Article Text

Abstract
Objective Protein-energy wasting is associated with chronic inflammation and advanced atherosclerosis in haemodialysis (HD) patients. We investigated association of geriatric nutritional risk index (GNRI), C reactive protein (CRP) with prediction of mortality after coronary revascularisation in chronic HD patients.
Methods We enrolled 721 HD patients electively undergoing coronary revascularisation. They were divided into tertiles according to preprocedural GNRI levels (tertile 1 (T1):<91.5, T2: 91.5–98.1 and T3:>98.1) and CRP levels (T1:≤1.4 mg/L, T2: 1.5–7.0 mg/L and T3:≥7.1 mg/L).
Results Kaplan-Meier 10 years survival rates were 32.3%, 44.8% and 72.5% in T1, T2 and T3 of GNRI and 60.9%, 49.2% and 23.5% in T1, T2 and T3 of CRP, respectively (p<0.0001 in both). Declined GNRI (HR 2.40, 95% CI 1.58 to 3.74, p<0.0001 for T1 vs T3) and elevated CRP (HR 2.31, 95% CI 1.58 to 3.43, p<0.0001 for T3 vs T1) were identified as independent predictors of mortality. In combined setting of both variables, risk of mortality was 5.55 times higher (95% CI 2.64 to 13.6, p<0.0001) in T1 of GNRI with T3 of CRP than in T3 of GNRI with T1 of CRP. Addition of GNRI and CRP in a model with established risk factors improved C-statistics (0.648 to 0.724, p<0.0001) greater than that of each alone.
Conclusion Preprocedural declined GNRI and elevated CRP were closely associated with mortality after coronary revascularisation in chronic HD patients. Furthermore, combination of both variables not only stratified risk of mortality but also improved the predictability.
- coronary artery disease
- risk factors
- risk stratification
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key question
What is already known about this subject?
Prognosis after coronary revascularisation is consistently poorer in haemodialysis (HD) patients with coronary artery disease (CAD) compared with non-HD patients. On the other hand, the association of malnutrition and chronic inflammation status with poor prognosis has been reported in HD population.
What does this study add?
Preprocedural declined geriatric nutritional risk index and elevated C reactive protein could not only stratify the risk of cardiovascular disease-cause and all-cause mortality after coronary revascularisation but also improve the predictability in HD population with CAD as well as HD population.
How might this impact on clinical practice?
Both variables are easily obtained from daily clinical practice, physicians should pay more attention to comorbidities in HD patients who need coronary revascularisation.
Introduction
Over the past decade, cardiorenal interactions have been featured because patients with chronic kidney disease (CKD) frequently experience cardiovascular disease (CVD) and vice versa.1 Particularly in subjects requiring haemodialysis (HD), coronary artery disease (CAD) reportedly presents in over half of patients, even at the beginning of HD therapy,2 and is the leading cause of death in this population.3 In such situations, coronary revascularisation with coronary artery bypass graft surgery (CABG)4–6 or percutaneous coronary intervention (PCI) is performed in HD patients world wide. However, their prognosis is still markedly poorer compared with that of the general population.4–8 On the other hand, protein-energy wasting (PEW),9 a state of decreased body protein mass and energy fuel, is reportedly prevalent in CKD patients10 11 and consistently associated with increased risks of cardiovascular mortality.12 PEW can result not only from an inadequate diet but also be induced by inflammatory processes.9 13 14 Moreover, inflammatory status itself is associated with mortality in this population.15 In these contexts, we investigated the association of the geriatric nutritional risk index (GNRI)16 as a surrogate marker of the PEW, C reactive protein (CRP) and their combined predictive value for CVD and all-cause mortality after coronary revascularisation in chronic HD patients.
Methods
Patients
From April 2001 to December 2011, a total of 721 HD patients electively underwent coronary revascularisation and were enrolled in this study. In advance, patients with acute myocardial infarction, those hospitalised due to other active diseases and those with a history of malignancies were excluded. Diabetes, hypertension and dyslipidaemia were defined according to each guideline.17–19 Multivessel disease was defined as the presence of a lesion at more than two vessels among the right coronary artery, left anterior descending artery and left circumflex artery and/or left main trunk disease. The left ventricular ejection fraction (LVEF) was measured using the modified Simpson’s method via ultrasonic echocardiography. In patients undergoing CABG, the off-pump technique was selected, and the internal thoracic arteries were used if possible. In patients treated with PCI, drug-eluting stent (DES) was used if the patients had no contraindications.
The GNRI and CRP measurements
Blood samples to determine serum albumin and CRP levels were taken at the just preperiod of procedural day. The GNRI was calculated from the individually obtained serum albumin levels and body weight as follows, reported by Yamada et al.20
GNRI = [14.89×albumin (g/dl)] + [41.7 × (body weight/ideal body weight)]
The body weight/ideal body weight was set to 1 when a patient’s body weight exceeded the ideal body weight. Ideal body weight was defined as the value calculated from height and a body mass index (BMI) of 22 kg/m2.20 All patients underwent HD therapy before 1 day prior procedural day, and body weight after HD therapy was used to calculate the GNRI. The serum CRP was measured using latex-enhanced highly sensitive CRP immunoassay. Thereafter, patients were divided into tertiles according to their GNRI and CRP levels.
Follow-Up study
The follow-up was concluded in December 2012. The primary endpoint was CVD-cause death, including that due to heart failure, myocardial infarction, arrhythmia, sudden death, stroke, peripheral artery disease (PAD) and other CVD-related death. The data for the endpoints were obtained from hospital charts and through telephone interviews with patients conducted by trained reviewers who were blinded to the protocol. In the present study, cases of unwitnessed death were counted as cardiac death. Second endpoint was all-cause death.
Statistical analyses
Variables with a normal distribution were expressed as mean values±SD, and asymmetrically distributed data were given as the median and IQR. Differences between the groups were evaluated by the one-way analysis of variance or Kruskal-Wallis test for continuous variables and by the X2 test for categorical variables. Differences in event-free survival among the groups were examined with the Kaplan-Meier method and compared using a log-rank test. HRs (HR) and 95% CIs were calculated for each factor via a Cox proportional hazards analysis. All baseline variables with p<0.05 by univariate analysis were entered into a multivariate model to determine the independent predictors for the endpoint. To assess whether the predictability for mortality would improve after the addition of the GNRI, CRP and/or both of them into a baseline model with established risk factors, we calculated the C-index, net reclassification improvement (NRI) and integrated discrimination improvement (IDI). The C-index is defined as the area under receiver-operating characteristic curves between individual predictive probabilities for mortality and the incidence of mortality and was compared among each predicting model.21 The NRI relatively indicates how many patients improve their predicted probabilities for mortality, while the IDI represents the average improvement in predicted probabilities for mortality after adding variables into the baseline model.22 Differences were considered statistically significant at p<0.05. The statistical analyses were performed using the SAS V.6.10 software (SAS Institute).
Patient and public involvement
Patients and public were not involved in this study.
Results
Of the enrolled patients, 592 patients underwent PCI and 129 patients underwent CABG based on the decision made primarily by the patients after adequate explanation by their physicians. The patients were divided into tertiles according to their GNRI levels (tertile 1 (T1):<91.5, T2: 91.5–98.1, and T3:>98.1) and CRP levels (T1:≤1.4 mg/L, T2: 1.5–7.0 mg/L, and T3:≥7.1 mg/al). The clinical characteristics of the patients are shown in table 1. The medians of the CRP levels were 5.8 (1.1–18.3) mg/L, 3.0 (1.0–9.0) mg/L, and 2.1 (1.0–8.0) mg/L in T1, T2 and T3 of the GNRI, respectively (p=0.0001). Inversely, the GNRI levels were 95.9±7.6, 95.0±8.3, and 92.6±9.8 in T1, T2 and T3 of the CRP, respectively (p<0.0001).
Clinical characteristics
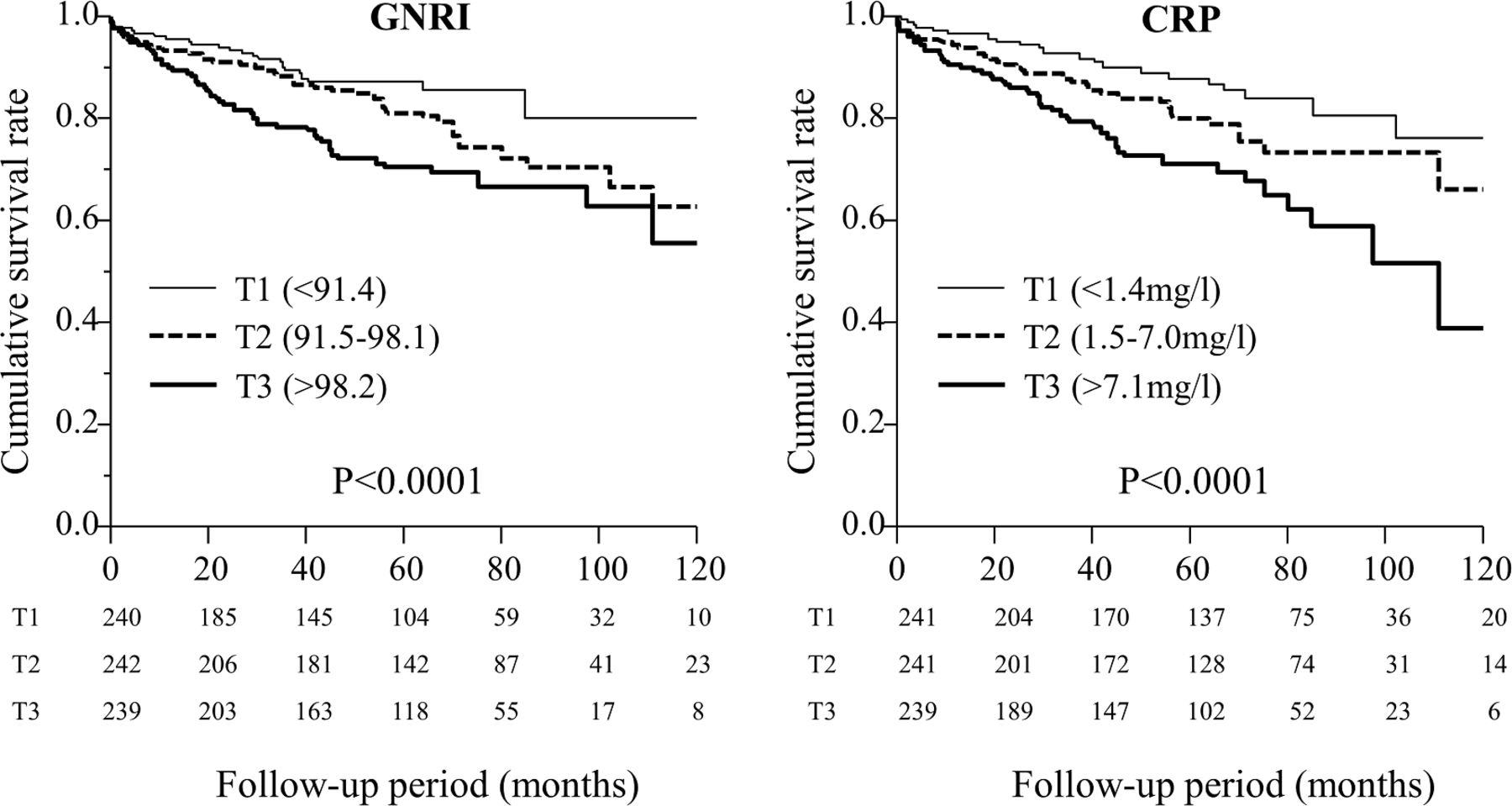
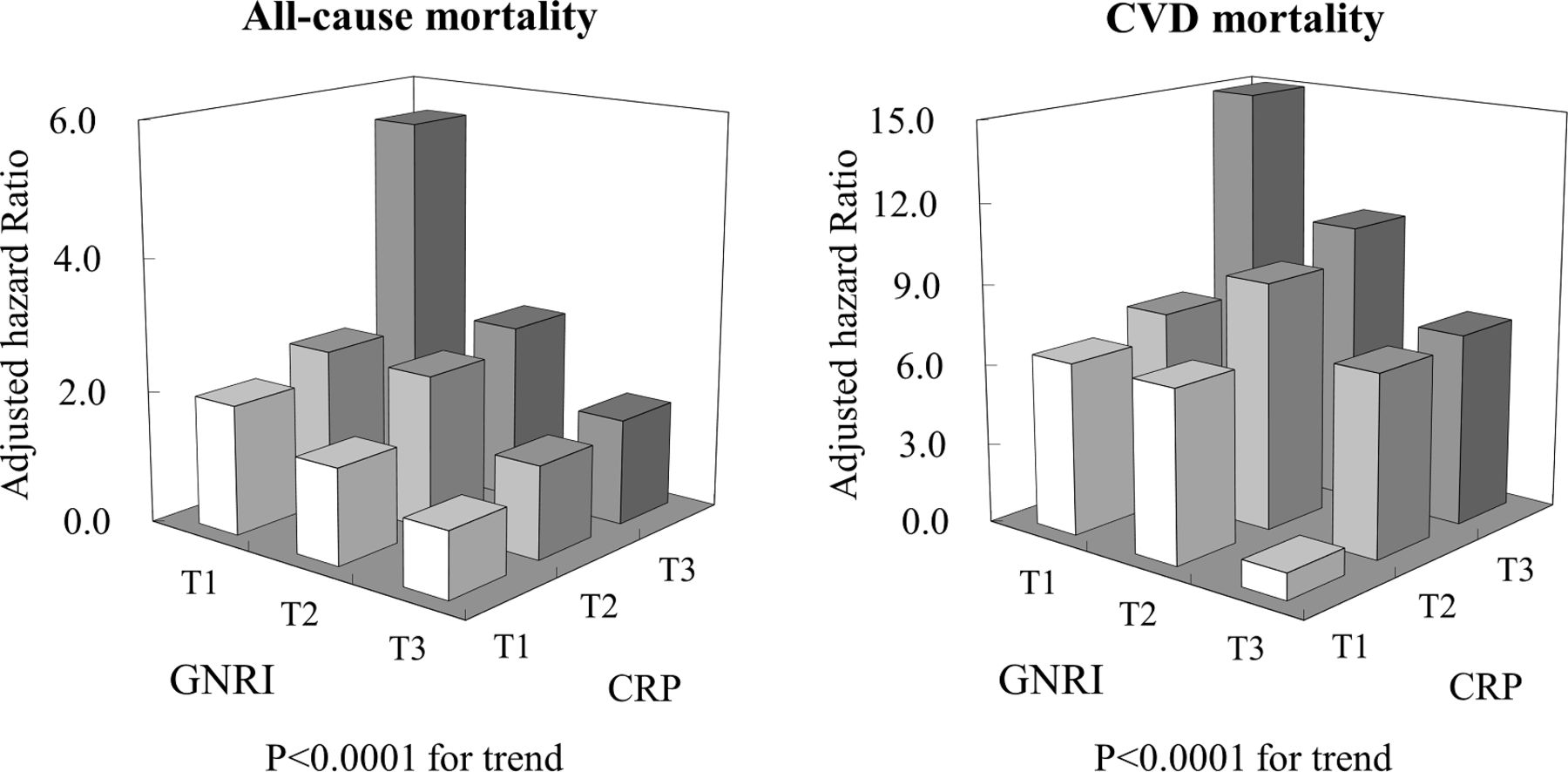
During the follow-up period (median: 53 months), 222 cases experienced death (30.8%), including 125 cases of CV death (17.3%). Also, four patients underwent renal transplantation, and were censored at the point of moving out. The Kaplan-Meier analysis showed that the 10-year survival rate was 32.3%, 44.8% and 72.5% in T1, T2 and T3 of the GNRI and 60.9%, 49.2% and 23.5% in T1, T2 and T3 of the CRP, respectively (p<0.0001 in both) (figure 1). For CVD-cause mortality, similar results were obtained (55.8%, 62.7% and 80.3%, p<0.0001, and 76.2%, 66.2%, and 38.7%, p<0.0001, respectively) (figure 2). After adjusting for age, multivessel disease, and LVEF as covariates with p<0.05 by univariate analysis, a declined GNRI (HR 2.40, 95% CI 1.58 to 3.74, p<0.0001 for T1 vs T3) and elevated CRP (HR 2.31, 95% CI 1.58 to 3.43, p<0.0001 for T3 vs T1) were identified as independent predictors of all-cause mortality (table 2). Similarly, both variables could predict CVD-cause mortality as well (HR 2.45, 95% CI 1.39 to 4.54, p=0.0015 for T1 vs T3 of the GNRI and HR 2.98, 95% CI 1.77 to 5.22, p<0.0001 for T3 vs T1 of the CRP). In addition, the GNRI and log CRP as continuous value were also independent predictors of all-cause mortality (HR 0.96, 95% CI 0.94 to 0.98, p<0.0001 and HR 1.68, 95% CI 1.35 to 2.08, p<0.0001) and CVD mortality (HR 0.96, 95% CI 0.94 to 0.98, p<0.0001 and HR 1.83, 95% CI 1.37 to 2.43, p<0.0001), respectively (table 2). In addition, when diabetes, hypertension, duration of HD and haemoglobin as clinically important factors were added the multivariate Cox model, the GNRI (HR 0.96, 95% CI 0.94 to 0.97, p<0.0001 for CVD mortality and HR 0.96, 95% CI 0.94 to 0.98, p<0.0001 for all-cause mortality) and log CRP (HR 1.81, 95% CI 1.35 to 2.41, p<0.0001 for CVD mortality and HR 1.70, 95% CI 1.34 to 2.11, p<0.0001 for all-cause mortality) were still independent predictors, respectively. In the combined setting of both variables, the risk of mortality was 5.55 times higher (95% CI 2.64 to 13.6, p<0.0001) in the T1 of the GNRI with the T3 of the CRP than in the T3 of the GNRI with the T1 of the CRP (figure 3). Similar results were also obtained for CVD-cause mortality (HR 14.9, 95% CI 5.26 to 247.4, p<0.0001). Furthermore, the addition of both the GNRI and CRP to a prediction model based on established risk factors—including age, multivessel disease and LVEF as covariates with p<0.05 by univariate analysis—improved the C-index (0.648 to 0.724, p<0.0001), NRI (0.539, p<0.0001) and IDI (0.081, p<0.0001) more than each alone (table 3). Similar results were also obtained for CVD mortality (C-index 0.630 to 0.718, p=0.0002, NRI 0.510, p<0.0001 and IDI 0.056, p<0.0001).

All-cause survival after coronary intervention among tertiles according to GNRI and CRP levels. CRP, C reactive protein; GNRI, Geriatric Nutritional Risk Index.
Cardiovascular survival after coronary intervention among tertiles according to GNRI and CRP levels. CRP, C reactive protein; GNRI, Geriatric Nutritional Risk Index.

{kind=link}
{kind=link}
{kind=link}
Adjusted HR of combination of GNRI and CRP for cardiovascular- and all-cause mortality. CRP, C reactive protein; CVD, cardiovascular disease; GNRI, Geriatric Nutritional Risk Index.
Predictive value of GNRI and CRP for cardiovascular-cause and all-cause mortality
Discrimination of each predicting models for cardiovascular-cause and all-cause mortality using C-index, net reclassification improvement (NRI) and integrated discrimination improvement (IDI)
Discussion
Until now, the consistent poorer outcome after, regardless of percutaneous,7 even in the modern DES era,8 or surgical coronary revascularisation,4–6 was considered to be due to various reasons such as complex and/or massive calcified coronary lesions,23 the presence of multivessel disease or an intolerance for procedural invasion due to accelerated systemic atherosclerosis in chronic HD patients.6 Thus, our results suggest that preprocedural PEW and/or chronic inflammation status should be newly added to such numerous prognostic factors after coronary revascularisation in this high-risk population.
We have reported that both a declined GNRI and elevated CRP are closely associated with abnormalities of the ankle-brachial index (ABI) and that the combination of these variables additively increases CVD-cause and all-cause mortality risks in HD patients24 . Other studies have also reported that an abnormal ABI reflects not only PAD but also a systemic atherosclerosis such as overall CVD, including coronary or cerebrovascular diseases.25 26 Thus, our previous report might manifest so-called malnutrition, inflammation and atherosclerosis syndrome in patients with CKD.13 14 In this context, our present findings might be appropriately explained by these previous findings, as HD patients undergoing coronary intervention, regardless of whether it is surgical or percutaneous, are consistently considered to be a highly atherosclerotic group, even among average HD patients.
Moreover, we have already reported that a preprocedural lower BMI and elevated CRP are independently associated with an incidence of lower limb amputation after infrapopliteal bypass surgery in HD patients with critical limb ischemia (HR 0.86, 95% CI 0.76 to 0.97, p=0.014 and HR 1.06, 95% CI 1.01 to 1.11, p=0.014, respectively). However, interestingly, the predictability of both of these variables were not significant in non-HD patients (HR 0.89, 95% CI 0.57 to 1.32, p=0.52, and HR 1.02, 95% CI 0.98 to 1.06, p=0.31, respectively).27 Referring to these results, preprocedural malnutrition and inflammation status might possibly CKD-specifically affect poorer outcomes after, regardless of coronary or lower extremity intervention, compared with non-HD patients.
In addition, it has been reported that predictability for mortality with the GNRI is broadly comparable with the diagnostic criteria of PEW recommended by the International Society of Renal Nutrition and Metabolism (PEW-ISRNM) (C-index: 0.819 vs 0.820, p=0.82).28 Although use of the PEW-ISRNM, including measurement of the mid-arm muscle circumference area or daily protein-energy intake, is accurate to assess PEW, it might be troublesome. In contrast, the GNRI value is easily obtained from daily clinical practice. Therefore, the GNRI may be a useful indicator over the PEW-ISRNM to assess malnutrition in HD patients. In this context, physicians should pay more attention to these pre-procedural comorbidities in this high-risk population.
There are several limitations in the present study. First, all the study subjects were Japanese, who reportedly have a better prognosis compared with patients in the United States and Europe.29 Second, study subjects were included from only two centres. Third, we did not evaluate HD patients without CAD as the control group. Thus, we could not demonstrate more effect of these comorbidities status in patients with CAD compared with those without. Four, we did not consider impact of changes in GNRI and CRP during follow-up period on outcomes. Changes in BMI or albumin is reportedly associated with mortality.30
In conclusion, a preprocedural declined GNRI and elevated CRP, which reflect PEW and chronic inflammation status, are closely associated with CVD-cause and all-cause mortality after coronary revascularisation in chronic HD patients. Furthermore, the combination of both variables could not only stratify the risk of mortalities but also improve the predictability when adding on established risk factors, including age, multivessel disease or LVEF.
References
Footnotes
Presented at A part of this study was previously presented at European Society of Cardiology Congress 2017.
Contributorship Statement Conception and design of the study; YK, HI and HT. Generation, collection, assembly, analysis and/or interpretation of data; YK, SO, RI, NU and HT. Drafting and/or revision of the manuscript; YK, HI andHT. Approval of the final version of the manuscript; YK, HI, HT, SO, RI, NU and TM.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests HI received lecture fees from Astellas Pharma, Astrazeneca, Bayer Pharma, Bristol-Myers Squibb, Chugai Pharma, Daiichi Sankyo and Otsuka Pharma. TM received lecture fees from Bayer Pharmaceutical, Daiichi Sankyo, Dainippon Sumitomo Pharma, Kowa, MSD K.K., Mitsubishi Tanabe Pharma, Nippon Boehringer Ingelheim, Novartis Pharma K.K., Pfizer Japan, Sanofi-aventis K.K and Takeda Pharmaceutical. TM received unrestricted research grant for Department of Cardiology, Nagoya University Graduate School of Medicine from Astellas Pharma, Daiichi Sankyo, Dainippon Sumitomo Pharma, Kowa, MSD K.K., Mitsubishi Tanabe Pharma, Nippon Boehringer Ingelheim, Novartis Pharma K.K., Otsuka Pharma, Pfizer Japan, Sanofi-aventis K.K., Takeda Pharmaceutica, Teijin Pharma.
Patient consent for publication Not required.
Ethics approval The study protocol and chart reviews used were approved by the institutional ethics of both hospitals and conducted in accordance with the Declaration of Helsinki.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available on reasonable request.