Article Text

Abstract
Background The diagnosis and quantification of right-to-left shunt (RLS) using transthoracic echocardiography (TTE) as well as transoesophageal echocardiography (TOE) have not been well established. We aimed to diagnose RLS by TOE using direct visualisation of the shunt and to compare the diagnosis with TTE diagnosis using conventional methods.
Methods and results We evaluated 141 patients with ischaemic stroke for RLS by both non-sedation TOE and TTE using saline contrast and Valsalva manoeuvre. The amount (graded as 0 to IV) and timing of RLS were demonstrated. All patients were classified into four groups by TOE based on direct visualisation of shunt through a patent foramen ovale (PFO) or either pulmonary vein: no shunt (group 1: n=11), PFO (group 2: n=47), pulmonary RLS (group 3: n=25) and indeterminate RLS (group 4: n=58). All cases in group 3 showed delayed shunt, and all cases in group 4 had small shunt. On TTE findings, all cases with early appearing large shunt (cardiac cycles ≤3 and shunt grade ≥III) were group 2. Six of the eight patients with delayed appearing large shunt on TTE were group 3. TTE diagnosis of PFO using criteria of cardiac beats ≤3 and grade ≥II had a sensitivity of 85% and a specificity of 98% compared with TOE diagnosis using shunt visualisation.
Conclusions Compared with TOE using shunt visualisation, TTE accurately diagnosed large PFO using criteria of cardiac cycles ≤3 and shunt grade ≥III. TTE possibly diagnosed pulmonary shunt using criteria of cardiac cycles >3 and shunt grade ≥III. Both modalities showed limitations in diagnosing small amount of RLS.
- right-to-left shunt
- patent foramen ovale
- pulmonary arteriovenous malformation
- agitated saline contrast
- echocardiography
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- right-to-left shunt
- patent foramen ovale
- pulmonary arteriovenous malformation
- agitated saline contrast
- echocardiography
Key questions
What is already known about this subject?
Although both contrast transoesophageal echocardiography (TOE) and transthoracic echocardiography (TTE) have shown the imperfect accuracy in diagnosing right-to-left shunt (RLS), TOE is accepted as a non-invasive standard for diagnosing RLS, and TTE is accepted as a screening test. Direct visualisation of the shunt on TOE was described as the best discriminator for diagnosis of RLS in the guideline. However, no study has diagnosed RLS solely using direct visualisation of the shunt on TOE and compared the diagnostic performance of TTE with the results.
What does this study add?
Compared with TOE using shunt visualisation, TTE using amount and timing of the shunt showed a good performance in diagnosing and discriminating a large amount of RLS. However, TTE showed limitations in diagnosing patent foramen ovale (PFO) with delayed appearing shunt or small amount of shunt. TOE using shunt visualisation also had limitations in discriminating small amount of RLS.
How might this impact on clinical practice?
These results support that contrast TTE is a good screening test to detect and diagnose large RLS. Semi-invasive TOE can be saved for diagnosing PFO with atypical shunting. However, the limitation of TOE in discriminating small amount of RLS should also be considered.
Introduction
Patent foramen ovale (PFO) is a common finding with a prevalence of about 25% in the general population.1 A strong association between PFO and ischaemic stroke has been reported.2 Pulmonary arteriovenous malformation (PAVM) is a rare disease in the general population and causes a permanent right-to-left shunt (RLS).3 The association of pulmonary RLS grade on contrast echocardiography and cerebral complications has also been reported, and embolisation is a first-line treatment of PAVM.4 Recent studies showed that transcatheter PFO closure in adults with cryptogenic stroke significantly reduces the risk of recurrent stroke compared with medical therapy.5–7 With extended therapeutic options for PFO, diagnosis and quantification of PFO are becoming more important in clinical practice.
Although right heart catheterisation with demonstration of a guidewire crossing the septum is the most accurate method for confirming the presence of PFO,8 performing right heart catheterisation to diagnose PFO is not practical considering its invasiveness. Despite the imperfect accuracy of transoesophageal echocardiography (TOE), TOE with bubble test is the accepted noninvasive standard for diagnosing PFO, as it allows quantification of shunt size, documentation of anatomic characteristics and differentiation among PFO, atrial septal defect and pulmonary shunt.9 10 Moreover, recent studies have shown that transthoracic echocardiography (TTE) using agitated saline contrast injection (ASCi) and Valsalva manoeuvre are similar to or better than TOE with various uses of intravenous sedation in the sensitivity of detection of RLS.11–14 TTE using ASCi is now a primary test used to identify the presence of PFO according to the guidelines.15 However, diagnosis of PFO on TTE depends only on microbubble presence and timing in the left chambers, while diagnosis of PFO on TOE can be confirmed by other evidence such as direct visualisation of the shunt, which was described as the best discriminator in the guideline.16 No study has diagnosed PFO or pulmonary shunt on TOE using direct visualisation of the shunt and compared the results with TTE diagnoses using microbubble presence and timing in the left chambers.
We aimed to diagnose RLS using direct visualisation of the shunt on non-sedation TOE and to compare the results with TTE diagnoses using microbubble presence and timing in the left chambers.
Methods
Patients
This prospective study was conducted between January 2013 and December 2017. The study involved consecutive patients referred to the echo-laboratory for TOE to detect RLS. Specifically, we included patients aged ≥18 years who had been referred from the neurological department because of clinically and neuroradiologically verified ischaemic stroke or transient ischaemic attack (TIA). The decision to perform TOE for evaluation of RLS was deferred to the neurologists. Exclusion criteria were atrial fibrillation, significant heart disease including moderate and severe valvular disease, moderate and severe left ventricular (LV) systolic dysfunction, congenital heart disease except PFO and other cardiac source of embolism such as thrombi, tumours or vegetation (figure 1). Patients who were unable to perform the Valsalva manoeuvre in the echo-laboratory before echocardiography were initially excluded. All patients, or a patient’s relative if the patient was incapable of providing consent, gave written informed consent for non-sedation TOE and TTE using ACSi.
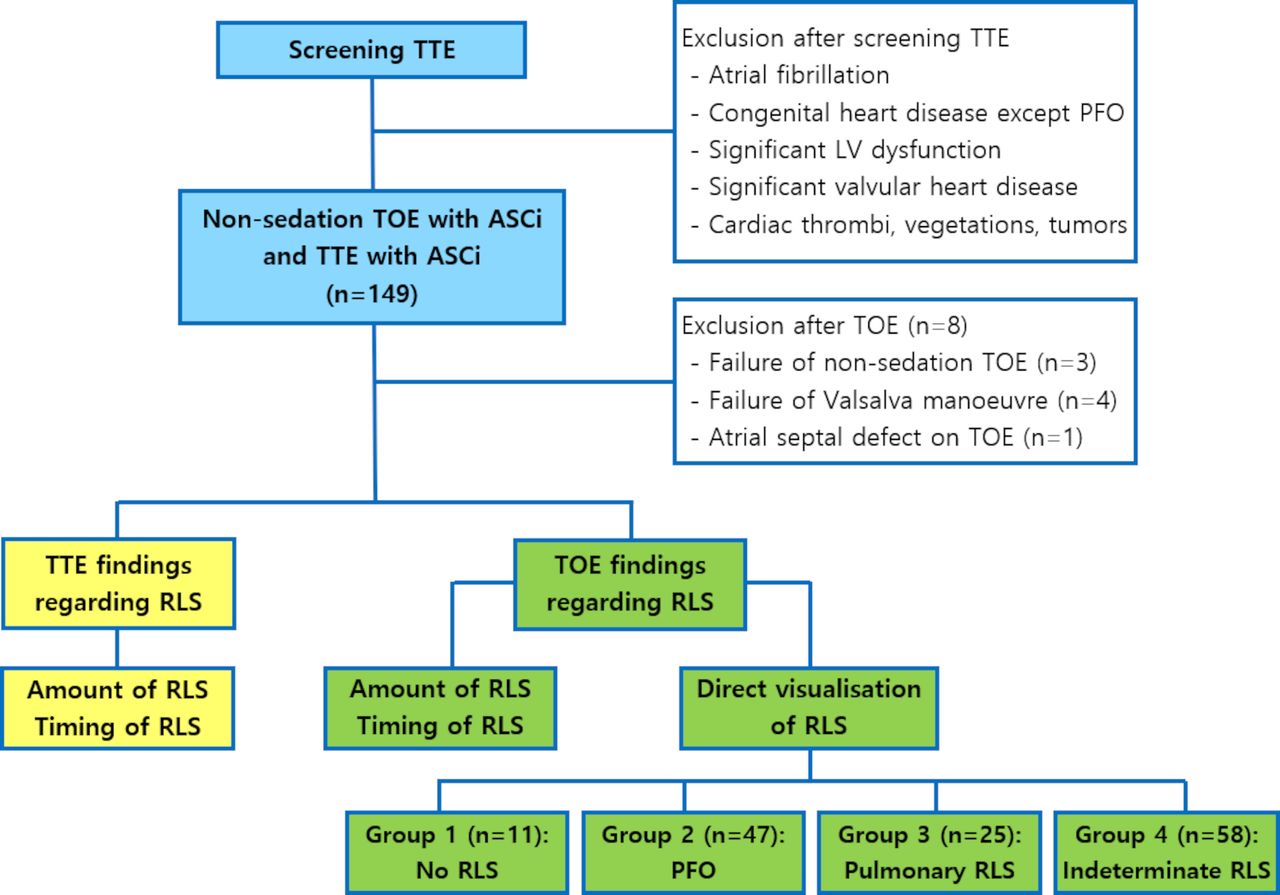
Study flow chart. ASCi, agitated saline contrast injection; LV, left ventricle; PFO, patent foramen ovale; RLS, right-to-left shunt; TOE, transoesophageal echocardiography; TTE transthoracic echocardiography.
Echocardiography
Conventional TTE was performed for every patient according to the established guidelines of the American Society of Echocardiography. Comprehensive TOE evaluation including two-dimensional (2D) echocardiography and colour Doppler study was performed on every patient. Both TTE and TOE were performed using a Vivid E9 or E95 apparatus (GE Vingmed; Horten, Norway) with harmonic imaging. TOE was performed using a 10% topical lidocaine spray for the oropharynx without using intravenous sedation. During TOE, the interatrial septum (IAS) was visualised by 2D echocardiography in the 100°−130° plane (bicaval view) and the 40°−60° plane (basal short axis view), as required to clearly demonstrate the junction of the septum primum and septum secundum of the IAS. In the two views, ASCi was performed both at rest and during Valsalva manoeuvre regardless of the resting RLS. Therefore, at least four movies of IAS imaging with ASCi including two resting and two provocation images were recorded during TOE. If a patient had a suboptimal TOE image or inconclusive RLS, we additionally injected agitated saline and acquired movies once or twice more in a plane showing the clearest IAS image. Movies starting with ASCi and ending at least 10 cardiac cycles after full opacification of the right atrium (RA) were stored. At rest before ACSi, we performed a colour Doppler study focused on possible PFO site to find colour Doppler across PFO. Colour scale and TOE angle were adjusted as required to clearly show colour Doppler. If there were microbubbles seen in the left atrium (LA), we also tried to find the origin of the microbubbles. If there was no direct visualisation of microbubbles coming out of PFO during the release phase of Valsalva manoeuvre, we observed the right and left pulmonary veins to look for microbubble drainage at rest with at least two additional ACSi in each 100°−130° plane and 40°−60° plane focused on the right and left pulmonary vein. TTE using ASCi and Valsalva manoeuvre was performed immediately after non-sedation TOE. On the apical four-chamber view, ASCi was performed during rest and during Valsalva manoeuvre. At least one movie of the apical four-chamber view for resting and two movies for provocation were recorded. The TTE movies were stored in the same manner as TOE movies with repetition in cases with a suboptimal TTE image or inconclusive RLS.
A qualified nurse placed a hand on the patient’s abdomen to check for abdominal muscle contraction while the Valsalva manoeuvre was performed.14 If a patient did not show adequate abdominal muscle contraction, he or she was induced to cough. If a patient failed to perform adequate abdominal muscle contraction or cough despite multiple attempts, the case was considered as failure to perform the Valsalva manoeuvre and additionally excluded in the analysis. Saline contrast was prepared by agitating 1 mL of air with 9 mL of sterile saline solution using two 10 mL syringes and a three-way stopcock. Saline contrast was rapidly injected through an antecubital vein using an 18-gauge venous cannula. Each injection was administrated at rest and before the release phase of a Valsalva manoeuvre. The Valsalva manoeuvre was released immediately after a bolus of microbubbles arrival into the IAS. One experienced echocardiologist evaluated the findings of TOE and TTE. TOE and TTE recordings were independently analysed in a blinded manner for the other examination. Some patients who were diagnosed with extracardiac shunt on echocardiography underwent chest CT scan. Chest CT scan was not included in the study protocol, but we reviewed the results for these patients.
Definitions
A positive RLS was diagnosed when at least one definite microbubble was seen in the left chambers in recorded movies using ASCi. The amount of RLS was semiquantified as grade 0 (no microbubble), grade I (1–5 microbubbles), grade II (6–20 microbubbles), grade III (21–50 microbubbles) and grade IV (>50 microbubbles). Grade I or II were considered as small RLS and grade III or IV as large RLS according to the previous studies.14 17 18 The number of microbubbles in the LA (TOE) and the LV (TTE) was counted in a single frame showing the maximal number of microbubbles. Although we graded both rest and provocation images separately, we analysed the amount, timing and diagnosis of RLS using provocation images. In order to define the timing of RLS, the number of cardiac cycles when early microbubbles started to be seen in the LA (TOE) and the LV (TTE) after RA opacification were counted. On TOE, we intended to diagnose RLS with direct visualisation of the shunt. Direct visualisation of the shunt was defined as visualisation of microbubble origin through PFO or pulmonary veins or colour Doppler across PFO. A colour Doppler across PFO was defined as left-to-right colour Doppler between the septum primum and septum secundum at rest (figure 2A). A direct visualisation of PFO was defined when microbubbles exiting from the RA between the septum primum and septum secundum at the release of the Valsalva manoeuvre were seen (figure 2B). The direct visualisation of pulmonary shunt was defined when microbubbles were observed inside the right or left pulmonary veins and moved to the LA (figure 2C). Using these definitions, we classified the TOE findings into four groups: group 1 without RLS, group 2 (PFO) showing colour Doppler or microbubbles across the PFO, group 3 (pulmonary RLS) showing microbubbles coming from either pulmonary vein and group 4 (indeterminate RLS) showing microbubbles in the LA but demonstrating no definite visualisation of RLS origin. Both TTE and TOE findings were analysed according to the amount (grades) and the timing (cardiac cycles) of RLS. PFO diagnosis on TTE was defined primarily as RLS with early appearance (within three cardiac cycles) of microbubbles using Valsalva manoeuvre.

Transoesophageal echocardiographic images. A1 and A2: Resting colour Doppler images of a patent foramen ovale. B1 and B2: direct visualisation of shunt through a patent foramen ovale. C1 and C2: direct visualisation of shunt coming from the right (C1) and left (C2) pulmonary veins. An arrow in each image indicates the point of microbubble origin.
Statistics
Categorical variables are presented as a number and percentage (%). Continuous variables are expressed as mean±SD. Sensitivity and specificity tests were used to compare TTE diagnosis with TOE diagnosis for PFO. Statistical analyses were performed using SPSS V.21.0 software.
Results
Patients
Of 149 patients who underwent non-sedation TOE and TTE with ASCi, 141 (89 men, mean age 54±13.6 years) were included and analysed in this study (figure 1), and the clinical characteristics of the study patients are shown in table 1. Eight patients were excluded because of failure of non-sedation TOE (n=3), failure of adequate Valsalva manoeuvre (n=4) and atrial septal defect on TOE (n=1) after TOE. On TOE, 136 patients showed optimal image quality for counting microbubbles in the LA and five patients showed suboptimal image quality. On TTE, 122 patients had optimal image quality for counting microbubbles in the LV and 19 patients had suboptimal image quality. However, with repeated image acquisition, semiquantification of the amount of RLS was achieved in all patients including cases with suboptimal images on TOE or TTE. With one microbubbles cut-off in the LA or LV, the rate of positive RLS was very high on both TOE (92.2%) and TTE (83.7%) in this population.
Baseline characteristics
TOE findings
By shunt visualisation on TOE, 11 (7.8%) patients were classified into group 1 (no shunt), 47 (33.3%) patients were classified into group 2 (PFO), 25 (17.7%) patients were classified into group 3 (pulmonary RLS) and 57 (40.4%) patients were classified into group 4 (indeterminate RLS) (figure 1). Atrial septal aneurysm was observed in 14 (9.9%) patients. Among them, eight patients were included in group 2. In group 2, 19 patients showed resting colour Doppler and among them seven patients (five in grade I, two in grade II) showed a small amount of RLS. Of 25 patients in group 3, 19 patients underwent chest CT, and only three patients were diagnosed with PAVM by chest CT. All the three patients had grade IV RLS on TOE. Figure 3 (left) showed shunt grade and timing in patients (n=130) with group 2, 3 and 4 on TOE. All cases in group 3 showed delayed shunt, and all cases in group 4 had small shunt.

{kind=link}
{kind=link}
{kind=link}
TOE (left) and TTE (right) graphs showing the amount and timing of shunt in 130 cases with shunt on TOE with Valsalva manoeuvre (11 cases without shunt on TOE are not shown in this figure). The x and y coordinates indicate cardiac cycles after right atrial opacification and grade of the shunt. Cases with black, red and green indicate inclusion in groups 2, 3 and 4, respectively, in both graphs. TOE, transoesophageal echocardiography; TTE, transthoracic echocardiography.
TTE findings compared with TOE
Figure 3 (right) demonstrates the shunt grade and timing in patients (n=130) with groups 2, 3 or 4. On TTE, all cases with early appearing large shunt (cardiac cycles ≤3 and shunt grade ≥III) were group 2. Six of the eight patients with delayed appearing large shunt were group 3. A large proportion of patients showed a delayed appearing small shunt on TTE-like TOE. They were included in groups 2, 3 or 4. According to the quantitative criteria for PFO diagnosis, sensitivity and specificity of TTE diagnosis compared with TOE diagnosis using direct visualisation were different (table 2). With PFO diagnosis criteria using cardiac cycles ≤3 and shunt grade ≥I, ≥II or ≥III, sensitivity and specificity of TTE were 89% and 95%, 85% and 98% or 74% and 100%, respectively.
Comparisons of diagnosis of patent foramen ovale between transthoracic echocardiography (TTE) and transoesophageal echocardiography (TOE)
Discussion
In the current study, we demonstrated the detailed amount and timing of RLS in all cases on saline contrast TTE and TOE and diagnosed the RLS with direct visualisation of the shunt on non-sedation TOE. To our knowledge, there are no other published reports that compare TTE results of RLS with TOE result of RSL based on direct visualisation of the shunt and that show sensitivity and specificity of PFO diagnosis on TTE with different quantitative criteria for PFO. Many previous studies compared accuracy of TTE and TOE for diagnosis of intracardiac shunt using TOE (based on microbubbles) as the gold standard or using PFO diagnosis confirmed with TTE or TOE. Those studies have shown different conclusions. Mojadidi et al and Clarke et al showed a low sensitivity and a high specificity of TTE (46% sensitivity and 99% specificity; 68% sensitivity and 93% specificity, respectively) compared with TOE.18 19 Other studies showed a higher sensitivity of TTE than that of TOE (94% sensitivity for TTE and 39% sensitivity for TOE, 86% sensitivity for TTE and 55% sensitivity for TOE) using PFO diagnosis confirmed with TTE or TOE.12 13 The other study showed good agreement in RLS diagnosis of TTE (99% sensitivity and 85% specificity) compared with TOE.11 Those different results might be caused by different methods and different standards. Low sensitivity of TOE in previous studies seemed to be related with ineffective Valsalva manoeuvre and sedation during TOE. We showed the different sensitivity and specificity of TTE diagnosis (ranged from 74% to 89% and from 95% to 100%, respectively, in table 2) compared with non-sedation TOE diagnosis based on direct visualisation according to the quantitative criteria for PFO.
Patent foramen ovale
The prevalence of PFO among patients with a cryptogenic stroke has been reported as 28%–50%.2 20 21 In this population, 33% of patients had a PFO by a PFO definition using direct visualisation of shunt on TOE and 30% (TOE) and 33% (TTE) of patients were diagnosed with a PFO by a PFO definition using the shunt timing (≥grade I, within three cardiac cycles after RA opacification). Most previous studies diagnosed PFO only using left heart contrast and cardiac cycles after RA opacification, but the definition for quantity of left heart contrast and cardiac cycles varies among studies. Different studies defined the positive contrast as at least one, three or five microbubbles.11–14 22 Cardiac cycles after RA opacification to define PFO separate from extracardiac shunt have also differed among studies mostly using 3–5 cardiac cycles.2 11–14 As we showed in figure 3, there were many cases in the range of 1–5 microbubbles and 3–5 cardiac cycles. That seems to be one explanation for why PFO diagnosed by TOE or TTE is not always accurate. Our grouping using direct visualisation of the shunt on TOE showed limitations in diagnosing cases with small shunt. False positive cases of PFO in TTE (table 2) might not be false positive cases but can be just small PFOs that were not diagnosed by direct visualisation of the shunt on TOE. However, most patients with grade II or more RLS and all patients with grade III or more RLS could be characterised without using cardiac cycles on TOE. Therefore, careful observation of the origin of RLS on TOE seemed to compensate for the limitation of cardiac cycles. Because of more effective Valsalva manoeuvre achieved by avoiding intravenous sedation and repeating attempts during TOE, the direct visualisation of microbubbles crossing the IAS was likely observed in most PFO cases in this study. Noticeably, some cases with resting colour Doppler across the IAS and even visual gap in the IAS showed small numbers of microbubbles or delayed bubble appearance despite an expectation of typical PFO shunting (early and large RLS). Therefore, those cases would most likely be undiagnosed as a PFO by contrast TTE. There are several mechanisms of false-negative saline contrast for detecting PFO, including the ineffective provocation test and increased left heart filling pressure.23 Siostrzonek et al24 demonstrated a lower prevalence of PFO in patients with left heart disease than in healthy patients. The cases with resting left-to-right shunt (colour Doppler) through PFO seemed to have high left atrial pressure which might prevent large RLS despite Valsalva manoeuvre.
Pulmonary shunt
We defined pulmonary shunts as cases with visible microbubbles drained from the right or left pulmonary veins on TOE. Because many cases with pulmonary drainage of microbubbles on TOE did not show a detectable PAVM on chest CT, we did not define those as PAVMs in this study. Gazzaniga et al25 showed similar results to ours regarding PAVMs in their contrast TTE study in patients with hereditary haemorrhagic telangiectasia. They semiquantified shunt size as grade 0 (no bubbles), 1 (<20 bubbles), 2 (moderate filling) and 3 (complete opacification). They reported no PAVMs on chest CT in 132 patients with grade 0 or 1, PAVMs in 11 of 25 patients with grade 2 and PAVMs in all 21 patients with grade 3. Similarly, in the current study, all three cases with PAVMs confirmed on chest CT showed grade IV RLS. Even though PAVM has been defined in many echocardiography studies based on delayed appearance of microbubbles, the delay depends on the quantity, anatomic locations and sizes of PAVMs, and a delay of 2–8 cardiac cycles has been described.26 27 According to our results, large amount and delayed RLS was a characteristic finding of PAVMs.
Indeterminate shunt
We found that many cases with a small delayed shunt were not diagnosed with PFO or pulmonary shunt by direct visualisation of the shunt and classified as indeterminate shunt. Because of the cases with indeterminate shunt, a small delayed shunt on Valsalva manoeuvre, the positivity of RLS in this study was very high. Although we defined those as indeterminate shunts, we consider those to be pulmonary shunt but not to be PAVM. It was reported that contrast echocardiography studies were frequently positive in normal lungs without any detectable impairment of gas exchange.25 28 29 Shovlin et al explained this phenomenon as ‘alvelolar transit’ bubbles that have passed though the capillaries but have not fully collapsed, and another study explained it as ‘microscopic PAVM’.26 30 This phenomenon was observed more commonly on exercise and in other high cardiac output states than at rest in the general population.28 29 Three small studies demonstrated that high rates of pulmonary shunt (89% (8/9), 88% (7/8) and 91% (21/23)) in healthy men and women with exercise compared with those (33% (3/9), 25% (2/8) and 0% (0/23), respectively) in resting condition.31–33 Interestingly, we observed small delayed shunts more frequently with Valsalva manoeuvre than at rest. Therefore, we suspected that some changes like those induced by exercise in pulmonary capillary bed might be induced by Valsalva manoeuvre, and this phenomenon might resulted in high positive rate of RLS during Valsalva manoeuvre in the current study.
Limitations
This study was conducted in a single centre and used echocardiographic machine with the same image setting and vendor, which may prevent us from generalising the results to other centres using different machines with various image settings. Our study population was not a single well-defined group such as a patient group with cryptogenic stroke because we included all cases referred for saline contrast TOE if they had an ischaemic stroke or TIA. Therefore, it was difficult to compare the prevalence of PFO and RLS with other studies conducted in patients with cryptogenic stroke. Adequate Valsalva manoeuvre was not assessed based on objective findings, such as deviation of the IAS or decreased E velocity but was evaluated only based on abdominal muscle contraction judged by a qualified nurse.
Conclusions
Compared with TOE diagnosis using direct visualisation of the shunt, TTE accurately diagnosed large PFO using criteria of cardiac cycles ≤3 and shunt grade ≥III. PFO with a delayed shunt was not diagnosed by TTE but only diagnosed using direct visualisation by TOE. TTE possibly diagnosed pulmonary shunt using criteria of cardiac cycles >3 and shunt grade ≥III. Both modalities showed limitations in diagnosing small amount of RLS. The clinical significance and appropriateness of further study for a small RLS need to be investigated.
References
Footnotes
Contributors ML designed study and data collection tools, monitored data collection for the whole trial, wrote the statistical analysis plan, cleaned and analysed the data and drafted and revised the paper. JHO monitored data collection and analysed the data, and revised the paper.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval This study was approved by the ethical committee of the institutional review board of our hospital and waived the requirement for informed consent regarding the use of their diagnostic data in research using offline image analysis.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available on reasonable request. Data are available in a public, open access repository.