitant CAD remains controversial. A recent pooled analysis demonstrated that patients undergoing TAVR with higher residual SYNTAX (Synergy Between Percutaneous Coronary Intervention With Taxus and Cardiac Surgery) score were at risk of greater subsequent mortality.65 The importance of correctly identifying ischaemia-inducing lesions in such patients prompted the recent exploration of pressure-based indices in these cohorts. While the feasibility of both FFR and iFR has been demonstrated in such patients, there are concerns that the altered ventriculo-aortic physiology distorts their accuracy.66 For example, the greater oxygen demands of hypertrophied ventricles in severe AS induces partial microcirculatory vasodilatation that increases resting coronary blood flow.67 Additionally, there is submaximal drug-induced hyperaemic response, potentially leading to underestimation of FFR significance.67–69 This latter point has led to speculation on the potential advantages of NHPR in severe AS, supported by clinicians’ reluctance to use hyperaemic agents in such patients.
The feasibility and accuracy of using iFR in patients with severe AS has been demonstrated in several studies.70–72 The data suggest that a lower iFR cut-off (0.82 or 0.83) is better predictive of ischaemia-provoking lesions compared with that validated in patients with no AS.70 72 This is likely explained by the greater resting blood flow due to the larger myocardial mass and partial microcirculatory vasodilatation which would produce greater trans-stenotic pressure gradients. This would therefore result in the lower iFR values for the same lesion if it existed in a patient with non-AS. In contrast, FFR values are likely higher and underestimate the true ischaemic burden induced by lesions given the submaximal hyperaemia.
Several studies have demonstrated discrepancies in FFR and iFR values measured in the same lesion immediately before and after TAVR,67 70 71 73 thus questioning the accuracy of the index reading. In one study of 66 patients, while mean iFR remained unchanged following TAVR there were notable variations within the individual iFR values, prompting the authors to advise caution over its use. Another recent study measuring invasive pressure and flow also demonstrated unchanged mean iFR following TAVR. Conversely, mean FFR decreased from 0.87 to 0.85. This was explained by an observed increase in systolic flow following TAVR (thus affecting whole-cycle indices), with no appreciable change in diastolic flow immediately after TAVR and thus no change in iFR.71 The remainder of the NHPRs have not been assessed in this context. There may be perceivable benefits to diastolic-only rather than whole-cycle indices in this context given the largely variable systolic physiology immediately before and after valve deployment.
The validity and role of pressure-based functional assessment of coronary stenosis in patients with severe AS continues to be investigated and two large randomised trials (NOTION-3 (NCT03058627) and FAITAVI (NCT03360591)) are currently underway to investigate the outcomes of upstream FFR-guided PCI in patients undergoing TAVR.
Myocardial bridging
Myocardial bridging (MB) has traditionally been considered a benign condition with preserved coronary perfusion in diastole. However, its associations with ACS,74 Takotsubo’s cardiomyopathy75 and malignant arrhythmias76 has highlighted attention on physiological assessment. Unlike coronary atherosclerosis, MB is a dynamic lesion that changes degree of luminal stenosis throughout the cardiac cycle due to systolic compression of the vessel as it is within the myocardium, rather than at the epicardium. This has important implications on the way pressure-based indices can be used to assess functional significance.
Studies measuring coronary pressure and flow velocity have demonstrated that there is limited or no flow through the MB segment in systole.77–79 This is followed by a spike in coronary flow in the early stages of diastole secondary to compensatory decreased microvascular resistance and concomitant residual myocardial compression. This increase in flow however, is not reflected in measured invasive pressure. The coronary pressure is highest during systole, and at times exceeds Pa. This is due to the ventricularisation of coronary pressure secondary to myocardial compression. Given this, averaged whole-cycle pressure ratios such as FFR are unsuitable for the assessment of functional significance.77–79
In a study to address this, coronary assessment was performed using diastolic FFR (hyperaemic Pd/Pa during diastole).80 This technique unmasked ischaemia in 5 of 12 patients, compared with conventional FFR, which demonstrated ischaemia in one patient. This led to speculations as to whether diastolic indices such as iFR would be more reliable in assessing the functional significance of MB. In another study, patients with angina or positive non-invasive test and MB underwent coronary assessment using FFR, iFR and hyperaemic WPR (HWPR; where iFR is measured during pharmacologically induced hyperaemia). Similar to diastolic FFR reported in the previous study, HWPR unmasked MB-related ischaemia in seven patients while FFR unmasked only one. After inotropic infusion—when most patients developed symptoms—HWPR dropped significantly while FFR did not.81 Other studies have demonstrated the importance of inotropic stimulation at unmasking ischaemia when assessing the functional significance of MBs.82
The use of NHPRs may therefore not be appropriate for assessing MB. The use of diastolic indices appears to be more appropriate than whole-cycle indices. Future studies may provide further insight on the use of hyperaemic diastolic indexes to assess MB.
Controversies in the use of NHPR
The evolution of NHPR has polarised opinions within the field with some questioning whether NHPRs can fully account for the fundamental principles of coronary and microcirculatory physiology.83 In particular, it is debated whether a truly WFP exists with no fluctuations in the microcirculatory resistance.22 84 85 These differences may be less relevant with the emergence of trials and subsequently guidelines supporting the use of iFR in clinical practice. The recent evidence demonstrating that iFR and other resting diastolic indices having a >0.99 correlation and AUC values has reignited the debate and led to the widely shared opinion that using proprietary-segmentation of the cardiac cycle offers no additive benefit.86 A recognised limitation of NHPRs is that they have been validated in cohorts of patients with intermediate coronary stenosis3 5 7 8 and there is limited data examining the physiological validity of iFR in increasingly stenotic lesions.87
A widely debated area remains the clinical relevance of discordance between the FFR and NHPR.27 37 49 88 Most data on discordance currently exist on the comparison between iFR and FFR, with discordance believed to occur ~15%–20% of lesions, particularly in those subtending large areas of myocardium, that is, LMCA and proximal LAD.49 89 Other areas where discordance has been identified include the pattern of coronary disease (focal vs diffuse),90 and patient characteristics such as gender, presence of diabetes mellitus and beta blocker use.91–94 A summary of these discordant groups associated with FFR and iFR is presented in table 2.
Evidence on discordance between FFR and iFR
The notion of discordance has created considerable discussion regarding the use of NHPRs in assessing lesions, particularly those in proximal coronary segments where they are most prognostically important. However, proponents of iFR have demonstrated that where discordance occurs, iFR better correlates with both thermodilution-derived and Doppler-derived CFR.92 95 Studies have also shown that increased risk of adverse outcomes only occurred when both iFR and FFR were both concordantly abnormal, and not in the discordant groups.92 96 Unlike FFR however,97 long-term outcome data are not available for NHPRs and will likely be key in reassuring those with ongoing concerns.
Conclusions
The emergence of NHPRs has not been without controversy and their uptake has been marred by uncertainties within the interventional community. Nonetheless, there is a plethora of evidence supporting their use, particularly with iFR, which is now guideline-recommended on the basis of randomised clinical trial data. Other NHPRs have excellent correlations with iFR, suggesting they can be used interchangeably. Certain NHPRs may be better tailored to specific patient and clinical scenarios, although further evidence is required, as is long-term clinical data to support their use. What is clear is that increasing physiologically-guided revascularisation, whether by FFR or NHPR, must remain the goal to improve patient outcomes.
References
Footnotes
Twitter @Aihdayhid
Contributors MM, conceptualisation, literature search and writing; UT, literature search and writing; JR, literature search and writing, AC, literature search and writing; ARI, literature search and writing; JDC, SN, SH AB, supervision, reviewing and editing.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests ARI has received consulting fees from Boston Scientific and Canon Medical. SH has received speaker’s bureau and proctoring fees from Abbott Vascular and Boston Scientific. AB has received consultancy fees from Abbott Vascular and Boston Scientific.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data sharing not applicable as no datasets generated and/or analysed for this study.