Article Text

Abstract
Background Balloon aortic valvuloplasty (BAV) has seen renewed interest since the advent of transcatheter aortic valve implantation (TAVI). The study aimed to characterise a contemporary BAV cohort and determinants of clinical outcomes.
Methods Patients undergoing BAV at a single tertiary centre were retrospectively reviewed over a 10-year period, and functional and mortality outcomes were reported with up to a 2-year follow-up.
Results 224 patients (aged 82.5±8.3 years; 48% female) underwent BAV over the study period. Indications were either destination treatment (39%) or bridge-to-valve replacement (61%)—including bridge-to-decision (29%), symptom relief while on the waitlist (27%), and temporary contraindications to TAVI/aortic valve replacement (AVR) (5%). The mean reduction of aortic mean pressure gradient was 38%. Procedural mortality occurred in 0.5%, stroke in 1.3%, and major bleeding in 0.9%. Twelve-month mortality was 36% overall, and 26% and 50% in the bridging and destination groups, respectively. New York HeartAssociation (NYHA) class improved by ≥1 at 30 days in 50%. Among the bridge-to-TAVI/AVR group, 40% proceeded to TAVI/AVR within 12 months following BAV. In multivariate analysis, active malignancy at baseline (OR: 4.4, 95% CI: 1.3 to 15.1, p=0.02), smoking history (OR: 3.3, 95% CI: 1.3 to 7.9, p<0.01), LVEF ≤30% at baseline (OR: 3.2, 95% CI: 1.3 to 7.6, p<0.01), destination treatment (OR: 2.2, 95% CI: 1.0 to 4.9, p=0.04) were all associated with 12-month mortality.
Conclusions BAV remains a useful procedure with relatively low rates of complications, however, 1-year mortality rates are high. Contemporary indications for BAV include a bridge to definitive valve replacement or destination treatment.
- aortic valve disease
- valvuloplasty
- valvular disease
- quality of care and outcomes
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known about this subject?
Balloon aortic valvuloplasty (BAV) has had a resurgence of interest since the advent of transcatheter aortic valve implantation. BAV may be used as a destination treatment for symptom improvement or as a bridge to transcatheter aortic valve implantation or surgical aortic valve replacement to stabilise patients while awaiting a definitive procedure.
What does this study add?
This study concludes that BAV remains a safe, useful procedure for severe aortic stenosis, with low rates of complications, however, 1-year mortality rates are high. Predicting functional response following BAV has not previously been well studied, and symptomatic patients (New York Heart Association (NYHA) 3 or 4), female patients and obese patients were identified as the groups most likely to benefit from this procedure.
How might this impact on clinical practice?
BAV is a useful clinical tool as destination therapy, where it provides effective symptomatic relief over 6–12 months, or as a bridge to definitive treatment where it can be used as a stratifying tool for clinical decision making on valve replacement, as a measure to address issues that pose temporary contraindication to TAVI/AVR and to offer symptomatic improvement to patients with prolonged waiting time, especially among the select groups identified in this study.
Introduction
Aortic stenosis (AS) is the most common valvular pathology in the elderly population and the preferred treatment in higher-risk populations has undergone major changes over the last 10 years with the development of transcatheter aortic valve implantation (TAVI).1–3 In this setting, there has been renewed interest in balloon aortic valvuloplasty (BAV), with increasing procedural numbers both in the USA4 5 and other countries,6 7 which is a marked change from the previous steady decline since its early peak in the 1990s.8 Initially proposed as an alternative to surgical aortic valve replacement (AVR),9 BAV was shown to improve symptoms, although with significant complication rates and no long-term survival benefits.9–12 Traditional indications for BAV have been limited to poor surgical candidates and have included cardiogenic shock,8 13 preoperative optimisation14 and symptomatic improvement with palliative intent.9 11 12 15 Recently, a more contemporary indication for BAV has included its utilisation as a bridge to either surgical or transcatheter AVR in patients who may have a temporary contraindication,16 who may derive uncertain benefit from TAVI or AVR,16–19 or when valve replacement is not immediately available.6 7 16 19–23 Recent data suggest that emergency TAVI has a poor outcome, whereas BAV treatment may give time to prognosticate more accurately.24 Timely TAVI availability remains an important concern among this population given the high mortality among patients with severe AS and the potential for death among waitlisted patients,25 which may potentially be reduced with bridging BAV given its effect on initial improvement in survival.26 This study aimed to assess contemporary indications and outcomes for BAV, as well as to identify factors that predict functional, haemodynamic and mortality benefits to highlight select patient groups that may benefit most from BAV procedures in the TAVI era.
Materials and methods
Consecutive patients undergoing BAV for severe aortic stenosis from February 1, 2008 to September 1, 2017 at The Alfred Hospital, a large tertiary referrals centre in Melbourne, Australia, were retrospectively identified from the hospital cardiac database. Severe aortic stenosis was determined by transthoracic echocardiography prior to the procedure and was defined as either aortic valve area (AVA) <1.0 cm2, Dimensionless Performance Index (DPI)<0.25 or mean gradient ≥40 mm Hg in the setting of normal left ventricular (LV) function on transthoracic echocardiography. Severe aortic stenosis in the setting of abnormal LV function was determined by an increase in mean gradient to ≥40 mm Hg with dobutamine stress transthoracic echocardiogram (TTE) or by Heart Team assessment. Patients with mixed aortic valve disease (moderate or severe aortic regurgitation in addition to AS) are not assessed for BAV at our centre and are not included in the study. The project was approved by the Alfred Hospital Ethics Committee.
Demographic data were obtained through a detailed review of the hospital electronic medical records to determine patient demographics, comorbidities, cardiovascular risk factors, cardiac symptoms and presence of cardiogenic shock prior to the procedure. Functional status was determined from medical records by trained medical personnel by applying New York Heart Association (NYHA) criteria to the nearest clinical encounter describing functional ability within 30 days preceding BAV procedure. Indication for BAV was determined by clinician intent at the time of BAV procedure (eg, bridge-to-TAVI/AVR) and patients remained in their intention-to-treat grouping irrespective of the eventual outcome (ie, bridge-to-TAVI and bridge-to-AVR patients did not necessarily receive a valve replacement procedure). Throughout the study period, over 300 TAVI procedures were performed at our institution, with 70 TAVIs performed in 2016 and >90 procedures projected for 2017.
BAV procedures were performed by three individual operators (SD, AW, DS) using standard techniques via the retrograde femoral approach in all patients. Peak and mean gradient measures were confirmed with simultaneous catheter gradient measures. NuMED NuCLEUS and Pyramed Cristal aortic balloons are used at our institution. Sheath size, balloon size, preprocedural and postprocedural haemodynamics, immediate complications and in-hospital mortality were determined from the electronic procedural and clinical records. In-hospital complications, including myocardial infarction and stroke, were defined according to the Academic Research Consortium definitions.27 Significant bleeding was defined as Bleeding Academic Research Consortium Classification Type 3 or 5.28 Acute kidney injury (AKI) following BAV was defined as increase in serum creatinine ≥26.5 μmol/L within 48 hours or increase in creatinine to ≥1.5 times baseline taken within the prior 7 days according to Kidney Disease: Improving Global Outcomes (KDIGO) criteria.29
Patient outcomes were assessed at 30 days, 6 months and 12 months post procedure. Clinic notes and subsequent admissions were used to determine NYHA functional status and hospital readmission rates. TTE reports were reviewed to determine LV ejection fraction (LVEF), AVA, LV end-diastolic diameter (LVEDD), E/e’ and severity of mitral regurgitation (trivial, mild, moderate or severe). Patient mortality was assessed to at least 12 months using clinical records and telephone follow-up, with days from procedure to death used to generate Kaplan-Meier survival curves. If a patient received TAVI or AVR during the 12 months post BAV, then they were no longer included in functional or TTE response after this point, however, continued to be followed for postprocedural mortality to at least 12 months. If a patient received a repeat BAV within 12 months, then the patient was censored from follow-up at the time of repeat BAV and included as a new procedure.
Statistical analysis was performed using Stata V.14.2 for Macintosh. All categorical variables are presented as frequencies and percentages and continuous variables are presented as mean±SD. Comparisons between groups were performed with the χ2 test for categorical variables and Student t test for continuous variables. Multivariate analysis was performed using logistic regression to determine independent predictors of 12 month mortality, functional response (defined by NYHA score improvement ≥1 at 30 days) and haemodynamic response (defined by improvement in LVEF by ≥10% at 30 days). Variables with a p<0.10 in univariate analysis were considered for inclusion in multivariate analysis. The cumulative probability of survival was estimated by Kaplan-Meier curves, with survival between indication groups compared using the log-rank test. All calculated p values were two-sided and p values of <0.05 were considered statistically significant.
Results
Two hundred and twenty-four patients were included in the cohort; the mean age was 82.5±8.3 years, and 47.8% were female (table 1). Procedural numbers increased across the study period, mainly driven by an increase in the number of bridge-to-TAVI/AVR procedures performed, in line with an increase in TAVI procedural numbers across the same period (figure 1).
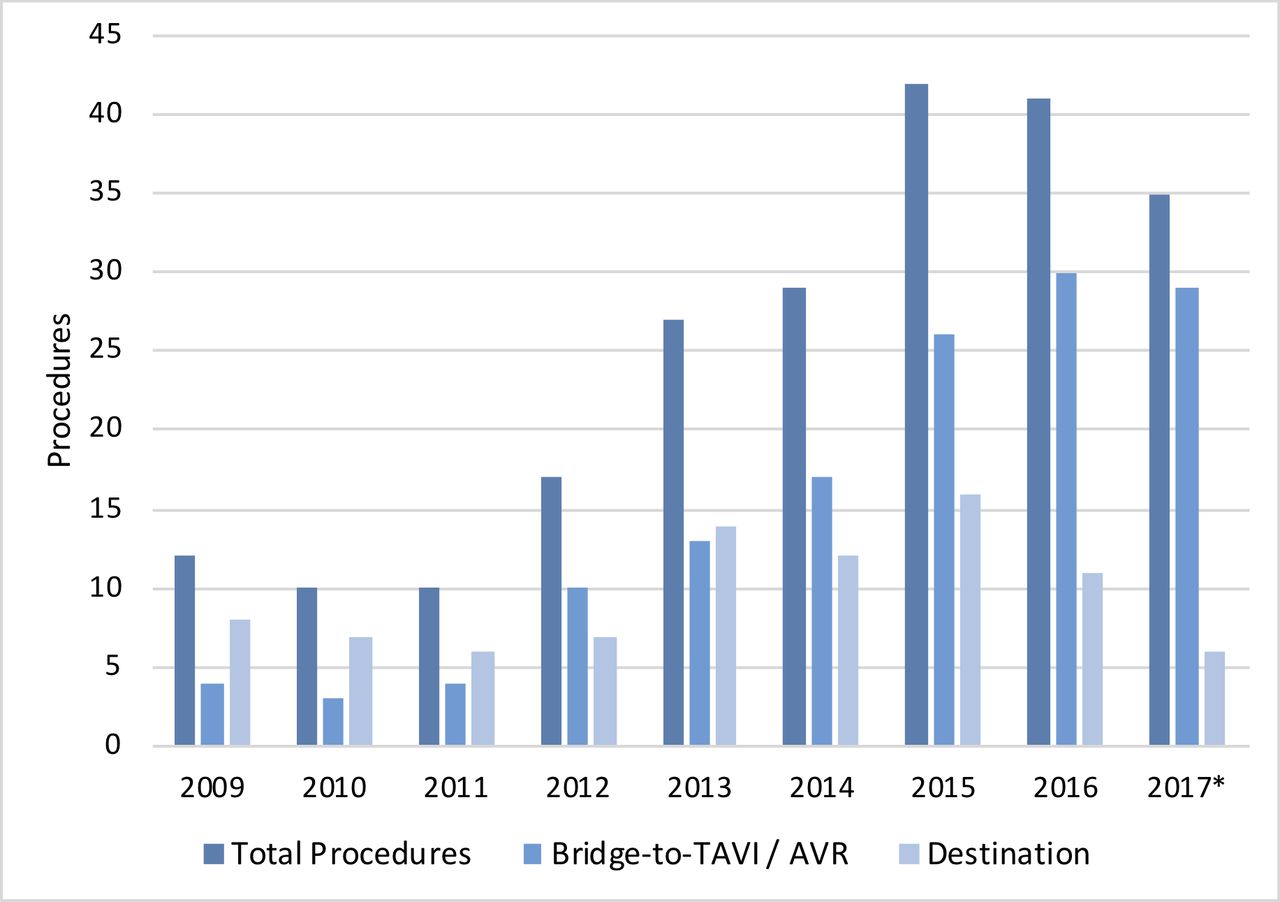
Procedural numbers by indication – procedural numbers at a single institution over a 9-year period. *2017 data only includes up to September 2017 (with projected numbers for the 2017 calendar year being 45 bridge-to-TAVI/AVR procedures and 8 destination procedures). AVR, aortic valve replacement; TAVI, transcatheter aortic valve implantation.
Baseline characteristics
Baseline clinical characteristics were similar in the bridge-to-TAVI/AVR and destination indication groups, however, there was a higher rate of prior BAV in the destination group (15.9% vs 5.9%, p=0.01). Syncope was more common among the bridge-to-TAVI/AVR group (p=0.05), whereas cardiogenic shock was more common in the destination group (p<0.01). Mean Society of Thoracic Surgery (STS) Risk Score was lower in the bridge-to-TAVI/AVR group (6.4±0.3% vs 8.7±0.7%, p<0.001). Baseline echocardiographic data are presented in table 1, with the destination group having lower mean LVEF (43.6±18.5% vs 50.3±18.5%, p<0.01), and higher mean E/e’ ratios (27.0±14.0 vs 20.5±8.9, p<0.001) compared with the bridge-to-TAVI/AVR group. Indications for BAV are presented in table 2.
Indications for BAV
Procedural characteristics are presented in table 3. One hundred and nine procedures (48.7%) were performed electively, with 84 of these (37.5%) performed at the time of TAVI workup with coronary and peripheral angiography. The mean gradient reduction was 15.9±9.5 mm Hg, with 144 procedures (66.4%) reducing the gradient by ≥30%. Balloon size used was 18 mm in 56.6%, 20 mm in 23.7% and 22 mm in 11.4%, with other sizes being less common.
Procedural characteristics and complications
Major vascular complications occurred in 3.1%, stroke in 1.3%, major bleeding in 0.9% and in-hospital mortality was 2.2%. Procedural mortality occurred in only one patient due to acute aortic regurgitation, while undergoing urgent inpatient BAV for intractable NYHA class 4 symptoms in the setting of low-flow AS. An 18 mm balloon size was used with single inflation, and no clear precipitant for acute aortic regurgitation was identified. There were no significant differences in procedural characteristics or in-hospital complications between the bridge-to-TAVI/AVR cohort and the destination cohort.
For destination and bridge-to-TAVI/AVR groups, mortality was 50.0% and 26.3% at 12 months (p<0.01), respectively (table 4). Eighty-six patients had a repeat aortic procedure: 18 patients had repeat BAV (median time to BAV 357 days), 56 patients proceeded to TAVI (median time to TAVI 135 days) and 12 patients proceeded to AVR (median time to AVR 128 days). Of the 136 patients receiving BAV for bridge-to-TAVI/AVR, only 54 patients (39.7%) proceeded to TAVI or AVR within 12 months following BAV, with many patients (60.3%) not proceeding to TAVI due to either death or Heart Team decision that they were unlikely to benefit. Twelve-month mortality was 7.0% among those proceeding to TAVI or AVR.
BAV outcomes to 12 months
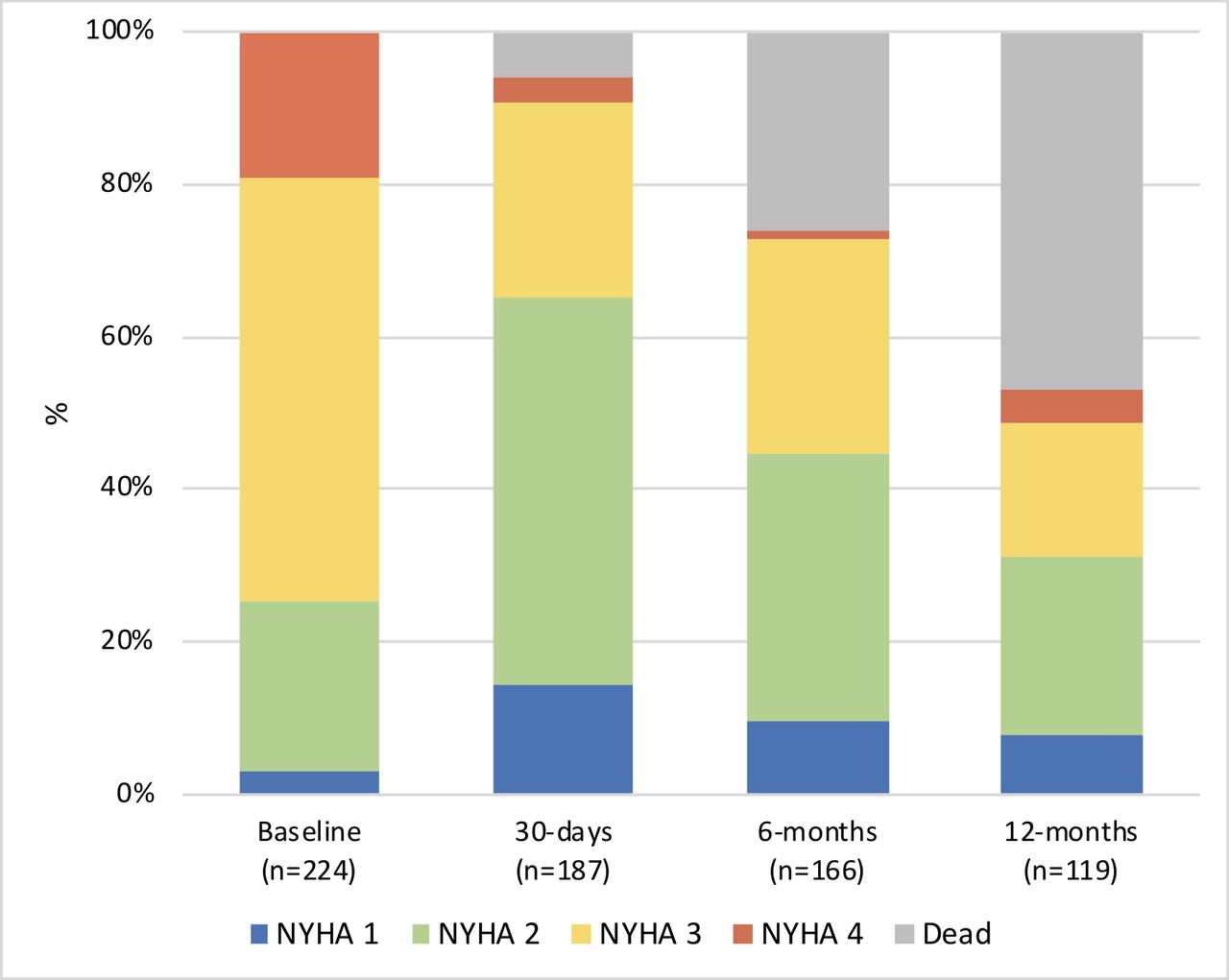
NYHA functional response to BAV is presented in figure 2. Of the cohort, 74.6% were NYHA grade 3 or 4 at baseline, compared with 34.8% at 30 days, 55.4% at 6 months, and 68.9% at 12 months (p<0.001). Multivariate analysis demonstrated NYHA 4 at baseline, NYHA 3 at baseline, body mass index (BMI) ≥30 kg/m2, female gender, and bridge-to-TAVI/AVR as the indication for the BAV, which were all associated with NYHA grade improvement of ≥1 at 30 days post BAV (table 5).

Functional response to BAV – functional response to BAV assessed using NYHA scores to classify symptoms. BAV, balloon aortic valvuloplasty; NYHA, New York Heart Association.
Multivariate predictors of response to BAV
The mean aortic valve area was 0.65±0.2 cm2 at baseline, 0.79±0.3 cm2 at 30 days, 0.73±0.2 cm2 at 6 months and 0.66±0.2 cm2 at 12 months. The mean aortic mean gradient was 46.1±19.0 mm Hg at baseline (pre-BAV), 40.4±0.2 mm Hg at 30 days (p<0.001 compared with baseline), 43.8±15.4 mm Hg at 6 months (p=0.65) and 47.8±24.0 mm Hg at 12 months (p=0.19). The mean LVEF, E/e’ and LVEDD measures were not different at 30 days, 6 months or 12 months following BAV.
LVEF improved by ≥10% in the destination treatment group in 15.6% at 30 days and 7.1% at 6 months, and in the bridge-to-TAVI/AVR group in 15.7% at 30 days and 21.2% at 6 months (table 4). Among patients with LVEF ≤40% at baseline, 24.3% had improvement by ≥10% at 30 days and 47.8% had improvement by ≥10% at 6 months. In multivariate analysis, LVEF ≤40% at baseline was the only variable associated with improvement in LVEF by ≥10% at 6 months (table 5).
Forty-four patients (20.4%) had low-gradient AS, of which 22 had a BAV indication of bridge-to-TAVI/AVR. Of those with available TTE data, 4 of 21 patients (19.1%) demonstrated improvement in LVEF ≥10% at 30 days, whereas 7 of 15 patients (46.7%) demonstrated improvement in LVEF ≥10% at 6 months. BAV was performed in 7 of the 22 bridge-to-TAVI/AVR patients with the intent of assessing for improvement in LVEF, and of these, 2 patients proceeded to TAVI, whereas 1 patient proceeded to AVR following a good response to BAV.
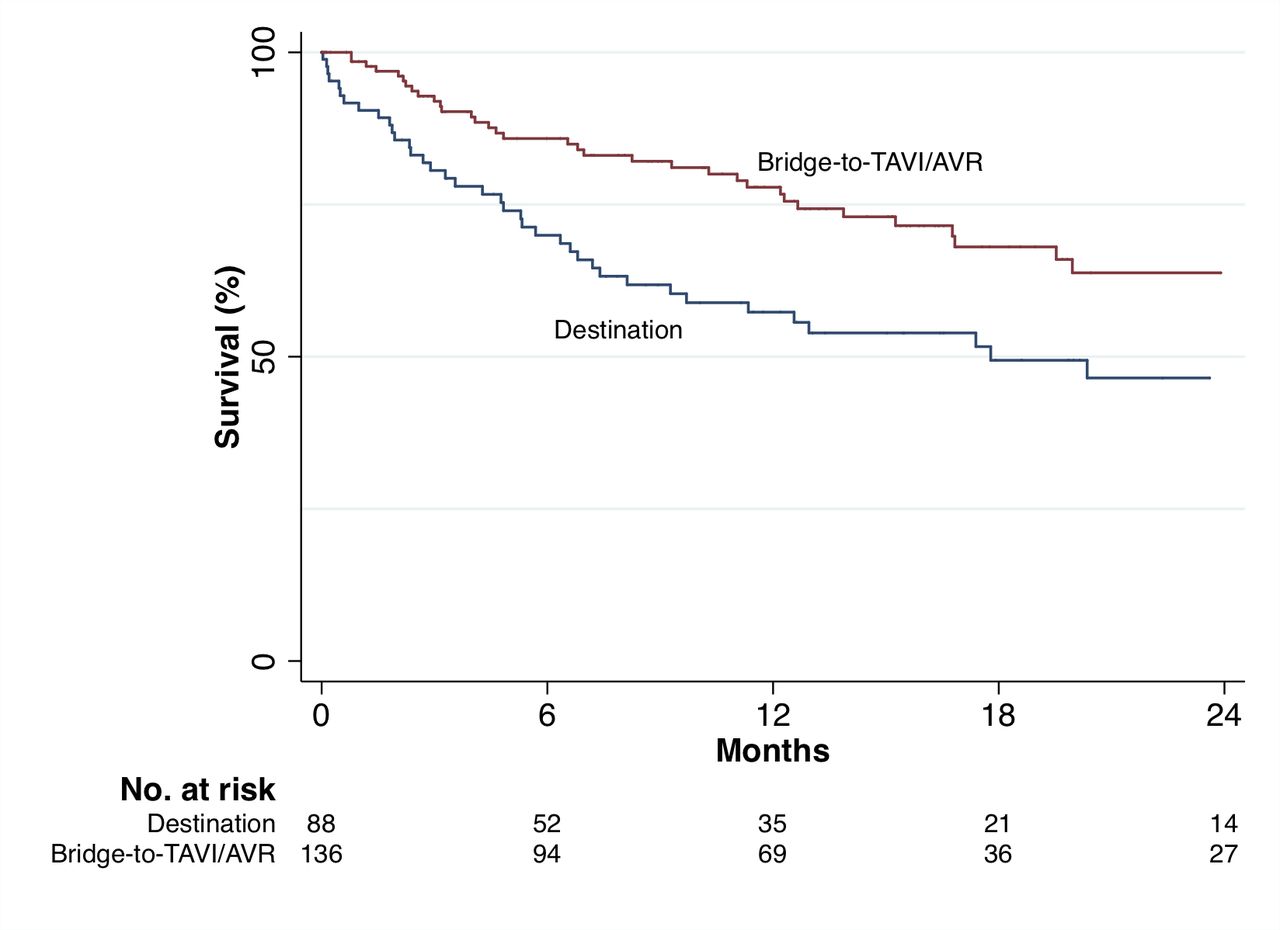
Multivariate analysis identified active malignancy at baseline, smoking history, LVEF ≤30% at baseline, non-elective procedure and destination treatment as the indication, which were all associated with 12-month mortality following BAV (table 5). Kaplan-Meier survival estimates are presented by indication in figure 3, demonstrating a significant difference in survival between destination and bridge-to-TAVI/AVR groups (p<0.01) to 24 months. Degree of reduction in catheter-measured mean pressure gradient immediately post BAV was associated with reduced 12 month mortality in univariate but not multivariate analysis, but was not associated with improvements in NYHA score. At 12 months, 76% had an NYHA score ≥2, consistent with severe symptomatic AS (figure 2).
{kind=link}
{kind=link}
{kind=link}
Kaplan-Meier survival estimates by indication – survival estimates for BAV over a 2-year follow-up. Groups compared using the log-rank test. AVR, aortic valve replacement; BAV, balloon aorticvalvuloplasty; TAVI, transcatheter aortic valve implantation.
Discussion
This study focuses on the current indications, use and outcomes of BAV in the contemporary setting, where TAVI is commonly used. Among our cohort, 57% of procedures were performed as a bridge-to-TAVI/AVR (and is increasing year by year), demonstrating that this is increasingly becoming accepted as an indication for BAV. This is in line with current American College of Cardiology/American Heart Association guidelines stating BAV may be considered as a bridge to AVR or TAVI in patients with severe symptomatic AS (Class 2B; Level of Evidence C).30 31 Of note, in our cohort, BAV was used as a bridge-to-decision in 29% of the cases. Although procedural mortality for BAV is low (<1%) and there is significant symptomatic benefit following BAV, by 12 months there is a recurrence of severe, symptomatic AS in 76% of patients. Thus, definitive therapy such as TAVI or AVR should be offered in the first 6 months following BAV, where appropriate.
Frequently, given the age, frailty and multiple comorbidities of patients with severe aortic stenosis, potential benefits of TAVI or AVR may be uncertain, and with this uncertainty, it may be difficult to justify the procedural risks and costs associated with TAVI/AVR. BAV has utility in this context for two reasons. First, as proposed by previous studies,12–14 patient response to BAV can be used to delineate the contribution of aortic stenosis to patients’ symptoms and functional impairment, relative to other limiting comorbidities. It provides the clinical prediction of likely functional and haemodynamic response to a valve replacement and thus allows better patient selection. This indication accounted for 11% of our cohort. Second, patients with severe aortic stenosis often have complex medical histories that require further evaluation of their comorbidities, prognosis and psychosocial support. BAV creates an opportunity for comprehensive patient assessment to be made. Indeed, only 40% of bridging patients proceeded to TAVI or AVR within 12 months following BAV, lending support to the discriminative power and clinical utility of BAV, as almost half of the patients originally considered for TAVI or AVR were subsequently deemed not suitable for these procedures. In this setting, BAV procedural numbers increased over the final few years of the study, mirroring the increase in TAVI procedural numbers as it becomes more frequently used among patients of lower risk.
Consistent with other studies, another important benefit of BAV is effective symptomatic relief. In our study, we have shown that in 30%–40% of all patients, the functional improvement (judged by the change in NYHA class of ≥1) lasts for 6 months. Although this may seem short lived, it could provide a meaningful improvement in the quality of life in the destination group, whose life expectancy may be severely limited by other comorbidities (eg, active cancer). Our finding also has implications for the bridging group, where waitlists for TAVI remain significant in many jurisdictions. Finally, recent data suggest that emergency TAVI has high rates of 30-day mortality, and bridging BAV in this setting may provide an opportunity to medically stabilise the patient with further assessment of suitability for TAVI once stabilised.24
Immediate postprocedural haemodynamic changes were comparable with previous studies (mean gradient reduction 13.2±13.5 mm Hg in the PARTNER Cohort B study vs 15.9±9.5 mm Hg in our study).26 Among our cohort, we describe low rates of major procedural complications and procedural mortality (0.5%) also consistent with prior data,4 16 19–21 and highlighting acceptable safety in this high-risk cohort. Twelve-month mortality was 50% among the destination treatment group, which is comparable with the 47% reported among the PARTNER Cohort B study for patients undergoing initial BAV.26 Twelve-month mortality was 26% in the bridge-to-TAVI/AVR group, which is also similar to previously reported rates.16 19 Active malignancy at baseline, smoking history, LVEF ≤30% at baseline and destination treatment as the indication for BAV were all associated with 12-month mortality in multivariate analysis, and therefore, careful consideration as to the likely benefit of a palliative BAV procedure in these patient groups should be made given their overall worsened prognosis.
Although numerous studies have reported BAV procedural outcomes,4–6 16 17 19 21–23 32–34 only one recent smaller study has assessed functional response following BAV,20 and none have assessed multivariate predictors of improvement in functional response post procedure. NYHA 4 at baseline, NYHA 3 at baseline, BMI ≥30 kg/m2, female gender and bridge-to-TAVI/AVR as the indication for BAV were all associated with improvement in NYHA score at 30 days in our cohort. Our data highlight the benefit of using BAV as a bridge-to-TAVI/AVR, especially among more symptomatic patients (NYHA 3 and 4), and those of the female gender. The improved functional response and mortality benefit among obese patients has not previously been described but is consistent with the notion of the ‘obesity paradox’ described in TAVI and percutaneous coronary intervention (PCI) outcomes, whereby obesity is associated with improved post-TAVI and post-PCI survival.35 36 However, this observation may be at least partially driven by frail patients having lower BMI, which is not captured by our study.
Determining patients who may show improvement in LV function following BAV or TAVI/AVR is clinically important to allow the selection of patients that may maximally benefit from the procedure. Among patients with low-gradient AS, we found that 47% had improved LVEF ≥10% at 6 months. In our study, the only factor associated with improvement in LVEF by ≥10% at 6 months was LVEF ≤40% at baseline in our study, suggesting a higher gain in patients with more advanced disease. This may support the role of using the improvement of LV function post BAV to identify patients that may benefit most from TAVI/AVR.
Limitations of this study include its retrospective cohort design at a single metropolitan centre, which may be susceptible to selection bias and reduced generalisability to the broader Australian and international populations. As with any retrospective study, there is the potential for unmeasured confounders and findings need to be interpreted as observational. The decision regarding whether a patient underwent BAV as a destination treatment or as a bridge-to-TAVI/AVR is partially explained by the difference in STS score between groups, but generally, baseline characteristics were surprisingly similar between the groups. Frailty and cognitive function play an important role in the selection of patients for BAV and TAVI and could not be captured by this study due to the retrospective design. These factors may have assisted in explaining the difference in patient selection and outcome between the destination and bridge-to-TAVI/AVR groups.
Conclusions
BAV remains a useful clinical procedure with relatively low rates of procedural complications and mortality and has become increasingly utilised since the advent of TAVI. Contemporary indications include destination therapy, where it provides effective symptomatic relief over 6–12 months, or as a bridge-to-TAVI/AVR where it can be used as a stratifying tool for clinical decision making on valve replacement, as a measure to address issues that pose temporary contraindication to TAVI/AVR and to offer symptomatic improvement to patients who have prolonged waiting time for the TAVI/AVR. Highly symptomatic patients (NYHA 3 or 4), females and obese patients may be more likely to benefit symptomatically following BAV.
References
Footnotes
Contributors All authors contributed to conception and design of the study. LD: performed the data collection, statistical analysis and initial manuscript drafting. LD and SD: responsible for the overall content. All authors contributed to conception and design of the study; contributed to interpretation of results and critical revision of the manuscript.
Funding Professor Duffy's work is funded by National Health and Medical Research Council grants.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request. Data are available upon reasonable request.