Article Text

Abstract
Introduction Stent underexpansion is a predictor of in-stent-restenosis and stent thrombosis. Semi-compliant balloons (SCBs) are generally used for lesion preparation. It remains unknown whether routine predilatation using non-compliant balloons (NCBs) improves stent expansion in ordinary coronary lesions.
Methods The PREdilatation by high-pressure NC balloon catheter for better vessel preparation and Optimal lesion preparation with non-compliant balloons for the implantation of bioresorbable vascular scaffolds studies randomised patients presenting with stable coronary artery disease or non-ST-elevation myocardial infarction requiring stent implantation to lesion preparation using NCBs versus SCBs. Stent expansion index (SEI-minimal luminal area/mean luminal area on optical coherence tomography) and periprocedural complications were compared.
Results We enrolled 104 patients: 53 patients (54 lesions) vs 51 patients (56 lesions) to the NCB and SCB groups, respectively. Predilatation pressure was higher in the NCB group (24±7 atmospheres (atm) vs 14±3 atm, p<0.0001). Postdilatation using NCBs was performed in 41 (76%) lesions vs 46 (82%) lesions pretreated with NCBs versus SCBs (p=0.57). Similar pressures were used for postdilatation with NCB in both groups (23±8 atm vs 23±9 atm, p=0.65). SEI after stent implantation was 0.88±0.13 in the NCB vs 0.85±0.14 in the SCB group (p=0.18). After postdilatation, SEI increased to 0.94±0.13 in the NCB group vs 0.88±0.13 in the SCB group (p=0.02). No relevant complications occurred.
Conclusions In simple coronary lesions, predilatation/postdilatation with NCBs at high pressures appears to result in better scaffold and stent expansion. Using SCBs only for predilatation might lead to inadequate stent expansion and postdilatation with NCBs might only partially correct this. Predilatation and postdilatation using NCBs at high pressure is safe.
Trial registration number ClinicalTrials.gov no. NCT03518645.
- Angioplasty
- Percutaneous coronary intervention
- Stent
- Scaffold
- Lesion preparation
- Optical coherence tomography
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- Angioplasty
- Percutaneous coronary intervention
- Stent
- Scaffold
- Lesion preparation
- Optical coherence tomography
Key questions
What is already known about this subject?
Stent underexpansion is a key contributor leading to adverse long-term events including in-stent-restenosis and stent thrombosis.
Most interventional cardiologists use semi-compliant balloons (SCBs) for lesion preparation, which might result in inappropriate lesion preparation and ultimately inadequate stent expansion.
What does this study add?
We assessed if routine predilatation using non-compliant balloons (NCBs) compared with SCBs improves final stent expansion in ordinary coronary lesions.
We found that adequate predilatation and postdilatation with NCBs at high pressures results in better stent expansion.
It is noteworthy that predilatation and postdilatation using NCBs at high pressure appears safe.
How might this impact on clinical practice?
The concept of routine use of SCB for lesion preparation in ordinary lesions requires a critical appraisal.
In clinical routine, interventionalists should rather aim for predilatation and postdilatation with NCBs at adequate pressures in order to achieve optimal stent implantation results, specifically stent expansion.
Introduction
Stent underexpansion has been identified as key contributor leading to adverse long-term events including in-stent-restenosis (ISR) and stent thrombosis (ST).1–3
Traditionally, semi-compliant balloons (SCB) have been used for lesion preparation before stent implantation. An earlier observational study evaluating the utility of scoring balloons demonstrated better stent expansion in calcified and fibrotic lesions.4 Furthermore, a recent small, randomised study demonstrated better stent expansion with scoring balloons compared with SCBs.5
The use of non-compliant balloons (NCBs) for lesion preparation has become clinical routine at many sites. NCBs have a much more predictable diameter during inflation at higher pressures and the so-called ‘dog-boning’ phenomenon causing vessel dissections and perforations can be avoided. There is a lack of evidence if routine use of NCBs for lesion preparation improves stent expansion. In fact, the concept of high-pressure predilatation and postdilatation, meaning usage of inflation pressures of ≥20 atmospheres (atm), has only been propagated on the basis of case reports and case series.6–8
We assessed whether the use of NCBs at high pressure versus use of SCBs for lesion preparation leads to better stent expansion and is safe for percutaneous coronary interventions (PCI) in simple coronary lesions.
Methods
We present the pooled data from two randomised pilot PCI studies with identical design comparing two different NCBs from the same manufacturer with standard SCBs.
The PREdilatation by high-pressure NC balloon catheter for better vessel preparation (Pre-NC) study was conducted between January 2014 and December 2016. The study population consisted of patients presenting with stable coronary artery disease (CAD) or non-ST-elevation myocardial infarction (NSTEMI) and requiring PCI with a metallic stent or bioresorbable vascular scaffold (BVS) implantation to a de novo lesion. The Pre-NC study was performed at the Heart Centre Lucerne (Switzerland) and at the University Medical Centre, Utrecht (The Netherlands).
The Optimal lesion preparation with non-compliant balloons for the implantation of bioresorbable vascular scaffolds (OPRENBIS), which was conducted between March 2015 and March 2018, included patients with stable CAD and NSTEMI in whom the implantation of BVS was planned. The patients were randomised to the OPRENBIS study was performed at the Heart Centre Lucerne (Switzerland).
Both studies were investigator initiated. Swiss Interventional Systems (SIS) Medical (Frauenfeld, Switzerland) provided unrestricted research grants for both studies (funding for core-lab analyses). The studies and their databases were monitored and coordinated by the Krakow Cardiovascular Research Institute (KCRI, Krakow, Poland). All patients provided written informed consent to participate.
Trial designs and devices
The patients were randomised by an envelope-based system. All angiograms, optical coherence tomography (OCT) recordings and clinical events were analysed in a blinded fashion by the core laboratory (KCRI). The Pre-NC study randomised patients undergoing PCI with third-generation drug-eluting metallic stents (DES), preferentially Xience everolimus-eluting stents (DES) (Abbott Cardiovascular, Santa Clara, California, USA), or the Absorb everolimus-eluting BVS (Abbott Cardiovascular, Santa Clara, California, USA) in a 1:1 fashion to predilatation using SCBs versus high-pressure predilatation (≥20 atm) with NCBs. The OPRENBIS study’s design was identical to the Pre-NC study. But for lesion treatment, we used only the Absorb BVS.
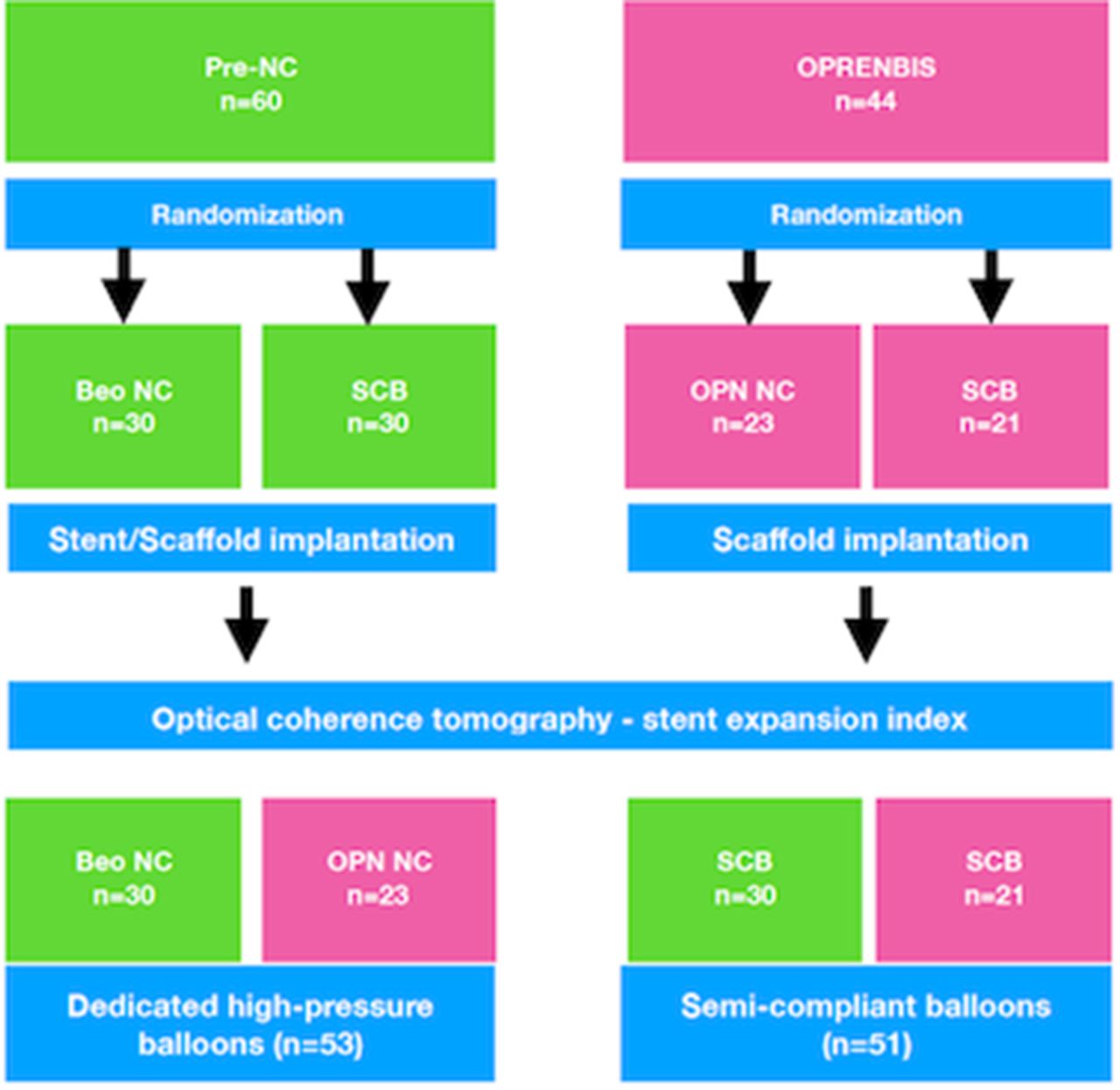
Patients allocated to the SCB predilatation arm underwent lesion preparation with a commercially available SCB at the interventionalist’s discretion. In the NCB groups, Beo NC or OPN NC (SIS Medical, Frauenfeld, Switzerland) were used. Lesions with visible thrombus on angiogram, chronic total occlusions or bifurcation lesions were excluded. By protocol, it was recommended to use inflation pressure of ≥20 atm with those two NCB devices. Of note, the Beo NC has a rated-burst pressure of 24 atm and the OPN NC has a rated burst pressure of 35 atm. After stent/scaffold implantation, OCT of the treated lesion was performed. Postdilatation was recommended in case of evidence for relevant stent under-expansion or malapposition. If performed, it was mandatory to obtain a final OCT. The studies’ flow diagram is illustrated in figure 1.

Study flow chart of the Pre-NC and OPRENBIS trials. NC, non-compliant; SCB, semi-compliant balloon.
For antithrombotic treatment, we ensured that all patients were pretreated with aspirin (eg, 100 mg daily dose prior to the procedure) and received clopidogrel 600 mg (in stable CAD) or ticagrelor 180 mg (or in selected cases prasugrel 60 mg) (in case of NSTEMI presentation). Unfractionated heparin 70 units/kg body weight was administered intravenously at the beginning of PCI. All patients were advised to take dual antiplatelet therapy for 12 months after study enrolment.
Analysis of coronary angiography
Baseline coronary target lesion characteristics and procedure results were evaluated off-line using a dedicated software package (CAAS V.5.11, Pie Medical Imaging, The Netherlands). The analyses generally comprised three main steps: (1) preprocedural (baseline) qualitative evaluation of target lesion; (2) qualitative evaluation of target lesion after last predilatation and (3) qualitative assessment after stenting or after post-dilatation, if performed.
The following parameters were assessed at baseline for target lesion: presence and severity of calcification, American College of Cardiology/American Heart Association (AHA) lesion severity, lesion length, reference vessel diameter, minimal luminal diameter, percentage of diameter stenosis. Calcification was defined as readily apparent densities noted within the apparent vascular wall at the stenosis and separated from the blood-filled lumen by the interceding radiolucent atheroma tissue and endothelial lining. Categories of calcification involved: none, moderate (densities noted only during the cardiac cycle prior to contrast injection) and severe (radio-opacities noted without cardiac motion prior to contrast injection generally involving both sides of the arterial wall).
Of note, evaluation of target lesion after predilatation, stenting/scaffold-deployment and postdilatation also considered assessment of any PCI-related local complications: presence of dissections, side branch closure, distal embolisation, spasm and thrombus.
Optical coherence tomography
All OCT pullbacks were also analysed off-line with dedicated software Ilumien Optis, Offline Review Workstation (St. Jude Medical, USA). The analyses consisted of two main steps: (1) qualitative and quantitative evaluation of region of interest (ROI) and references at after-stenting pullback; (2) qualitative and quantitative evaluation of ROI and references at postdilatation pullback. ROI was defined as the segment with implanted stent/scaffold. Proximal and distal references were defined as the 5 mm segment located proximally/distally to the stent/scaffold. In-stent area was defined as interpolated contour connecting the endoluminal edge of the reflective border, in case of metallic stents, or the abluminal side of black strut cores, in case of bioresorbable vascular scaffold. Lumen area was automatically detected and contoured by the dedicated software and manually corrected if necessary by the analyst. In-stent area contour was delineated in 1 mm interval within the ROI. Each pullback was reviewed for the presence of edge dissections, plaque protrusions, thrombus and incomplete stent apposition after the procedure.
End points and sample size justification
For the current analyses, our primary end point of interest was stent expansion index (SEI), which was calculated based on OCT analysis and defined as the minimum stent/scaffold area divided by average reference lumen area (distal reference area+proximal reference area/2)).9
Procedural complications were systematically evaluated by using angiography and OCT. Clinical end points included new or peri-interventional myocardial infarction (MI) according to the guidelines definitions and stent thrombosis, as defined by the academic research consortium’s definitions.10 11 Additionally, information about any target-vessel revascularisations (TVR), non-TVRs, transitory ischaemic attacks/strokes, major bleedings by Bleeding Academic Research Consortium (BARC) definitions, cardiac and non-cardiac deaths were collected during 1-year follow-up.
Sample size estimation
The sample size estimations were based on the investigators’ clinical experience, as there has not been published any comparable study until now, on which statistical consideration could refer. Using a significance level of α=0.05 at 80% power for two-sided test and null difference between proportions equal to 0 with assumption of frequency of primary end point (optimal stent expansion and apposition) occurrence in study and in standard group 40% and 80%, respectively, the study sample size was calculated to require at least 23 subjects per group for a total study population of 46 subjects per trial.
Statistical analysis
The analyses were performed using SAS V.9.4 (SAS Institute, Cary, North Carolina, USA). Results are presented on the analyses performed according to intention-to-treat (ITT) principle, because it tends to avoid overoptimistic estimates of efficacy and because of small sample size. In order to increase statistical power, we decided to pool the data for the primary analyses.
For comparison of the baseline demographics according to allocated groups (standard predilatation using SCBs vs high-pressure predilatation), differences in continuous variables were analysed by t-tests, Mann-Whitney U test or paired t-test as appropriate and differences in categorical variables by χ2 tests. A p value <0.05 was considered statistically significant.
Results
Study population
The pooled study population consisted of 104 patients (n=60 in Pre-NC study and n=44 in OPRENBIS study). In total, 51 and 53 patients were randomised to predilatation with SCBs or NCBs, respectively (figure 1). The baseline characteristics are displayed in table 1. In brief, the mean age was 64.0±8.6 years in the NCB group and 62.3±11.2 years in the SCB group (p=0.4). Cardiovascular risk factors and past medical history were well balanced between compared groups. The demographics of the two study cohorts are separately displayed in the online supplementary table 1.
Supplemental material
Baseline characteristics of the study population grouped according to allocated predilatation strategy (non-compliant vs semi-compliant balloons).
Procedural characteristics
A total of 110 lesions were treated, 54 in the NCB group and 56 in the SCB group. Angiographic and procedural characteristics are depicted in table 2. The lesion and procedural characteristics of the Pre-NC and OPRENBIS studies are separately shown in the online supplementary table 1. AHA lesion classification was not significantly different between the NCB versus SCB groups. Presence and severity of angiographically visible calcification was similar between both groups (p=0.99) as was lesion length (19.3±10.1 vs 21.1±9.4, p=0.25). The diameter of the balloons used for predilatation was similar (p=0.86). Mean predilatation pressure was higher in the NCB group (24.2±6.6 vs 14±3.3, p<0.0001). Absorb BVS were implanted in 55% of the patients in the SCB group and 58% of the patients in the NCB group (p=0.72). Postdilatation was performed in 41 (76%) NCB patients and 46 (82%) SCB patients. Mean postdilatation pressure was 22.8±8.3 atm in the NCB group and 23.5±8.6 atm in the SCB group (p=0.82). Similar diameter sizes of postdilatation balloon were used in both groups (p=0.26).
Lesion and procedural characteristics
In patients treated with BVS compared with metallic stents, postdilatation was more frequently performed and the applied pressures were higher (displayed in the online supplementary table 2).
Supplemental material
OCT and angiographic measurements
OCT measurements are summarised in table 3. Overall, 45 (88%) patients in the SCB group and 49 (92%) patients in the NCB group fulfilled the core-lab quality criteria for OCT assessment and were included in this analysis. Distal and proximal reference area was similar between both groups. After stent implantation, in-stent minimal luminal diameter was significantly better in the NCB group (2.47±0.40 mm vs 2.37±0.32 mm, p=0.03) and after postdilatation in-stent minimal luminal diameter increased in both groups and was slightly larger in the NCB group (2.57±0.42 mm vs 2.47±0.33 mm, p=0.08).
Lesion assessment based on OCT measurements after stent/scaffold implantation and after postdilatation
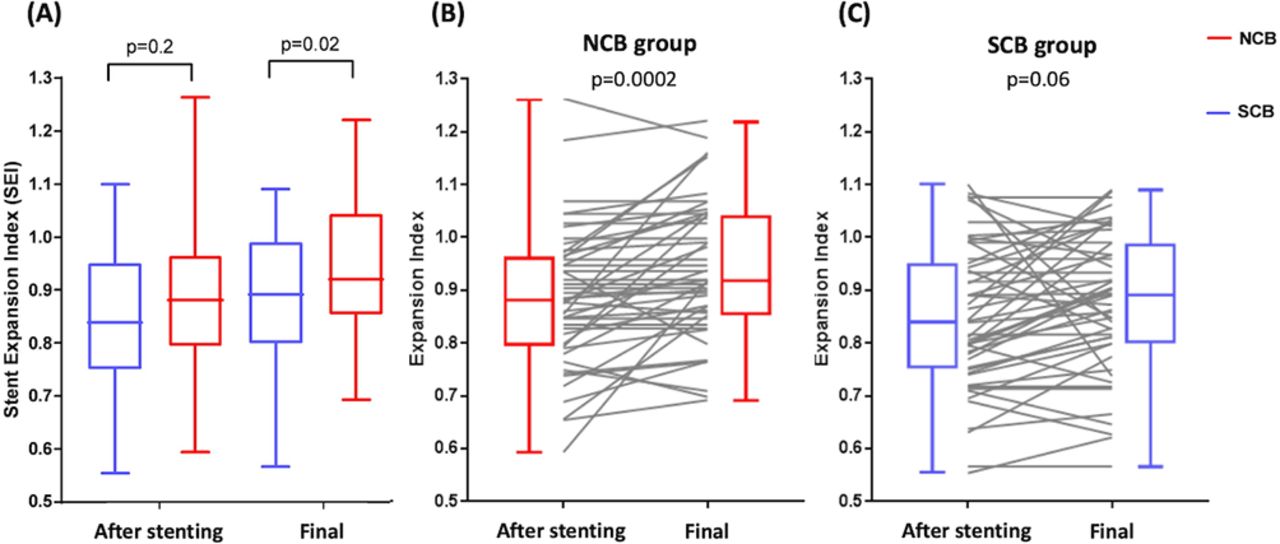
Immediately after stent implantation, SEI was 0.88±0.13 in the NCB vs 0.85±0.14 in the SCB group (p=0.18). SEI was <0.8 in 27% of all patients in the NCB group and 42% of all patients in the SCB group (p=0.14). After postdilatation, SEI increased to 0.94±0.13 in the NCB group vs 0.88±0.13 in the SCB group (p=0.02). Finally, the fraction of patients with SEI <0.8 dropped to 15% of the patients in the NCB group and 25% of patients in the SCB group (p=0.18).
When analysing the patients treated with metallic stents or BVS separately, we found that final SEI was significantly larger, when lesions treated with DES were predilated with NCBs compared with SCBs (0.95±0.11 vs 0.86±0.13 (p=0.036)). On the other hand, final SEI in lesions treated with BVS did not significantly differ between lesion pretreated with NCBs versus SCBs (0.94±0.14 vs 0.89±0.13 (p=0.17)) (shown in the online supplementary table 3).
Periprocedural safety and long-term clinical outcomes
Periprocedural OCT and angiographic safety outcomes are displayed in table 4. Overall, periprocedural safety was good and no perforations of coronary artery occurred. Proximal and distal edge dissections were mainly seen on OCT and were comparable between both groups.
Procedural complications evaluated by angiography and OCT
One-year clinical follow-up was available in all patients and is summarised in table 5. One patient from the NCB group had a non-cardiac death and one patient in the SCB group had an MI and needed TVR. No patient had probable or possible ST.
Clinical end points after 1-year follow-up
Discussion
When analysing pooled data from two proof-of-concept studies including unselected patients with CAD requiring PCI, we found that the use of NCBs at high pressure for predilatation and postdilatation results in better stent expansion compared with predilatation with SCBs. This approach appears to especially improve final SEI when implanting metallic stents. Additionally, we showed that the use of high-pressure inflations with dedicated NCBs was safe and did not lead to any relevant coronary dissections or vessel perforations.
Although short-term outcomes after PCI have tremendously improved with use of latest generation DES, repeat ischaemic event requiring medical attention or interventions, especially target lesion failures and revascularisations, over 5 years remain high, especially in patients with multivessel disease, diabetes or complex lesions.12–14 The presence of diabetes, the use of multiple stents (long lesions), ISR, chronic total occlusion and vessel diameter <3 mm are known independent predictors of target lesion failure.1 Mechanical factors, including small diameter stents, stent underexpansion and malapposition, are still very important factors contributing to ISR and ST in the current DES era.2 15–19
In this context, the minimum stent area reflecting stent expansion postimplantation is an important independent predictor of ISR and ST.15 Theoretically, three measures can be considered to achieve the largest minimum stent area or SEI possible: (1) adequate lesion preparation, (2) optimal stent/scaffold sizing and (3) appropriate postdilatation once the stent/scaffold is implanted.3 20–22
The routine use of an SCB for lesion preparation still represents common practice, but while it facilitates stent delivery, it might fail to properly crack the lesion, in particularly in fibrotic and/or calcified lesions, and therefore prepare the lesion site for device implantation. One needs to take into account that most PCI procedures are performed without intravascular imaging, which usually facilitates characterisation and appreciation of the lesion. Hence, one might easily underestimate the complexity of a lesion and accordingly misses to adequately predilate a lesion, which in turn can contribute to stent and scaffold underexpansion.
As demonstrated in our study, better stent expansion was achieved immediately postdevice implantation when an NCB was used for lesion preparation, but the difference did not reach statistical significance. Postdilatation was performed in both groups in a similar fashion (comparable diameters and pressures of NCBs) and this led to a relevant increase in stent expansion in the NCB group, while only mildly increasing SEI in the SCB group (figure 2).
{kind=link}
{kind=link}
Stent expansion index (SEI) assessed by optical coherence tomography (A) after device implantation and postdilatation in the semi-compliant balloon (SCB) group vs non-compliant balloon (NCB) group, (B) SEI after predilatation and postdilatation in the NCB group and (C) SEI after predilatation and postdilatation in the SCB group.
To comprehend these differing results, we need to consider the impact of balloon angioplasty with SCB versus NCB on the arterial wall. While SCBs tend to expand into the ‘softer’ (compliant) part of the vessel, dedicated NCBs are able to tackle the calcified and fibrotic parts of the lesion, especially if a high balloon-to-vessel ratio is used. Additionally, with NCBs increasing pressures beyond nominal values leads to an exponential rise in balloon diameter. Contrary to this, there is a linear diameter-pressure relationship in NCBs, allowing the use of higher pressure, with less risk for coronary artery rupture. For instance, the OPN NC balloon can be safely inflated above rated burst pressure of 35 atm with minimal increase in diameter and appears therefore an ideal device for complicated fibro-calcific lesions, with recoil tendency.7 23
A recent post hoc analysis of two randomised studies using contemporary DES demonstrated that adjunct postdilatation was not associated with a reduction of major adverse cardiac events at 1 year among patients treated with everolimus-eluting stents, irrespective of lesion length or vessel diameter.24 Putting the results of our study into clinical perspective, the postulated lack of efficacy of postdilatation might not be surprising since direct stenting or lesion preparation with smaller SCBs are still very popular in most catheterisation laboratories. It is obvious that many coronary lesions can probably be treated without aggressive predilatation. However, interventionalists should vigorously ensure optimal stent expansion and apposition in order to avoid adverse short-term and long-term outcomes, including restenosis or stent/scaffold thrombosis. As indicated by our results, achieving optimal stent expansion might require both adequate predilatation and postdilatation. This concept is novel and might lead to paradigm change when addressing lesion preparation in the future.
The fact that we did not find a significant difference between lesion preparation with NCBs versus SCBs in patients treated with Absorb BVS, might be explained by differences in procedural characteristics. Among lesions treated with BVS, the percentage of postdilatations was higher and most lesions were actually postdilated with the OPN NC balloon at very high pressures (>25 atm), which could have helped to optimise final SEI.
Although we present the first randomised comparisons of two different lesion preparation strategies, we are well aware of certain limitations: (1) we pooled data from two randomised trials with similar protocols and identical implantation strategies in order to increase the sample size, which was not preplanned; (2) while the Beo NC and the OPN NC are both NCBs, the latter is a highly NCB with a very flat compliance curve allowing the use of very high pressure (>30 atm); (3) both studies were designed and conducted during an era, when BVS devices were very popular. Hence, we present data from a mixed population treated with either contemporary metallic stents and the Absorb BVS. In fact, 73% of all patients enrolled in the Pre-NC trial were treated with a third-generation DES, while in the OPRENBIS trial, patients were treated with BVS only. BVS depend on vigorous lesion preparation, which may have magnified the effect of vessel preparation using NCBs. This variation in lesion treatment may account for differences in final luminal results observed. It is also important to take into account that the use of the Absorb BVS outside of randomised trials had been downgraded to a class III recommendation by various guideline committees and it should therefore not be a comparator with latest generation DES in clinical practice; (4) overall, our two studies were not designed to assess clinical efficacy and need to be considered as pilot data. Therefore, the concept of aggressive predilatation using NCBs for lesion preparation needs further clinical evaluation by prospective studies, which are adequately powered for clinical end points.
Conclusions
In simple coronary lesions, adequate predilatation and postdilatation with NCBs at high pressures seems to result in better stent and scaffold expansion. In fact, using SCBs for predilatation might lead to inadequate stent expansion and postdilatation with NCBs at high pressures might only partially correct this. It is important to note that predilatation and postdilatation using NCBs at high pressure appear safe. Whether this approach leads to superior clinical long-term outcomes needs to be assessed in further clinical trials.
Supplemental material
References
Footnotes
FC and MB are joint first authors.
Twitter @MatthiasBossard
FC and MB contributed equally.
Contributors FC (principal investigator) designed the study, organised funding, monitored the data collection, wrote the statistical analysis plan and drafted and revised the paper. MB contributed to data collection, data analysis and drafted and revised the paper. WZ monitored the data collection, conducted the core lab and statistical analyses and reviewed the manuscript. FM contributed to the data analyses and drafting of the manuscript. MV and MW contributed to the data collection and reviewing of the manuscript. KPM monitored the data collection, conducted the core lab and statistical analyses and reviewed the manuscript. ST contributed to data collection and reviewed the paper. RK (co-principal investigator) designed the study, organised funding, monitored the data collection, drafted and reviewed the paper.
Funding This is an independent investigator-initiated study. Swiss Interventional Systems (SIS) Medical, Frauenfeld (Switzerland) provided research grants for the Pre-NC and OPRENBIS studies (funding for core-lab analyses).
Competing interests FC has received speaker fees and research grants from Abbott Vascular and SIS Medical. RK has received institutional grant support from Abbott, Biotronik, Biosense Webster, Boston Scientific, Medtronic and SIS Medical. None of the other authors had any relevant conflicts of interest.
Patient consent for publication Not required.
Ethics approval The studies were approved by the local ethics committee and complied with the Declaration of Helsinki.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available on reasonable request. All data relevant to the study are included in the article or uploaded as supplementary information.