Article Text

Abstract
Atrial fibrillation (AF) is the most common arrhythmia encountered in clinical practice, with a prevalence that increases alongside the ageing population worldwide. The management of AF involves restoration of sinus rhythm through antiarrhythmic drug therapy. Yet, these medications have only modest efficacy in achieving long-term success, have not shown to result in a mortality benefit, are frequently not tolerated and have associated adverse side effects. Therefore, catheter ablation has become a valuable treatment approach for AF and even a viable first-line strategy in select cases. Traditionally, the combination of radiofrequency energy and a three-dimensional electroanatomical mapping system has been used to guide catheter ablation for AF. However, single-procedural efficacy and long-term outcomes still remain suboptimal for many patients, particularly those with persistent or long-standing AF. Recent advances in ablation technology and strategy, therefore, provide new procedural approaches for catheter-based treatment with the aim of overcoming current challenges in procedural duration and overall success. The aim of this paper was to provide an updated review of the current practices and techniques relating to ablation for AF and to compare the use of these strategies for paroxysmal and persistent AF.
- atrial fibrillation
- atrial flutter
- arrhythmias
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Identifying the optimal strategy for the treatment of atrial fibrillation (AF) continues to be an evolving challenge for clinicians as the initiation and maintenance of AF occur as a result of complex interactions between arrhythmia triggers, changes in the atrial substrate and alterations in the autonomic nervous system activity.1 For patients undergoing catheter ablation, the optimal set of ablation lesions depend primarily on the distribution of these factors and the clinical type of AF.2
Pulmonary vein isolation (PVI) is the recommended treatment for drug refractory symptomatic AF or in patients who are intolerant or unwilling to take antiarrhythmic drug therapy.3 However, the success of catheter ablation is limited and depends largely on patient characteristics.4 Indeed, while PVI can be achieved in a significant proportion of patients with paroxysmal AF with a 60%–80% clinical success rate,5 results remain suboptimal in patients with persistent and long-standing persistent AF who are often refractory to catheter ablation or require multiple repeat procedures. In patients with paroxysmal AF, ablation successfully targets triggers that are predominantly located in the pulmonary veins (PVs) and less commonly non-PV triggers. Accordingly, circumferential PVI, with confirmation of both entrance and exit block, remains the cornerstone of this procedure.
Conversely, in patients with persistent AF, the atrial substrate is complicated by atrial wavelets, multiple macro re-entry circuits, and localised sources,6 7 leading to suboptimal procedural outcomes.8 The most effective ablation strategy in patients with persistent and long-standing persistent AF is currently unknown despite the fact that several techniques have been attempted with minimal or no success. A summary of triggers responsible for the initiation and propagation of AF is displayed in figure 1.
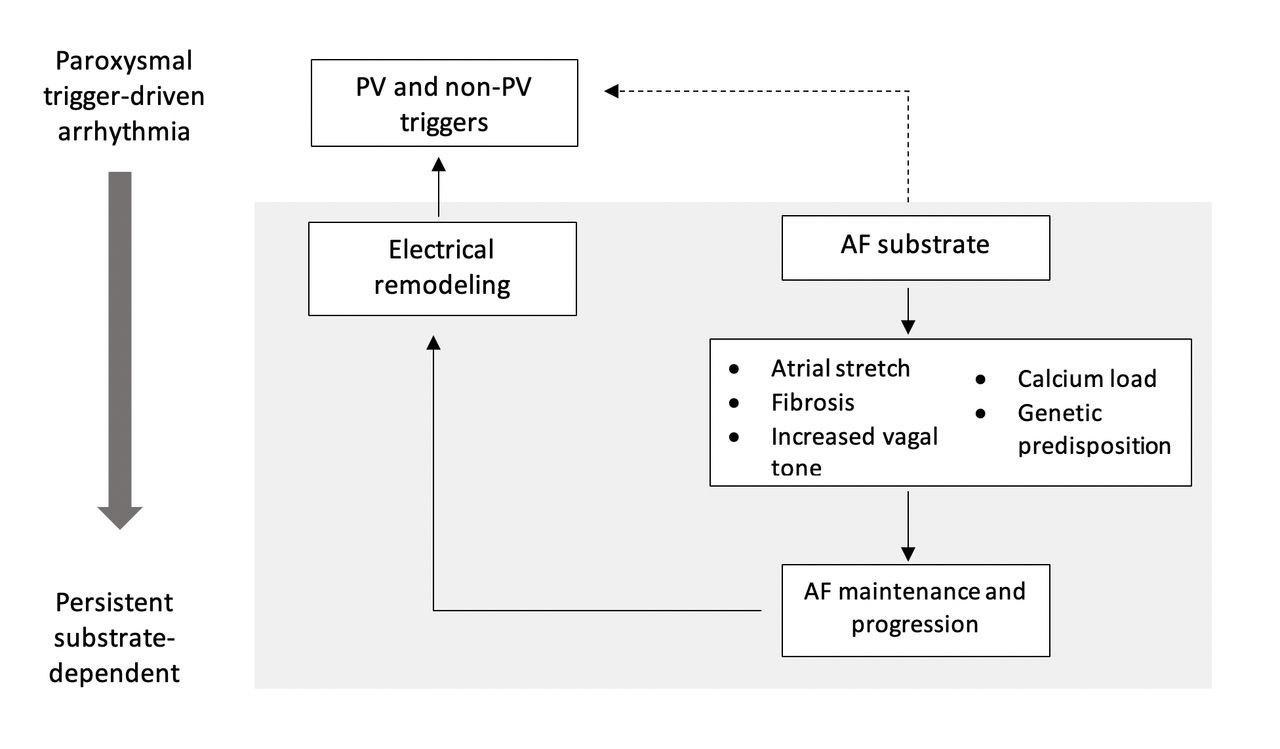
Distribution of triggers responsible for the initiation of AF. AF, atrial fibrillation; PV, pulmonary vein.
In this review, we will provide an overview of evolving techniques for the treatment of catheter ablation, while focusing on the more recent advances.
Catheter technology and energy sources
To date, a variety of energy modalities have been employed for the catheter ablation of AF including radiofrequency (RF), cryoablation (CB), microwave, high-intensity focused ultrasound and electroporation. Notably, the two most commonly used sources in clinical practice are RF and CB.
RF energy is generated at a frequency of 500–1000 KHz and transmitted between the catheter tip and an electrode patch positioned on the skin. The maximum amount of resistive energy occurs within approximately 2 mm of the catheter tip and is either transmitted to the endocardial surface of the heart or the blood. The majority of lesion formation occurs as a result of conductive heat, which is inversely proportional to the distance from the tip of the electrode. CB on the other hand involves three phases of tissue damage. The first occurs during delivery of CB and is known as the freezing–thawing phase. As the temperature drops below −15°C, microscopic extracellular ice formation occurs, followed by intracellular ice formation when the temperature drops below −40°C and results in localised tissue damage. As thawing occurs, there is fusion of the ice crystals with mircothrombi and platelet aggregation. Subsequently, the hemorrhagic-inflammatory phase occurs with localised tissue inflammation and oedema and finally, the replacement-fibrosis phase takes place and a fibrotic scar develops.
When compared with RF energy, patients randomised to either CB or RF groups had similar success rates and safety outcomes at 1.5 years follow-up. The results of the large multicentre Cryobaloon or Radiofrequency Ablation for Paroxysmal Atrial Fibrillation (FIRE AND ICE) trial,9 therefore, validate the use of CB as an alternative to conventional RF ablation for the treatment of paroxysmal AF. While the results of this trial may have been limited by the combined use of both first-generation non-contact force and second-generation contact force (CF) catheters, freedom from AF was still observed in 64.1% of subjects undergoing RF ablation and 65.4% of those undergoing CB. Additional 30 months freedom from AF data supported the non-inferiority of CB to RF ablation. It is important to note that cryoballoon ablation has been associated with significantly higher radiation doses due to the need for PV angiography to confirm complete PV occlusion and ensure optimal tissue freezing.10 Nonetheless, more than 35 000 CB-based ablations have been performed worldwide to date.11
More recently high-power short-duration (HPSD) RF has been studied to assess if this is more effective and safer than conventional power settings. It has been postulated that HPSD lesions may minimise the impact of catheter stability as the lesion is delivered over a shorter period of time which may increase the consistency of the lesions with less localised oedema. By using the method there is more immediate localised tissue heating and with less conductive heat which may result in collateral damage. Ablation at 90 W delivered over 4 s per lesion has been shown to be effective (reduced linear gaps and non-transmural injury as well as increased lesion to lesion consistency) and safe in a preclinical model and superior to 20 W delivered over 20 s in the atrium.12
HPSD lesion diameters have been shown to be significantly larger and deeper when compared with standard settings in an in silico simulation study.13
Ablation catheters
Current catheter technology can be divided into a single tip irrigated catheter (generally 3.5–4.0 mm) which may or may not use CF or a single-shot device which generally has multiple electrodes and is positioned within the PV antra in order to deliver energy over a region of tissue.
Lesion creation depends on catheter-to-tissue contact, the quality of which is conventionally assessed via impedance drop during RF application. However, these parameters may not provide a full depiction of actual electrode–tissue contact14 and creating continuous effective circumferential lesions remains a clinical challenge. More recently, the adoption of CF-sensing catheters enables rapid and accurate confirmation of the completeness of PV antrum isolation, leading to improved outcomes and fewer repeat procedures.15–17 This is achieved through direct assessment of catheter–myocardial contact and directionality during the delivery of RF ablation. Catheter–tissue CF can be measured at the catheter tip either with fibreoptic or magnetic sensors which are able to measure the force between the distal catheter electrode and the tissue or a localised impedance calculation algorithm which does not provide CF but indicates wall contact versus no wall contact. The local impedance drop has a more accurate correlation with lesion size than global impedance drop.18
During a procedure, certain CF parameters can be measured in real time. This includes amplitude and orientation of real-time CF (recorded every 100 ms), average force (Fav in gram-force, g), force time integral index measured as the product of real-time force and ablation time and lesion index, a proprietary index combining CF, RF application duration and RF current.
The effectiveness of a CF-sensing catheter has previously been investigated in ex vivo models and in vivo experimental studies. While these results were promising, there is no consensus that the use of CF catheters imparts better efficacy for PVI in clinical applications, particularly with respect to reducing the rate of complications. Nonetheless, real-time CF-sensing RF catheter ablation utilising CF of 10–20 g has been previously correlated with significantly reduced rates of AF recurrence in paroxysmal AF when compared with PVI without CF monitoring.19 Likewise, in patients with persistent AF, CF-guided ablation has been related to significantly reduced AF recurrence rates during 1-year follow-up as compared with non-CF-guided ablation, 27.6% vs 46.4%, respectively.20 To date, countless studies still fail to demonstrate clear differences in ablation outcomes or procedural safety.21 22 First-pass PVI, however, does appear to be more likely with CF technology and occurrences of acute PV reconnection may also be diminished.23 24 This is because continuous catheter–tissue CF can be measured, which not only ensures accurate placement of the catheter at the onset of the procedure, but also enables further detection of catheter dislodging or shifting in real time. Future studies should aim to establish the optimal RF power and lesion duration required of CF-sensing catheters to ensure adequate lesion formation, while avoiding collateral tissue injury.
Although several single-shot devices have been used in the past with differing effects and complications, there are a number of single-shot devices currently being developed which are yet to be released on the clinical market.
Techniques for the management of paroxysmal AF
Isolation of PV triggers
In patients with paroxysmal AF, catheter ablation is concentrated on eliminating AF triggers, which originate within the PVs in 80%–94% of patients with AF.25 Evaluation of PV electrical activity and identification of residual conduction gaps are performed using a circular multipolar catheter with a focus on PV antral electrical activity. Although the use of these catheters has previously been shown to result in lower rates of AF recurrence when compared with an RF catheter alone,26 the orientation of the PV to the left atrium (LA) is complex and may result in additional RF energy delivery beyond that which is required. A novel mapping catheter which allows for bipole recording both along and across the splines (HD Grid Mapping Catheter Sensor Enabled, Abbott Technologies, Mineapolis, USA), has been shown to enhance the accuracy of substrate mapping by providing simultaneous assessments of conduction voltage, activation and directionality. High-resolution mapping using the HD Grid has recently demonstrated efficacy in the assessment of bidirectional block and signal differentiation in first-time and redo PVI.27 However, while acute electrical disconnection between the PV and LA is an established endpoint and may indicate isolation after lesion delivery, there are cases where PV connection is concealed by local oedema.28 Three-dimensional (3D) mapping systems are widely utilised to support the procedure and can confirm the completeness of PVI by creating a detailed voltage map. In general, wide antral circumferential ablation is performed in order to achieve PVI.
Non-PV trigger elimination
The identification and elimination of non-PV triggers are important, particularly in repeat procedures, where PVI continues to be present. The majority of these non-PV triggers are located in the superior vena cava (SVC), coronary sinus and crista terminalis or at the posterior LA wall as well as the left atrial appendage (LAA).29 Specifically, isolation of the SVC has been evaluated as an adjunct to PVI. In one study of 320 consecutive patients with either paroxysmal or persistent AF, 90% of those with paroxysmal AF undergoing SVC isolation were free of atrial tachycardia (AT) compared with 77% of those without isolation.30 However, these results are yet to be replicated in other randomised populations.
In patients without spontaneously firing non-PV triggers, a high-dose of isoproterenol (ie, infusion of 20–30 µg/min or bolus infusion of 10–20 µg) is commonly used to provoke them. Cardioversion of AF during low-dose isoproterenol infusion is also used in many cases. However, the protocol for provoking and subsequently localising the non-PV triggers is yet to be standardised. For patients with paroxysmal AF, there is little evidence to support the benefit of routine ablation beyond PVI in the absence of documented extrapulmonary triggers or coexisting atrial tachyarrhythmias in patients undergoing an index ablation.
Management of persistent AF
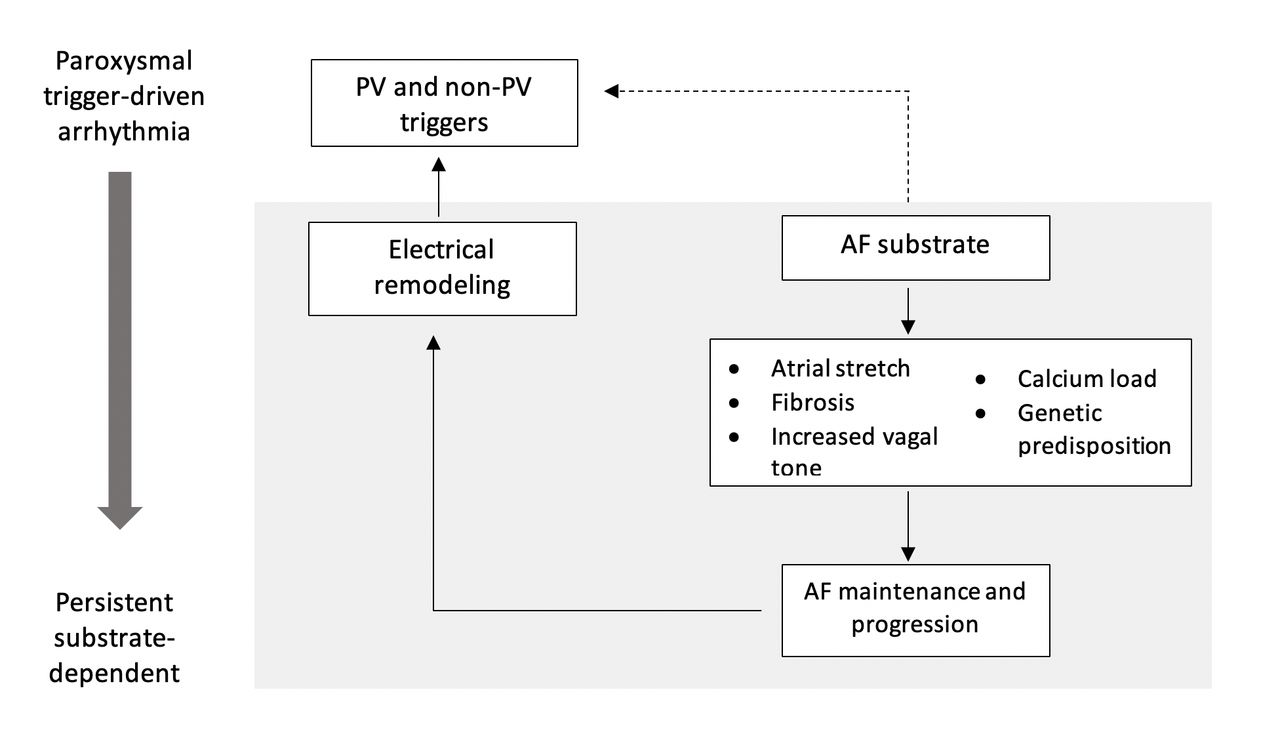
The effectiveness of PVI in patients with persistent and long-standing persistent AF has been reported as low as 21%.31 The basis for these results is that the sites of AF initiation and maintenance may be diffuse in all four PVs and their antrum and conduction recurrence in only one PV can lead to AF recurrence.32 The pathogenesis of persistent AF is complex and cannot be characterised by the same markers of paroxysmal AF (anisotropic conduction, autonomic innervation of the heart, embryogenesis of thoracic veins and interspersion of inhomogeneous tissue). The purported mechanisms of persistent AF are summarised in figure 2.

Potential mechanisms in the pathophysiology of persistent AF. AF, atrial fibrillation.
The main techniques which have been studied for the management of persistent AF include the elimination of complex fractionated atrial electrograms (CFAEs), linear lesions, rotor ablation and scar homogenisation. This has raised questions of whether trigger-based ablation strategies through PVI should be performed alone or in combination with substrate-based strategies, such as CFAEs. Yet, as recently reported, the use of additional ablation lesion sets such as CFAEs and linear lesions fail to improve ablation success.
CFAE ablation
Defragmentation of the LA is based on the elimination of all multicomponent electrograms of short cycle length, such as CFAEs. CFAEs are most often defined as continuous atrial activity, complex fractionated potentials or low-voltage electrograms with a short cycle length of <120 ms over a 10 s period. Therefore, their ablation usually leads to prolongation of AF cycle length, resulting in conversion into AT or sinus rhythm.33 However, the endpoints of CFAE ablation are not clearly defined, resulting in low-intraprocedural reproducibility of CFAE elimination and limited clinical success rates.34
Previous studies have demonstrated that CFAE originate along the regions of slow conduction, functional block and pivot points.35 Non-PV ectopies have also been found in similar locations as the CFAEs, with 25% of CFAEs in the LA and 57% of CFAEs in the right atrium related to non-PV triggers after PVI.36 These abnormal conduction patterns then serve as potential targets for ablation. Data suggest that CFAE ablation beyond PVI may not necessarily enhance single procedure efficacy in ablating persistent or long-standing persistent AF. In the RASTA Study, the addition of LA CFAE ablation with PVI was less efficacious to both PVI plus ablation of non-PV triggers using a standard approach as well as the standard protocol plus empirial ablation of common non-PV AF trigger sites (fossa ovalis, SVC and mitral annulus).37
Despite multiple investigations, the optimal treatment strategy for persistent AF remains unknown and the addition of substrate-based ablation strategies has failed to demonstrate conclusive benefit in subsequent trials. Results of the CHASE-AF Study38 and the recently published Alster-Lost-AF Study have demonstrated no clinical benefit of a combined approach of PVI plus additional substrate modification through CFAE ablation and linear ablation over stand-alone PVI.39 Of 118 patients with persistent or long-standing persistent AF who were assigned PVI alone or combined PVI and substrate modification, there was no statistically significant difference observed in recurrence rates (46% and 43%, respectively). The multicentre, randomised STAR-AF II trial produced similar results when the recurrence rates of AF or AT at 18 months follow-up were compared between stand-alone PVI and PVI with additional ablation techniques.34
Linear lesions
The roof and mitral isthmus of the LA are the most commonly targeted sites for substrate modification using linear ablation (figure 3). However, it is difficult to achieve a durable and complete bidirectional conduction block across these lines. In particular, mitral isthmus ablation is difficult and may warrant entry into the coronary sinus to achieve complete block. This has been correlated with a high incidence of mitral isthmus reconduction,40 which is significantly associated with the development of mitral isthmus-dependent flutter. In a retrospective cohort of 50 patients who had perimitral flutters during the index procedure of follow-up,41 prior mitral isthmus ablation was associated with a higher risk of developing perimitral flutter despite achieving bidirectional block acutely.

{kind=link}
{kind=link}
{kind=link}
Linear ablation at mitral isthmus and roof line. MI, mitral isthmus; R, roof.
Previous studies have demonstrated that up to 90% of ATs after AF ablation are re-entrant42 and consequently, repeated procedures are often required to increase the success rate above 50%. However, even after multiple procedures, the incidence of atypical flutter or AT has been reported as high as 30%.43 Therefore, while linear lesions may contribute to eliminating AF at initial ablation, incomplete block lines may promote proarrhythmic AT and re-entry.
Rotor ablation
AF has been postulated to be sustained by electrical rotors and focal impulses and ablation of such sources has been associated with improved procedural outcomes compared with conventional ablation alone.44 This is of particular interest in patients with long-standing persistent AF, where the LAA may be a common source of AF rotors or focal drivers. Rotors are enabled by the ionic and conduction defects at the cellular level and intermittent areas of fibrosis lead to the stabilisation and propagation of rotors.45 Certain techniques, such as optical mapping, assist in uncovering the location of rotors and therefore, are amenable for ablation. Yet, there is no consensus on ablation of rotors in patients with AF due to inconsistencies in determining their contributory role in the maintenance of human AF. Most recently, focal impulse and rotor modulation (FIRM)-guided ablation demonstrated low long-term efficacy when performed in 43 patients as part of a single-centre observational study.46 FIRM-guided ablation led to redo PVI in 72% of patients, of which 21% were free from AF at 16±10.7 months follow-up. Furthermore, the randomised BELIEF trial reported routine LAA isolation to be safe with no cases of embolic events postablation, although, an impaired contractile function of the LAA was identified in more than 50% of patients using transoesophageal echocardiography.47
The presence of rotors has been widely disputed given the available technologies used to map these small regions of rotational activity. Currently, the identification of rotors depends on utilising either basket catheters deployed within the atrium or multielectrode vests worn on the outside of the body to map AF. Both these mapping techniques lack detailed resolution and as result, identification of rotors can be challenging and heavily dependent on postprocessing of the raw data. The development of omnipolar technology may overcome these limitations by providing instantaneous visual depictions of local electrogram amplitude, activation direction and conduction velocity at any given point. Evidence supporting omnipolar mapping to conventional bipolar mapping has been previously described in vivo,48 49 but further investigation is warranted to validate this concept in human subjects.
Scar homogenisation
The pathophysiological importance of epicardial adipose tissue, atrial fibrosis and arrhythmogenic foci has been implicated in previous studies. The development and progression of atrial fibrosis are the primary modulator of structural remodelling in AF. Fibrosis promotes AF by interrupting fibre bundle continuity and causing disturbances in local conduction.50 Catheter ablation based on atrial scar sites as arrhythmic substrate has, therefore, emerged as a recent treatment approach for persistent AF. It can be detected from cardiac MRI with delayed enhancement or 3D mapping with bipolar low-voltage electrogram. Previous studies have demonstrated that atrial fibrosis, estimated by delayed-enhancement MRI, is independently associated with the likelihood of AF recurrence.50 51 With evolving data on the association between atrial fibrosis and AF progression, ablation strategies have been developed to eliminate low-voltage zones that may indicate scar, otherwise known as scar homogenisation. Improved AF outcomes may be achievable through patient-specific substrate modification based on targeted ablation of atrial fibrosis. Nonetheless, voltage map-guided ablation is yet to gain widespread adoption into routine practice and further investigation is required to establish its long-term safety.
Conclusion
Despite the advancement of ablation strategies over the past two decades, long-term success rates and single-procedural efficacy remain suboptimal for many patients. These outcomes are particularly evident in patients with persistent or long-standing AF, where the results are clearly inferior to those for paroxysmal AF. Furthermore, the overall stroke and mortality benefits conferred on patients undergoing catheter ablation remain inconclusive. Ongoing clinical trials have, therefore, been designed to better address this. The Early treatment of Atrial Fibrillation for Stroke prevention Trial (EAST-AFNET 4) has enrolled over 2500 and will evaluate whether an early, comprehensive, rhythm control strategy using anti-arrhythmic drugs (AADs) or catheter ablation prevents adverse cardiovascular outcomes compared with standard care. Other recently conducted trials such as CASTLE-AF assess these outcomes in specific patient populations, including those with heart failure and left ventricular ejection fraction below 35%. With the development of ablation techniques, our understanding of AF mechanisms as well as the underlying factors influencing the incidence of perioperative complications, and overall success rates, are expected to improve. Thus, ongoing research may offer new treatment avenues for AF, while identifying novel therapeutic mechanisms in discrete populations of difficult-to-treat arrhythmia.
References
Footnotes
Twitter @kathrynhong
Contributors All authors contributed equally to this work.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement No data are available. Review article.