Article Text

Abstract
Objective A multidisciplinary heart valve team is recommended for the evaluation of treatment in patients with valvular heart disease, but evidence supporting this concept is lacking. In patients with severe mitral regurgitation, we thought to analyse the patient selection process by the heart team for different treatment options and the outcome after treatment.
Methods In this single-centre cohort study, all patients treated for mitral regurgitation between July 2013 and September 2018 were included. Primary end points during follow-up were all-cause mortality and a combined end point, consisting of all-cause mortality, cardiovascular rehospitalisation and mitral valve reintervention.
Results 179 patients (44.8%) were treated using Mitraclip, 185 (46.2%) by surgical repair and 36 (9.0%) by surgical replacement. The mortality risk according to EuroScore II differed significantly between treatment groups (6.6%±5.6%, 1.7%±1.5% and 3.6%±2.7% for Mitraclip, surgical repair and replacement, respectively, p<0.001). In-hospital mortality for the 3 groups were 3.4%, 1.6% and 8.3%, respectively (p=0.091). Overall, surgical repair patients had higher 4-year survival (HR 0.40 (95% CI 0.26 to 0.63), p<0.001) and fewer combined end points (HR 0.51 (95% CI 0.32 to 0.80), p<0.001) compared with surgical replacement and Mitraclip patients. However, patients undergoing Mitraclip for isolated, primary mitral regurgitation achieved very good long-term survival.
Conclusion The multidisciplinary heart team assigned only low-risk patients with favourable anatomy to surgical repair, while high-risk patients underwent Mitraclip or surgical replacement. This strategy was associated with lower than expected in-hospital mortality for Mitraclip patients and high 4-year survival rates for patients undergoing surgical or percutaneous repair of isolated primary mitral regurgitation.
- surgery-valve
- percutaneous valve therapy
- mitral regurgitation
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known about this subject?
According to current guidelines, a multidisciplinary heart valve team is recommended for the evaluation of treatment in patients with severe valvular heart disease; however, there is a lack of data supporting this approach, and the decision-making process is not well defined.
What does this study add?
In this single-centre cohort study including 400 patients, we thought to analyse the patient selection process by the heart team for different treatment options in patients with mitral valve regurgitation and the outcome after treatment.
The multidisciplinary heart team assigned only low-risk patients with favourable anatomy to surgical repair, while high-risk patients underwent Mitraclip or surgical replacement.
This strategy was associated with lower than expected in-hospital mortality for Mitraclip patients and high 4-year survival rates for patients undergoing surgical or percutaneous repair of isolated primary mitral regurgitation.
How might this impact on clinical practice?
A consequent selection process by the heart team requires reduction of factors often biassing treatment assignment.
In view of future treatment options including percutaneous mitral valve replacement, the heart team selection process becomes even more important and may influence patient outcome.
Introduction
Patients undergoing surgical treatment for mitral regurgitation (MR) have been studied for decades. In selected patient populations (relatively young patients, primary MR), surgical mitral valve repair (MVrepair) leads to outstanding repair rates and excellent long-term survival.1 2 However, in patients with secondary MR, and in particular in ischaemic heart disease, it is an ongoing debate whether surgical MVrepair or mitral valve replacement (MVR) is the treatment of choice.3 In addition, for elderly patients outcomes after mitral valve (MV) surgery are far less favourable.4 Percutaneous MV repair using the Mitraclip (MC) procedure has proven to be a treatment alternative for surgical high-risk patients with MR.5 6 However, these specific cohorts or randomised trials exclude many patients seen in daily practice, and single surgeon experiences in few, highly specialised centres may not represent reality in large parts of the world where patients are evaluated and treated by heart teams.
The concept of an multidisciplinary heart team (MDT) has evolved to a central role in modern cardiovascular care to ensure the most appropriate individual treatment and to improve the outcome for each patient.7 However, evidence supporting such an approach is lacking, in particular for MV regurgitation.8 Furthermore, the exact patient selection process performed by the MDT has not been described. The aim of this study was to report the selection process and the outcomes of patients undergoing MV treatment in a centre with an institutionalised MDT approach.
Methods
Patient population
In this retrospective cohort analysis, all patients treated for MR at the Heart Clinic Zurich between July 2013 and September 2018 were included. Three patients treated with percutaneous valve-in-valve/ring replacement were excluded as they have been reported elsewhere.9 Surgical treatment included isolated or combined MV surgery (MV surgery plus coronary bypass and/or additional valve surgery). In the percutaneous group, interventions counted as combined instead of isolated if the MC procedure was part of a beforehand planned series of interventions, including percutaneous coronary and/or other valve interventions. Clinical data, including follow-up data, were extracted from patient charts and by telephone interview. Twelve patients were lost to follow-up. Echocardiographic parameters were quantified according to current guidelines.10 11
MDT decision
The MDT of the Heart Clinic Zurich consists of cardiac surgeons (two dedicated MV surgeons with >600 MVrepair operations each), interventional cardiologists (three experienced in MC procedure, main operator with >500 MC interventions), imaging and heart failure specialists as well as cardiac anaesthetists. The MDT meets weekly to discuss all heart valve cases and works as an organisationally and financially independent unit. In cases of disagreement between the team members regarding optimal treatment, decision is taken according to the majority principle of present team members.
According to current guidelines, the MDT assigned all patients to one of the three treatment strategies (MC, surgical MVrepair or primary MV replacement (I° MVR)).8 12 The primary MDT’s treatment intention was surgical MVrepair. Anatomical amenability for MVrepair was analysed using three-dimensional transoesophageal echocardiography.13 For patients deemed high risk for surgery but with suitable MV anatomy, percutaneous MV repair using MC was performed.14 Patients were considered ‘high surgical risk’ based on a combination of factors, including estimated mortality (EuroScore II) >4%, age >80 years and additional clinical risk factors not covered by EuroScore II such as frailty, obesity or liver disease. If neither MVrepair nor MC seemed feasible according to anatomical criteria, or the surgical repair effort appeared unreasonably high, primary MV replacement was performed.
In-hospital outcome
In-hospital outcome was measured as success of the initial treatment strategy and in terms of mortality. ‘Treatment success’ in surgical patients was defined as survival with residual MR ≤mild, no secondary MVR and absence of MV stenosis at discharge. The term ‘secondary’ MVR was used for patients in whom primary MVrepair failed and the surgical team decided intraoperatively to convert to MVR. Absence of mitral stenosis was defined as mean transvalvular gradient <5 mm Hg, or a gradient ≥5 mm Hg when haemodynamically explained by heart rate and/or haemoglobin level. In MC patients, a residual MR ≤moderate at discharge with a reduction in MR by ≥1 grade from baseline was still considered as success. Pure technical success for MC patients was defined according to the M-VARC criteria.5 15
Follow-up outcome
Primary end points during follow-up were all-cause mortality and a combined endpoint, consisting of all-cause mortality, cardiovascular rehospitalisation and MV reintervention.
Secondary end points during follow-up were severity of MR and dyspnoea according to the New York Heart Association classification (NYHA) after 3 months, 1 year and at the last follow-up examination before January 2019. Secondary end points were analysed separately for the accomplished intervention at discharge (MC, MVrepair or all MVR).
Statistical analysis
Continuous data are expressed as mean±SD, and categorical data as number and percentage (%). To compare data, we used the t-test, one-way analysis of variance (ANOVA) or repeated measures ANOVA, as appropriate. The Kaplan-Meier survival curves were constructed to estimate event-free survival for different subgroups and were compared with the log rank (Mantel-Cox) test. Univariate and multivariate Cox-regression model was used to analyse the predictors on combined end points. The conditional average treatment effect was estimated for various subgroups of patients as the difference in probability of a combined end point within 1 year between MVrepair and MC using an augmented inverse probability weighted estimate. Both the treatment and outcome model were fitted with a Random Forest regression and a missForest imputation was used for 5.9% missing covariate values, while the width of the CIs was approximated using Bootstrap. The level of significance was set at a p value of <0.05. All statistical analyses were performed using SPSS software (V.25.0, SPSS, Chicago, Illinois, USA) and R (V.3.4.1).
Results
MDT decision and baseline characteristics
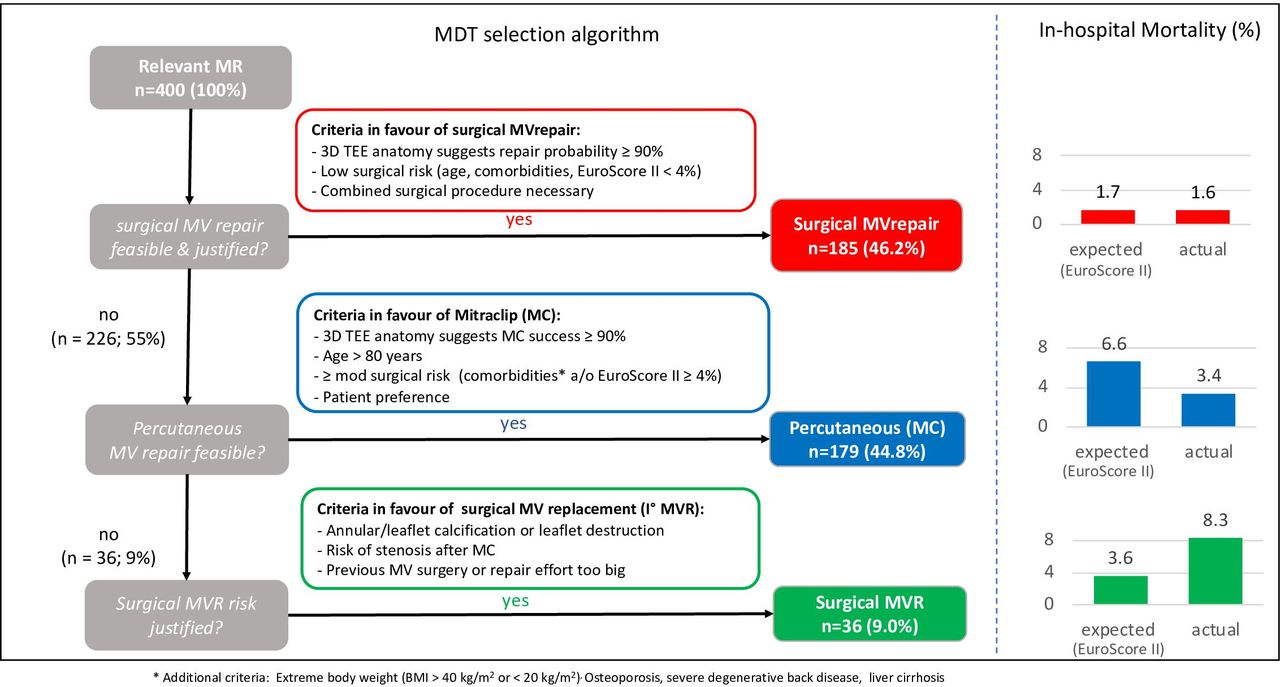
Figure 1 demonstrates the assignment to the initial treatment strategy. Seventy-five per cent of MVrepair and 55% of MVR patients had isolated MV surgery. Baseline characteristics are summarised in table 1. Within the MC population, 57.0% of patients were treated for primary (EuroScore II 5.2%) and 35.7% for secondary MR (EuroScore II 9.0%). Of patients assigned to MVrepair, only 4.9% were treated for secondary MR (EuroScore II 3.1%).

Decision-making algorithm of the heart team compared with estimated and experienced in-hospital mortality. MDT, multidisciplinary heart team; MR, mitral regurgitation; MV, mitral valve; MVR, surgical MV replacement.
Baseline characteristics of the study population (n=400)
In-hospital outcome
Treatment success rates at discharge for the initial treatment strategy MC, MVrepair and MVR were 84.9%, 89.7% and 91.7%, respectively (p=0.284). The treatment success rate for patients who underwent minimally invasive MVrepair for isolated MR was 93.6%. For MC patients, the technical success rate according to the M-VARC criteria was 99.4%.
One MC patient (0.6%) and 12 MVrepair patients (6.5%) needed peri-interventional conversion to MV replacement (secondary MVR) and were counted as failure of initial treatment strategy. Anatomical and peri-interventional factors associated with treatment success (or failure) for the three treatment arms are summarised in table 2. Of note, staged percutaneous interventions did not impact initial MC treatment success, while concomitant surgical procedures, in particular aortic valve replacement, were more frequent in patients in whom the surgical treatment strategy failed. A calcified leaflet and/or annulus was more frequent in patients in whom surgical MVrepair failed but had no impact on MC or MVR treatment success.
Anatomical and peri-interventional factors associated with in-hospital outcome
The median (IQR) duration of hospital stay was 5 (4–7.5) days for MC, 10 (9–12) days for MVrepair and 12 (10–19.3) days for MVR. Echocardiographic findings at discharge are summarised in table 3.
Echocardiographic findings at discharge
In-hospital mortality of MC, MVrepair and MVR was 3.4%, 1.6% and 8.3%, respectively, p=0.091 (figure 1).
Long-term outcome according to initial treatment strategy
Outcomes of the entire cohort during the mean follow-up time of 32.2±17.6 months are reported in figure 2A,B. Single and multivariate regression analysis of factors predicting combined end points in MC and MVrepair patients are summarised in table 4.
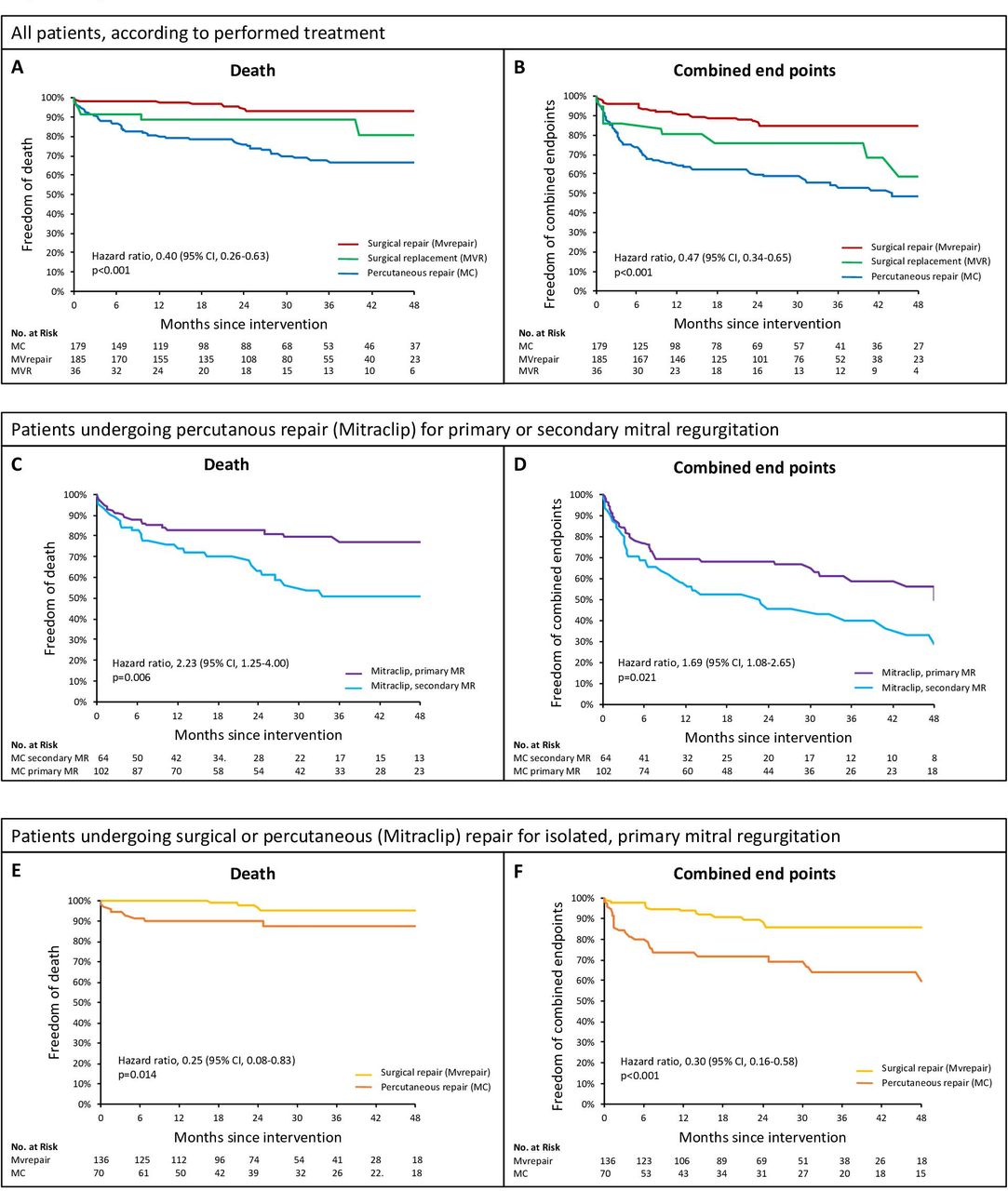
Long-term all-cause mortality and combined end points of the overall cohort (A and B), of Mitraclip patients according to the mitral regurgitation (MR) aetiology (C and D), and of patients with a primary MR who received an isolated repair, either by Mitraclip or surgically (E and F).
Predictors for combined end points
When analysing the long-term impact of treatment success at discharge, failure of initial treatment strategy did not influence all-cause mortality for MC or MVrepair patients but led to more combined end points in MC patients (HR 0.528, 95% CI 0.289 to 0.964, p=0.034).
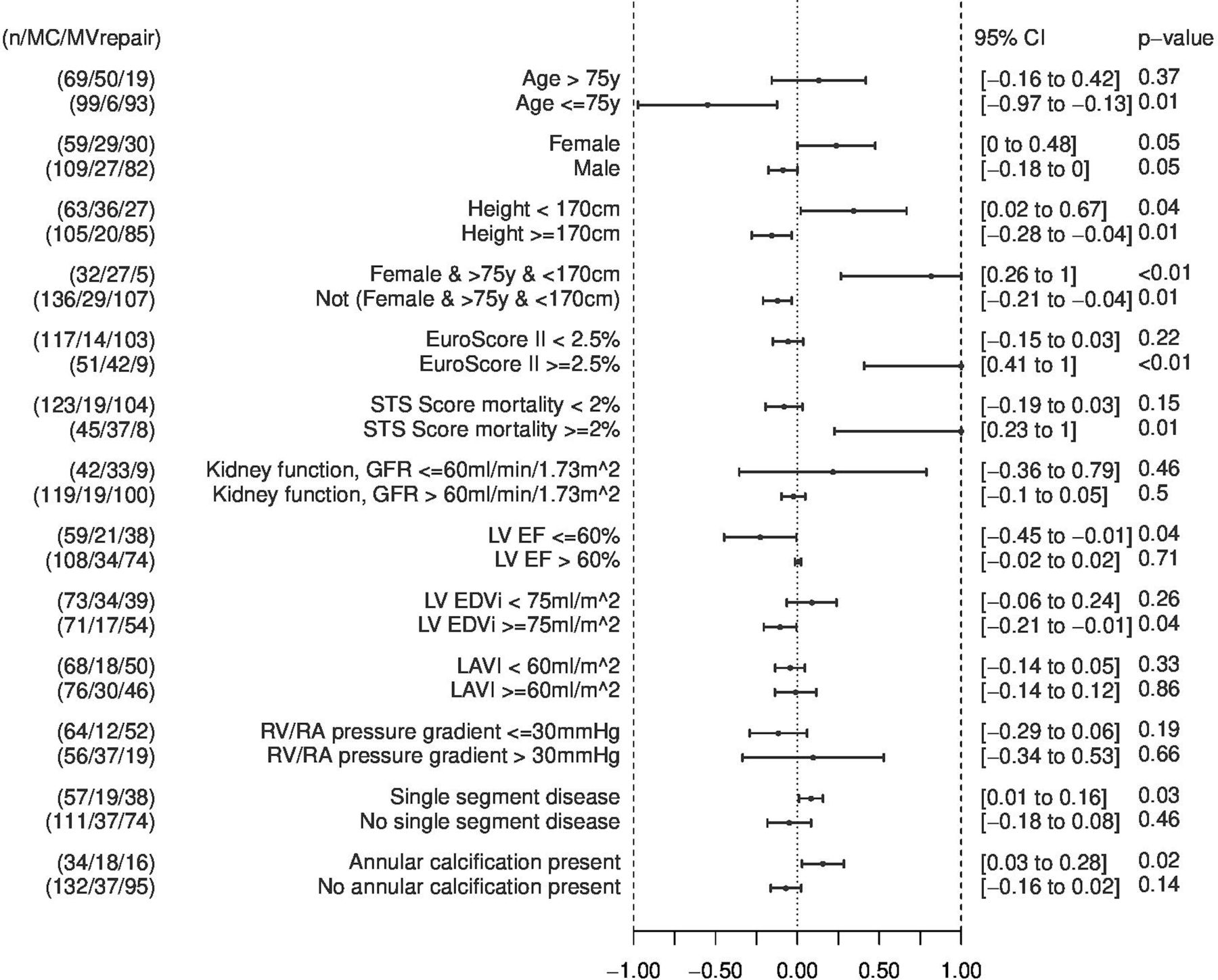
Concomitant heart treatments as well as MR aetiology were additional factors influencing outcome. Patients with combined surgical or percutaneous interventions had a significantly higher all-cause mortality compared with patients with an isolated MV intervention (surgical MV treatment: HR 3.419, 95% CI 1.300 to 8.993, p=0.008; MC patients: HR 2.753, 95% CI 1.569 to 4.832, p<0.001). Furthermore, MC patients with secondary MR had a worse outcome compared with MC patients with a primary MR (figure 2C,D). And in the subgroups of patients with primary MR with an isolated MV treatment (figure 2E,F), the 4-year mortality rates were particularly low in MC patients. Women older than 75 years with small body size appear to profit from the MC procedure when analysing for combined end points at 1 year (figure 3).

Subgroup analysis to evaluate whether MVrepair or Mitraclip may be better for patients with isolated, primary MR. GFR, glomerular filtration rate; LAVI, left atrial volume index; LVEDVi, left ventricular end diastolic volume index; LVEF, left ventricular ejection fraction; MC, Mitraclip; MV, mitral valve; MVrepair, surgical mitral valve repair; RV/RA, rightventricular/right atrial.
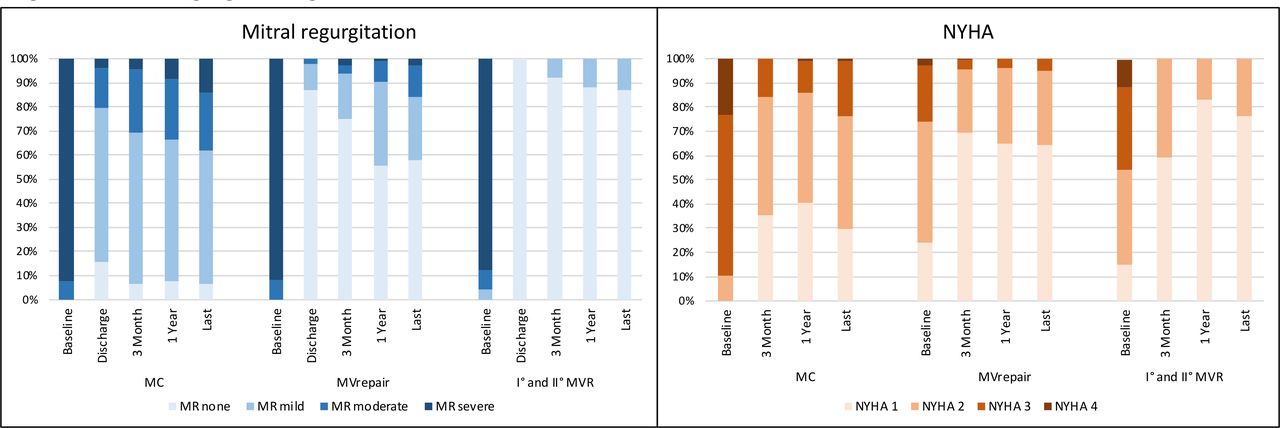
The secondary follow-up end points MR grade and dyspnoea according to NYHA class over time are shown in figure 4.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Mitral regurgitation grade (MR) and dyspnoea (New York Heart Association (NYHA) I–IV) from baseline to the last follow-up examination according to the treatment performed. MC, Mitraclip.
Discussion
MDT decision process
The concept of an interdisciplinary MDT is a centrepiece in modern structural heart disease treatment. Yet, there is no consensus on how the MDT should decide, and evidence supporting the effectiveness of MDT decisions for patients with severe MR is lacking. In our cohort study, we describe the selection process and outcome of an all-comer population with severe MR treated by a dedicated valvular MDT. Counter to the expectations generated by valvular guidelines, the percentage of MR patients assigned to (gold standard) surgical MVrepair was only 46.2%, while 44.8% received percutaneous repair by MC and 9.0% of patients were eligible for primary MVR. In the only other published cohort of patients with MV disease treated according to the MDT decision, the distribution was similar (23% percutaneous and 62% surgical MV repair, 15% MVR).16 In our cohort, mainly patients with primary MR, favourable repair anatomy and low surgical risk were offered surgical MVrepair, while patients with elevated risk or secondary MR were treated percutaneously. Such a consequent selection process was achieved as our MDT has reduced factors often biassing treatment assignment such as patient referral to a specific doctor or financial interest of the individual MDT members.
As additional treatment options such as percutaneous MV replacement will be available in the future, selecting the right patient for the right treatment will be even more challenging.17 18 Percutaneous MVR by compassionate use of TAVR prostheses as valve-in-valve or valve-in-ring showed lower than expected peri-interventional mortality and acceptable mid-term survival in highly selected patients.9 19 Whether the prostheses specifically designed for transcatheter MVR will improve outcome in patients at high risk for treatment failure (ie, calcified leaflets or annulus, high surgical risk) remains to be seen.20
Effectiveness of the MDT treatment decision and room for improvement
The most important question is whether the MDT decision was the right one for the given patient. According to our data, patients assigned to MC achieved a lower in-hospital mortality than expected with surgical treatment, while patients assigned to surgical repair experienced in-hospital mortality rates that met the expectations according to EuroScore II. This was particularly relevant for patients with secondary MR treated by MC, where the reduction of the expected to the achieved in-hospital mortality was largest. Our consequent selection process thus improved the short-term outcome of high-risk surgical patients by assigning them to the lower risk percutaneous treatment option. Furthermore, the benefit of the less invasive percutaneous treatment seemed particularly relevant for MC patients who had isolated, primary MR. Long-term survival rates of these patients was excellent and better than in most previously published series.21 22 In addition, this study corroborates previous data showing a negative impact of concomitant heart treatments on long-term survival and thus emphasises the importance of a careful selection process by the MDT.23
The best treatment option for short elderly patients remains controversial. This study suggests that 1 year outcome for women with an age >75 years and small height (as well as patients with a calcified annulus) might have been further improved if a percutaneous approach had been chosen. Reduced MVrepair rates in women have previously been reported24 and are possibly due to the lack of repair space in shorter elderly women with smaller annular dimensions and limited MV prolapse tissue. Two recent propensity-weighted analyses between surgical and percutaneous MV repair in elderly patients came to opposing conclusions, one favouring surgery and one favouring the percutaneous approach.25 26 The reasons for these discrepant results are unclear and need further analysis by randomised controlled trials.
Limitation
This study has the limitations attributed to its retrospective design and data collection. In addition, the decision-making process was not defined ‘a priori’ but represents the common understanding of our MDT. We cannot exclude that additional factors may have influenced decisions and outcome.
The small number of patients assigned to MVR did prevent further statistical analyses. It may also account for the higher than expected in-hospital mortality in this group (one expected, three actual deaths), a mortality rate comparable to the 5.4% operative mortality in a large series of patients undergoing MVR.27 It does, however, underscore the need for lower-risk percutaneous MV replacement options for this high-risk surgical group.
A similar limitation has to be acknowledged regarding patients with secondary MR. Our team opted for surgical treatment in only 13 patients (9 MVrepair, 4 MVR), as opposed to 64 patients with secondary MR treated by MC. Therefore, this study cannot answer the question which treatment option is best for functional MR.
As we are a tertiary referral centre, patients not eligible for surgical or percutaneous treatment options are sent back to the primary cardiologist for optimal medical care. These (overall few) patients were not included in our study and we do not have follow-up data on them.
Conclusion
This study describes the MDT selection process in assigning patients for MR treatment and relates it to outcome. Only low-risk patients with favourable anatomy were offered MVrepair, while high-risk patients underwent MC or MVR. This strategy was associated with lower than expected in-hospital mortality for MC patients and high 4-year survival rates for MVrepair and MC patients with isolated primary MR.
References
Footnotes
Contributors All authors have contributed significantly to the content of the article. Each one has read and approved the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Obtained.
Ethics approval Written informed consent was given by all patients, and the study protocol was approved by the Cantonal Ethics Commission Zurich (Protocol Number 2017–01895).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available on reasonable request. All data relevant to the study are included in the article.