Article Text

Abstract
Current guidelines recommend angiotensin receptor blocker neprilysin inhibitors (ARNI) (sacubitril/valsartan) as a replacement for angiotensin-converting-enzymeinhibitor (ACE-I) in heart failure with reduced ejection fraction (HFrEF) who remain symptomatic despite optimal medical therapy. The effects of ARNIs have not previously been assessed in a systematic review. We searched for relevant trials until October 2019 in CENTRAL, MEDLINE, Embase, LILACS, BIOSIS, CNKI, VIP, WanFang and CBM. Our primary outcomes were all-cause mortality and serious adverse events. We systematically assessed the risks of random errors and systematic errors. PROSPERO registration: CRD42019129336. 48 trials randomising 19 086 participants were included. The ARNI assessed in all trials was sacubitril/valsartan. ACE-I or ARB were used as control interventions. Trials randomising HFrEF participants (27 trials) and heart failure with preserved ejection fraction (HFpEF) participants (four trials) were analysed separately. In HFrEF participants, meta-analyses and Trial Sequential Analyses showed evidence of a beneficial effect of sacubitril/valsartan when assessing all-cause mortality (risk ratio (RR), 0.86; 95% CI, 0.79 to 0.94) and serious adverse events (RR, 0.89; 95% CI, 0.86 to 0.93); and the results did not differ between the guideline recommended target population and HFrEF participants in general. We found no evidence of an effect of sacubitril/valsartan in HFpEF participants. Sacubitril/valsartan compared with either ACE-I or ARB seems to have a beneficial effect in patients with HFrEF. Our results indicate that sacubitril/valsartan might be beneficial in a wider population of patients with heart failure than the guideline recommended target population. Sacubitril/valsartan does not seem to show evidence of a difference compared with valsartan in patients with HFpEF.
- heart failure
- heart failure treatment
- renin-angiotensin system
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known about this subject?
Sacubitril/valsartan is recommended as an alternative to angiotensin-converting-enzyme inhibitor in patients with heart failure with reduced ejection fraction who remain symptomatic despite optimal medical therapy.
No former systematic review has been conducted.
What does this study add?
Meta-analysis and Trial Sequential Analyses shows that sacubitril/valsartan reduces the risk of all-cause mortality, serious adverse events, hospitalisations and NT-proBNP as well as increases quality of life and ejection fraction.
How might this impact on clinical practice?
Our results indicate that sacubitril/valsartan might be beneficial in a wider population of patients with heart failure with reduced ejection fraction.
Introduction
Worldwide, an estimated 37 million people have a diagnosis of heart failure.1 2 The lifetime risk for developing heart failure is approximately 20%.3 The prevalence of heart failure is increasing, presumably caused by an increase in both life expectancy and risk factors leading to heart failure as well as improved treatment of acute cardiovascular events.1 2 4 5
Guidelines recommend treatment of heart failure with reduced ejection fraction with a beta-blocker and an inhibitor of the renin-angiotensin-aldosterone system (angiotensin-converting-enzyme inhibitor (ACE-I) or angiotensin II receptor blocker (ARB)). It is recommended to add a mineralocorticoid-receptor antagonist in patients who remain symptomatic after this initial treatment.3 6
New drugs for heart failure have been developed and approved that combine inhibition of the renin-angiotensin-aldosterone system pathway (with an ARB) with inhibition of the neprilysin enzyme. These new types of drugs are classified as angiotensin receptor blocker neprilysin inhibitors (ARNIs).7
The European Society of Cardiology recommends ARNIs as a replacement for ACE-I in patients with heart failure with reduced ejection fraction (HFrEF) (EF <35%) who remain symptomatic (New York Heart Association (NYHA) II to IV) despite optimal medical therapy with an ACE-I, a beta-blocker and a mineralocorticoid-receptor antagonist (unless there are contraindications).6 The American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Failure Society of America, make similar recommendations.8
To our knowledge, the effects of ARNIs have not been assessed previously in a systematic review.9
Methods
This systematic review has been developed based on the Preferred Reporting Items for Systematic Reviews and Meta-Analysis Protocols (PRISMA-P) guidelines for reporting systematic reviews evaluating interventions in healthcare (online supplemental S1 text).9 10 Our methodology was predefined and described in detail in our pre-published protocol.11
Supplemental material
In short, we included all trials assessing the beneficial and harmful effects of ARNIs in participants with any type of heart failure.11 We included randomised clinical trials irrespective of trial design, setting, publication status, publication year and language. We searched from their inception to October 2019 for relevant trials in the Cochrane Central Register of Controlled Trials (CENTRAL), Medical Literature Analysis and Retrieval System Online (MEDLINE), Excerpta Medica database (Embase), Latin American and Caribbean Health Sciences Literature (LILACS), Science Citation Index Expanded on Web of Science, Chinese Biomedical Literature Database (CBM), China National Knowledge Infrastructure (CNKI), Chinese Science Journal Database (VIP), WanFang, SINOMED and BIOSIS. The search strategy can be found in (online supplemental S2 text). Additionally, we hand searched reference lists, major pharmaceutical companies and several databases for relevant publications.
Outcomes and subgroup analyses
Our primary outcomes were all-cause mortality, serious adverse events; secondary outcomes were myocardial infarction, quality of life, non-serious adverse events and hospitalisations; and exploratory outcomes were cardiovascular mortality, ejection fraction, 6-min walking distance, and NT-proBNP. We used the trial results reported at maximum follow-up.11 We planned several subgroup analyses (test of interaction)12 and sensitivity analyses11 (see ‘Results’). In addition we added three subgroup analyses: (1) trials comparing different co-interventions, (2) trials published in English compared with Chinese and (3) trials using guideline criteria for inclusion compared with trials with broader inclusion criteria.
Data collection and risk of bias
Three authors (EEN, JF and F-LB) extracted data and assessed risks of bias of the included trials using standardised extraction sheets. Disagreements were resolved by discussion with a third author (JCJ). Our bias risk assessment was based on the results of meta-epidemiological studies (online supplemental S2 ref). Hence, risks of bias were assessed using the domains random sequence generation, allocation concealment, blinding of participants and treatment providers, blinding of outcome assessment, incomplete outcome data, selective outcome reporting, for profit bias and other risks of bias.13 14 We contacted all authors by email in order to retrieve missing information.
Supplemental material
Data synthesis and assessment of significance
We used the statistical software Review Manager 5.3 provided by Cochrane to analyse data.12 We assessed our intervention effects with both random-effects meta-analyses15 and fixed-effect meta-analyses.16 We primarily used the most conservative point estimate of the two.17 We assessed two primary outcomes, and therefore, we considered a p value of 0.033 as the threshold for statistical significance.17 We investigated possible heterogeneity through subgroup analyses (test of interaction).12 In order to control the risks of type I errors and type II errors, we performed Trial Sequential Analysis.17
Results
Study characteristics
We identified 2393 potentially relevant studies through our literature search conducted in October 2019. In addition, three potential studies were identified through Novartis clinical registry. We included a total of 48 trials randomising 19 086 participants (figure 1). In all trials, the experimental intervention was 97 mg sacubitril/ 103 mg valsartan two times per day. The trials were conducted between 2012 and 2019 in 48 different countries. Nine of the included trials were written in English and published in Western databases and these trials accounted for 83% of the included participants. Two of these trials randomised 71% of all participants.18 19 Thirty-nine trials were conducted and published in China. These trials were generally small (34 to 180 participants) and reported mostly on surrogate outcomes (left ventricular ejection fraction, 6-min walking distance and NT-proBNP). Characteristics of included studies are summarised in (table 1).

PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analysis) flow diagram.
Characteristics of included studies
All nine trials published in English-language journals were judged to be high risk of bias mainly due to industry funding; Novartis Pharmaceuticals funded all nine trials. All trials published in Chinese were judged to be of high risk of bias and of low methodological quality; for example, none of the trials registered/ published protocols, used blinding and only 18/39 reported how the randomisation process was conducted (figure 2).

Risk of bias summary.
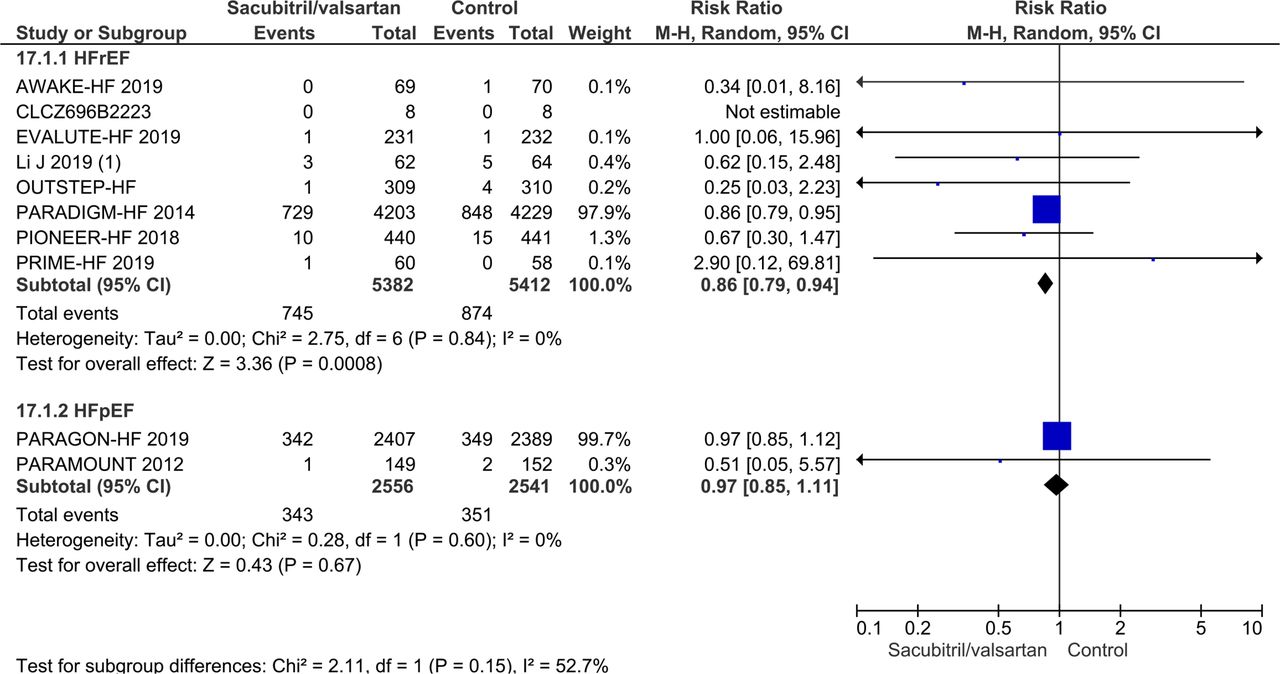
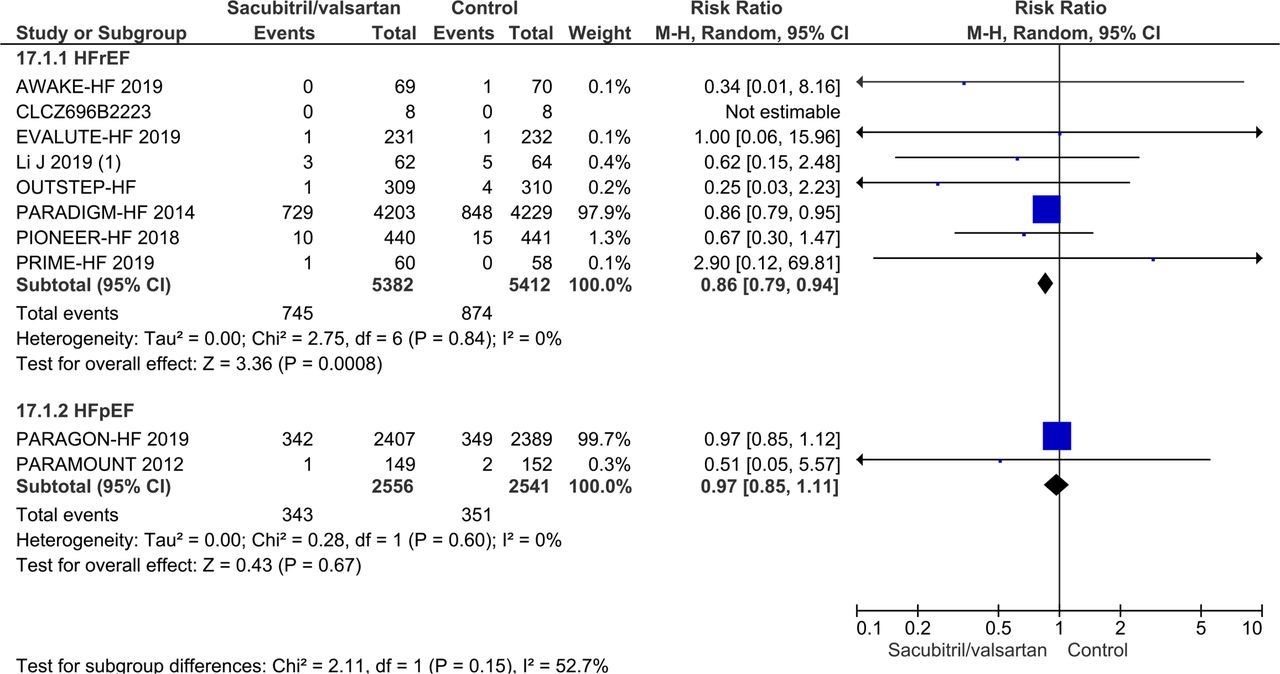
Forest plot of subgroup based on type of heart failure on all-cause mortality.
Twenty-seven trials randomised a total of 12 311 HFrEF participants and four trials randomised 5278 heart failure with preserved ejection fraction (HFpEF) participants. The remaining 17 trials randomising a total of 1497 participants either did not specify which type of heart failure they assessed, or they included participants with different types of heart failure. The majority (93.0%) of the total number of randomised participants had NYHA II or III. The mean age of the trial participants was 65.9 years and the mean proportion of women was 34.2%. Baseline characteristics are summarised in (table 2).
Baseline characteristics
The trials used different control interventions: 14 trials used valsartan, 20 trials used an ACE-I (enalapril=12, benazepril=7, perindopril=1 and ramipril=1); 8 trials did not administer any comparator to the control group besides usual care, which was planned to be administered in both groups (as co-intervention); and 4 trials used either an unspecified ARB or an unspecified ACE-I. One trial used intravenous milrinone as control intervention. All trials used guideline recommended co-interventions (usual care) planned to be delivered similarly in both intervention groups, that is, beta-blockers, mineralocorticoid-receptor antagonists, diuretics and digitalis, if indicated.
Visual inspection of the forest plots and statistical tests (I2 statistics) showed signs of heterogeneity (figure 3 and online supplemental S1 figure). When trials randomising HFrEF participants and trials randomising HFpEF participants were analysed separately, then the heterogeneity was mostly resolved. Hence, we chose to report results separately for each type of heart failure.11
Supplemental material
Participants with heart failure with reduced ejection fraction
Primary outcomes
All-cause mortality
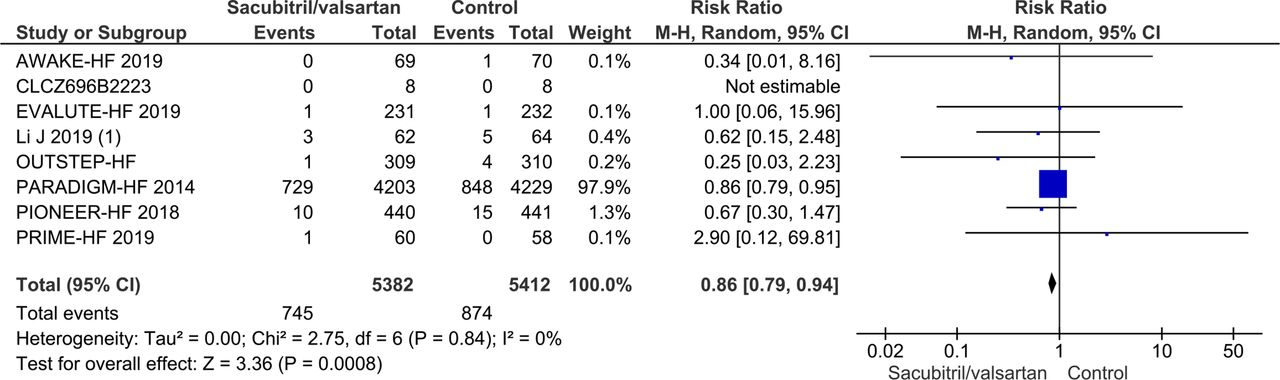
Seven trials randomising a total of 10 794 HFrEF participants reported on all-cause mortality. A total of 745/5382 (13.8%) sacubitril/valsartan participants died compared with 874/5412 (16.1%) control participants (mean follow-up of 22.8 months). Meta-analysis (risk ratio (RR), 0.86; 95% CI, 0.79 to 0.94; p=0.0008) showed evidence of a beneficial effect of sacubitril/valsartan compared with control (figure 4). Neither visual inspection of the forest plot nor tests for statistical heterogeneity (I2=0%; p=0.84) indicated significant heterogeneity. Trial Sequential Analysis showed that there was enough information to confirm that sacubitril/valsartan compared with control reduced the risk of death by 15% (figure 5). Incomplete outcome data alone did not seem to have the potential to influence the meta-analysis results (online supplemental S2 and S3 figures). The following tests of interaction showed no evidence of a difference: (1) acute decompensated heart failure participants compared with chronic heart failure participants (p=0.53); (2) different types of control intervention (valsartan, enalapril and benazepril) (p=0.68); (3) trials published in English compared with trials published in Chinese (p=0.64); and (4) trials using guideline criteria for inclusion compared with trials with broader inclusion criteria (p=0.77) (online supplemental S4–S7 figures). None of the remaining planned subgroup analyses could be conducted due to lack of relevant data.11
Supplemental material
Supplemental material
Supplemental material
Supplemental material
Supplemental material
Supplemental material

Forest plot of participants with heart failure with reduced ejection fraction on all-cause mortality.

Trial sequential analysis of participants with heart failure with reduced ejection fraction on all-cause mortality.
Serious adverse events
Seven trials randomising a total of 10 794 HFrEF participants reported on serious adverse events. A total of 2013/5382 (37.4%) sacubitril/valsartan participants had a serious adverse event compared with 2263/5412 (41.8%) control participants (mean follow-up of 22.8 months). Meta-analysis (RR, 0.89; 95% CI, 0.86 to 0.94; p=<0.00001) showed evidence of a beneficial effect of sacubitril/valsartan compared with control (figure 6). Neither visual inspection of the forest plot nor test for statistical heterogeneity (I2=33%; p=0.17) indicated significant heterogeneity. Trial Sequential Analysis showed that there was enough information to confirm that sacubitril/valsartan compared with control reduced the risk of serious adverse events by 15% (figure 7). Incomplete outcome data alone did not seem to have the potential to influence the meta-analysis results (online supplemental S8 and S9 figures). The following tests of interaction showed no evidence of a difference: (1) different types of control intervention (valsartan, enalapril and and benazepril) (p=0.81); (2) trials published in English compared with trials published in Chinese (p=0.77); (3) trials using guideline criteria for inclusion compared with trials with broader inclusion criteria (p=0.62) (online supplemental S10–S12 figures). Test of interaction showed evidence of a difference when comparing acute decompensated heart failure participants to chronic heart failure participants (p=0.004) (online supplemental S13 figure). One trial randomised 881 participants with acute decompensated heart failure. However, this trial did not publish a full list of serious adverse events but only reported a predefined composite of serious clinical events. The remaining six trials randomised participants with chronic heart failure. None of the remaining planned subgroup analyses could be conducted due to lack of relevant data.11
Supplemental material
Supplemental material
Supplemental material
Supplemental material
Supplemental material
Supplemental material
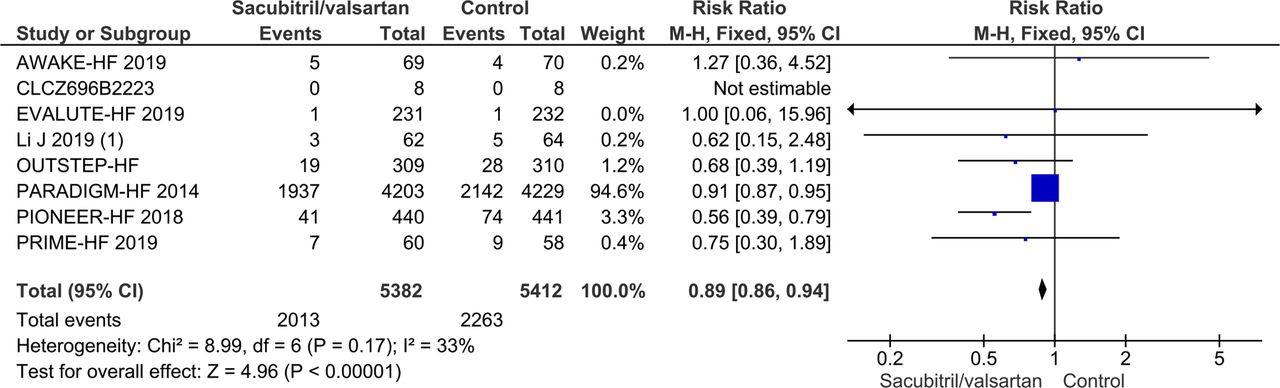
Forest plot of participants with heart failure with reduced ejection fraction on serious adverse events.

Trial sequential analysis of participants with heart failure with reduced ejection fraction on serious adverse events.
All serious adverse events were analysed individually and can be found in supplemental appendix (online supplemental S1 table). As a hypothesis generating analyses, we performed meta-analyses on all serious adverse events. Meta-analysis showed evidence of a beneficial effect of sacubitril/valsartan compared with control, when assessing the risk of hyperkalaemia (RR 0.44; 95% CI, 0.26 to 0.76; p=0.003), fatigue (RR 0.10; 95% CI, 0.10 to 0.79; p=0.03) and syncope (RR 0.62; 95% CI, 0.43 to 0.91; P 0.01). Prior neprilysin in combination with ACE-I have shown an elevated risk of angioedema. Meta-analysis showed no evidence of a difference between sacubitril/valsartan compared with control on angioedema (RR 1.01; 95% CI, 0.27 to 3.72; p=0.99).
Secondary outcomes
Myocardial infarction
Two trials randomising a total of 9051 HFrEF participants reported on myocardial infarction. A total of 70/4513 (1.6%) sacubitril/valsartan participants had a myocardial infarction compared with 72/4538 (1.6%) control participants. Meta-analysis (RR, 0.98; 95% CI, 0.71 to 1.35; p=0.89) showed no evidence of a difference between sacubitril/valsartan and control (online supplemental S14 figure). Neither visual inspection of the forest plot nor tests for statistical heterogeneity (I2=0%; p=0.62) indicated significant heterogeneity. Trial Sequential Analysis showed that there was not enough information to confirm or reject that sacubitril/valsartan compared with control reduced the risk of myocardial infarction by 15% (online supplemental S15 figure). Incomplete outcome data alone did not seem to have the potential to influence the meta-analysis results (online supplemental S16 and S17 figures). None of the planned subgroup analyses could be conducted due to lack of relevant data.11
Supplemental material
Supplemental material
Supplemental material
Supplemental material
Quality of life
Two Chinese trials randomising 232 HFrEF participants reported on quality of life using the Minnesota Living with Heart Failure Questionnaire (MLHFQ). Meta-analysis (mean difference (MD), −5.19; 95% CI, −8.37 to −2.01; p=0.001) showed evidence of a beneficial effect of sacubitril/valsartan compared with control (online supplemental S18 figure). Both visual inspection of the forest plot and tests for statistical heterogeneity (I2=85%; p=0.01) indicated substantial signs of heterogeneity which could not be resolved. Trial Sequential Analysis showed that there was enough information to confirm a MD of 5 (online supplemental S19 figure). Incomplete outcome data alone did not seem to have the potential to influence the results. Only one trial randomising 8442 participants reported on quality of life using the Kansas City Cardiomyopathy Questionnaire (KCCQ).20 The trial had a follow-up of 36 months and found a least squared mean of 2.28 (0.73), with a p value of 0.002. None of the planned subgroup analyses could be conducted due to lack of relevant data.
Supplemental material
Supplemental material
Non-serious adverse events
Nine trials randomising a total of 10 401 HFrEF participants reported on non-serious adverse events. A total of 2738/5186 (52.8%) sacubitril/valsartan participants had a non-serious adverse event compared with 2855/5215 (54.7%) control participants. Meta-analysis (RR, 0.91; 95% CI, 0.74 to 1.11; p=0.35) showed no evidence of a difference between sacubitril/valsartan and control (online supplemental S20 figure). Both visual inspection of the forest plot and tests for statistical heterogeneity (I2=60%; p=0.009) indicated moderate signs of heterogeneity which could not be resolved. Trial Sequential Analysis showed that there was not enough information to confirm or reject that sacubitril/valsartan compared with control reduced the risk of non-serious adverse events by 15% (online supplemental S21 figure). Incomplete outcome data alone did not have the potential to influence the meta-analysis results (online supplemental S22 and S23 figures). Test of interaction showed evidence of a difference when comparing trials only including patients according to current guidelines compared with trials including all HFrEF participants (online supplemental S24 figure). Three subgroup analyses showed no evidence of a difference (online supplemental figures 25–27). None of the remaining planned subgroup analyses could be conducted due to lack of relevant data.11
Supplemental material
Supplemental material
Supplemental material
Supplemental material
Supplemental material
Supplemental material
Supplemental material
Supplemental material
Hospitalisations
Four trials randomising a total of 9476 HFrEF participants reported on hospitalisations during follow-up. A total of 594/4724 (12.6%) sacubitril/valsartan participants were hospitalised during follow-up compared with 756/4752 (15.9%) control participants. Meta-analysis (RR, 0.79; 95% CI, 0.72 to 0.87; p=<0.00001) showed evidence of a beneficial effect of sacubitril/valsartan compared with control (online supplemental S28 figure). Neither visual inspection of the forest plot nor tests for statistical heterogeneity (I2=31%; p=0.09) indicated significant heterogeneity. Trial Sequential Analysis showed that there was enough information to confirm that sacubitril/valsartan compared with control reduced the risk of hospitalisations by 15% (online supplemental S29 figure). Incomplete outcome data alone did not seem to have the potential to influence the meta-analysis results (online supplemental S30 and S31 figures). Three subgroup analyses showed no evidence of a difference (online supplemental S32–S34 figures). None of the remaining planned subgroup analyses could be conducted due to lack of relevant data.11
Supplemental material
Supplemental material
Supplemental material
Supplemental material
Supplemental material
Supplemental material
Supplemental material
Exploratory outcomes
Cardiovascular mortality, ejection fraction, 6-min walking distance and NT-proBNP were analysed as exploratory outcomes. Meta-analyses showed evidence of a beneficial effect of sacubitril/valsartan compared with control when assessing ejection fraction (online supplemental S35 figure), 6-min walking distance (online supplemental S36 figure) and NT-proBNP (online supplemental S37 figure). Only one trial assessed cardiovascular mortality so meta-analysis could not be performed.21
Supplemental material
Supplemental material
Supplemental material
Participants with heart failure with preserved ejection fraction
Primary outcome
All-cause mortality
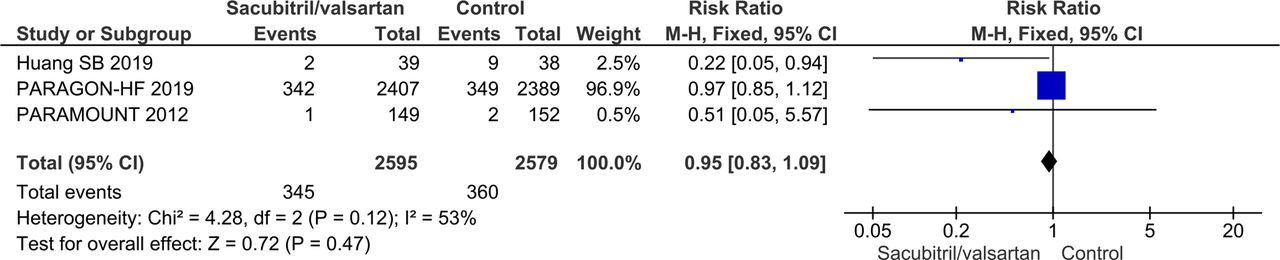
Three trials randomising a total of 5174 HFpEF participants reported on all-cause mortality. A total of 345/2595 (13.3%) sacubitril/valsartan participants died compared with 360/2579 (14.0%) control participants (mean follow-up of 34.1 months). Meta-analysis (RR, 0.95; 95% CI, 0.83 to 1.09; p=0.47) showed no evidence of a beneficial effect of adding sacubitril/valsartan compared with control (figure 8). Both visual inspection of the forest plot and test for statistical heterogeneity (I2=53%; p=0.12) indicated moderate heterogeneity. When removing the trial published in China assessing sacubitril/valsartan compared with usual care, with an extreme result, no heterogeneity was observed. Trial Sequential Analysis showed that there was not enough information to confirm or reject that sacubitril/valsartan compared with control reduced the risk of death by 15% (online supplemental S38 figure). A post-hoc Trial Sequential Analysis showed that there was enough information to confirm that sacubitril/valsartan compared with control did not reduce the risk of death by 20% (figure 9). Incomplete outcome data alone did not seem to have the potential to influence the meta-analysis results (online supplemental S39 and S40 figures). Test of interaction showed evidence of a difference between (1) trials published in English compared with Chinese (p=0.05) and (2) different control interventions (valsartan and usual care) (p=0.05) (online supplemental S41 and S42 figures). None of the remaining planned subgroup analyses could be conducted due to lack of relevant data.11
Supplemental material
Supplemental material
Supplemental material
Supplemental material
Supplemental material

Forest plot of participants with heart failure with preserved ejection fraction on all-cause mortality.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Trial sequential analysis of participants with heart failure with preserved ejection fraction on all-cause mortality.
Serious adverse events
Three trials randomising a total of 5174 HFpEF participants reported on serious adverse events. A total of 1448/2607 (55.5%) sacubitril/valsartan participants had a serious adverse event compared with 1455/2592 (56.1%) control participants (mean follow-up of 34.1 months). Meta-analysis (RR, 0.99; 95% CI, 0.94 to 1.04; p=0.63) showed no evidence of a difference between sacubitril/valsartan and control (online supplemental S43 figure). Both visual inspection of the forest plot and test for statistical heterogeneity (I2=64%; p=0.06) indicated moderate heterogeneity. When removing the trial published in China assessing sacubitril/valsartan compared with usual care, with an extreme result, no heterogeneity was observed. Trial Sequential Analysis showed that there was enough information to reject that sacubitril/valsartan compared with control reduced the risk of serious adverse events by 15% (online supplemental S44 figure). Incomplete outcome data alone did not seem to have the potential to influence the meta-analysis results (online supplemental S45 and S46 figures). Test of interaction showed evidence of a difference between (1) trials published in English compared with Chinese (p=0.04) and (2) different control interventions (valsartan and usual care) (p=0.04) (online supplemental S47 and S48 figures). None of the remaining planned subgroup analyses could be conducted due to lack of relevant data.11
Supplemental material
Supplemental material
Supplemental material
Supplemental material
Supplemental material
Supplemental material
Secondary outcomes
Two trials randomising a total of 5122 HFpEF participants reported on myocardial infarction. Meta-analysis (RR, 0.94; 95% CI, 0.59 to 1.50; p=0.79, I2=0%) showed no evidence of a difference between sacubitril/valsartan and control (online supplemental S49 figure). The same trials reported on non-serious adverse events. Meta-analysis (RR, 0.96; 95% CI, 0.85 to 1.09; p=0.56, I2=50%) showed no evidence of a difference between sacubitril/valsartan and control (online supplemental S50 figure). Only one trial assessed quality of life using the KCCQ – OSS score and found no evidence of a difference.22
Supplemental material
Supplemental material
Exploratory outcomes
Cardiovascular mortality, ejection fraction, 6-min walking distance and NT-proBNP were analysed as exploratory outcomes. Meta-analysis showed no evidence of a difference when assessing ejection fraction (online supplemental S51 figure). Six-minute walking distance23 and NT-proBNP22 were only assessed in one trial each so meta-analysis could not be performed. No trials reported cardiovascular mortality.
Supplemental material
Summary of findings
Our main results are presented in the summary of findings tables (tables 3 and 4).
Summary of findings table – heart failure with reduced ejection fraction
Summary of findings table – heart failure with preserved ejection fraction
Discussion
We included a total of 48 trials. HFrEF participants and HFpEF participants were analysed separately due to heterogeneity showing difference in effect between these two types of participants. Twenty-seven trials randomised a total of 12 391 HFrEF participants and four trials randomised a total of 5278 HFpEF participants. The remaining 17 trials randomised a total of 1497 participants, did either not report the participants’ type of heart failure or included a combination of both HFpEF and HFrEF participants. Nevertheless, these 17 trials did not report any data on our primary outcomes, and very limited data for our secondary outcomes. All trials and outcome results were at high risk of bias. The certainty of the evidence according to GRADE was judged to be moderate to very low (tables 3 and 4).
Meta-analyses and Trial Sequential Analyses showed that sacubitril/valsartan compared with control decreases the risk of death, risk of serious adverse events, risk of hospitalisations and NT-proBNP; and seems to increase quality of life using the MLHFQ, ejection fraction and 6-min walking distance; and have no effect on myocardial infarction and non-serious adverse events. Current guidelines recommend sacubitril/valsartan as a replacement for ACE-I in HFrEF patients (EF <35%) who remain symptomatic (NYHA II to IV) despite optimal medical therapy with ACE-I, beta-blocker and mineralocorticoid-receptor antagonist.6 8 Our meta-analyses showed no signs of heterogeneity when including trials regardless of prior treatment with ACE-I, NYHA class and NT-proBNP, that is, our results indicate that sacubitril/valsartan seems to be beneficial in HFrEF patients in general. In addition, we performed a post-hoc subgroup analyses on our primary outcomes, we assessed the difference between trials using guideline recommended inclusion criteria with trials randomising patients with HFrEF irrespective of prior treatment with ACE-I, NYHA class and NT-proBNP. We found no significant subgroup difference (see Primary outcomes). Our results suggest that sacubitril/valsartan might be beneficial for patients with HFrEF in general and not only in the guideline recommended target population. Furthermore, current guidelines highlight that sacubitril/valsartan is associated with an increased risk of hypotension and angioedema. Our results showed no evidence of a difference between sacubitril/valsartan and control when assessing risk of hypotension and angioedema.
In HFpEF participants, meta-analysis and Trial Sequential Analysis showed no evidence of a difference between sacubitril/valsartan and control when assessing all-cause mortality, serious adverse events, myocardial infarction, non-serious adverse events, quality of life and ejection fraction. Not enough data was available for the remaining outcomes.
Our review has several strengths. We followed our protocol, which was registered and published prior to the systematic literature search.11 Data were extracted by two authors in order to minimise the risk of inaccurate data extraction. This systematic review considered both risks of random errors and risks of systematic errors. Bias was assessed according to Cochrane13 and Lundh.14 We used GRADE to assess the certainty of the evidence,24 25 Trial Sequential Analysis to assess the risks of random errors, (online supplemental S3 ref) the eight-step assessment suggested by Jakobsen et al to assess if the thresholds for significance were crossed,17 subgroup analyses to assess possibly heterogeneity and sensitivity analyses to test the potential impact of incomplete outcome data bias.17 We included data from both unpublished and published trials.
Our review also has several limitations. The majority of our participants came from two trials,18 19 which held the largest weight in our meta-analysis. However, the heterogeneity of the trials in our meta-analysis was judged very low, both by test of heterogeneity (p=0.84), and by visual inspection. In addition, the point estimates of the smaller trials is mostly centred around the RR of the meta-analysis results, indicating that the results of the larger trials are reproducible. All included trials had high risk of bias, which might bias our review results.14 All nine English published trials were sponsored by Novartis, which currently produces the only licensed sacubitril/valsartan. This might introduce high risk of bias as study-sponsored studies tend to show more favourable efficacy results and conclusions than trials receiving sponsorship by other sources.14 These limitations should be considered when interpreting the results. There were differences in the choice of control intervention for trials including HFrEF participants. The majority of trials with HFrEF participants used enalapril as control intervention with a target dose of 10 mg twice daily, below the guideline recommended dose of 20 mg. However, the dose is higher than in the trials that lay the basis for recommending enalapril in the first place. In our meta-analysis of trials with HFpEF participants, all trials used valsartan as control except one small trial. However, valsartan is not recommended in guidelines for HFpEF patients, due to their failure to show benefit in large randomised trials.26 27 The choice of control interventions has been an issue of debate and our present results should be interpreted accordingly.28 29 Subgroup analyses assessing the potential difference between control interventions, showed no significant subgroup difference.
We identified 12 ongoing trials. Characteristics of the ongoing trials are summarised in (online supplemental S2 table).
Conclusions
Sacubitril/valsartan compared with either ACE-I or ARB seems to have a beneficial effect in patients with heart failure with reduced ejection fraction. Our results indicate that sacubitril/valsartan might be beneficial in a wider population of patients with heart failure than the guideline recommended target population. Sacubitril/valsartan does not seem to show evidence of a difference compared with valsartan in patients with heart failure with preserved ejection fraction.
Acknowledgments
Department of Internal Medicine – Cardiology Section, Holbæk Hospital, Denmark, and the Institute of Regional Health Research, University of Southern Denmark, Odense, Denmark, paid the salary for all authors during the writing of the review.
References
Footnotes
Contributors EEN conceived the systematic review, conducted the literature search, data extraction, data analysis, data interpretation and wrote the article. JF conducted the literature search, data extraction, aided in data interpretation and amended the article. F-LB conducted the literature search, data extraction and amended the article. MHO, IR, and FS-H helped conceive the systematic review, provided invaluable comments and amended the article. JCJ conceived the systematic review, aided in data interpretation and amended the article.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Disclaimer No ethics approval was obtained, as all data is anonymised and all data used is obtained from clinical trials in which informed consent has already been obtained by trial investigators.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information.