Article Text

Abstract
Aim To evaluate the impact of preinterventional moderate-to-severe functional tricuspid regurgitation (FTR) on early outcome after percutaneous edge-to-edge mitral valve repair (pMVR) with MitraClip procedures for functional mitral regurgitation (FMR) in patients with heart failure with reduced ejection fraction (HFrEF).
Methods and results From January 2013 to December 2017, 80 patients with HFrEF (ejection fraction 22%±5.3%) and FMR (grade 3.0±0.36) underwent successful pMVR. The 3-year actuarial survival was 58%. However, 73% (n=22) of non-survivors died of cardiac failure within 1 year. Patients were categorised into none-to-mild (n=36) and moderate-to-severe (n=44) postinterventional FTR groups according to pre-MitraClip tricuspid regurgitation grade. Cox regression analysis on 1-year survival demonstrated an impact of FTR severity (HR=1.8, 95% CI 1.01% to 3.09%, p=0.047), preoperative New York Heart Association class (HR=2.8, 95% CI 1.2% to 6.5%, p=0.015) and peripheral artery disease (HR=5.4, 95% CI 1.6 to 18, p=0.0054). Kaplan-Meier analysis showed that 1-year cardiac death was higher in the moderate-to-severe FTR group (p=0.048). In our study, 77% of pre-MitraClip moderate-to-severe FTR cannot be significantly reduced. Post-MitraClip moderate-to-severe FTR grade was related to lower survival (p<0.001).
Conclusion In patients with HFrEF treated with MitraClip for FMR, moderate-to-severe FTR was an independent predictor of cardiac death within 1 year. To improve survival, additional therapy to residual FTR should be considered in early phase after MitraClip therapy.
- tricuspid valve disease
- mitral regurgitation
- cardiac surgery
- heart failure
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known about this subject?
Functional tricuspid regurgitation (FTR) is a common finding in the presence of functional mitral valve regurgitation, and untreated moderate-to-severe FTR is known as a predictor of poor survival.
What does this study add?
In patients with heart failure with reduced ejection fraction undergoing percutaneous edge-to-edge mitral valve repair (pMVR), postinterventional moderate-to-severe tricuspid regurgitation (TR) grade was an independent predictor of cardiac death within 1 year.
77% of pre-MitraClip moderate-to-severe FTR cannot be significantly reduced.
How might this impact on clinical practice?
Residual moderate-to-severe TR might require dedicated additional procedures (an additional TR intervention) even if pMVR was successful.
Introduction
Functional tricuspid regurgitation (FTR) is a common finding in the presence of functional mitral valve regurgitation (FMR).1–3 In case of moderate-to-severe FTR, tricuspid valve (TV) repair is usually performed simultaneously when patients undergo mitral valve surgery. In the modern era, isolated percutaneous edge-to-edge transcatheter mitral valve repair (pMVR) with the MitraClip system (Abbott Vascular, Menlo Park, California) for FMR in patients with a high risk of perioperative mortality and comorbidities is available and has become increasingly favoured over sMVR (surgical mitral valve repair), representing a less invasive beating-heart interventional technique.4–7 According to a recent randomised study, early clinical results of pMVR were acceptable in patients with heart failure with reduced ejection fraction (HFrEF).8 Concomitant FTR ameliorates by itself in some patients treated for FMR, but remains significant in others. Simultaneous TV edge-to-edge repair (transcatheter mitral plus tricuspid valve edge-to-edge repair) in addition to pMVR has been described but is not routinely performed in clinical practice.9 In general, untreated moderate-to-severe FTR is known as a predictor of poor survival, yet the prognostic role of FTR severity after pMVR has not yet been investigated. Therefore, the present retrospective study aimed to evaluate the impact of FTR severity in the early phase after pMVR in patients with HFrEF and symptomatic FMR.
Methods
Patient selection
Since the start of our MitraClip programme in 2013, individual treatment selection has been based on a multimodal decision-making process based on age, evaluation of surgical risk by logistic EuroSCORE, as well as adjunctive risk evaluation (liver dysfunction, during chemotherapy for malignancy and frailty). In addition, preoperative echocardiography played a critical role in patient selection for MitraClip implantation according to the German Cardiac Society (DGK) criteria.10 In selected cases, patients were enrolled in the programme despite extremely poor left ventricular (LV) function (ejection fraction <15%).
Echocardiography
Transthoracic echocardiography (TTE) data were available for all patients preoperatively. All patients had TEE (Transesophageal echocariography) during MitraClip implantation and at discharge. The TTE examinations were performed by two experienced cardiologists, and all evaluations were carried out according to standard techniques recommended by the American Society of Echocardiography.11 Assessment of right ventricular (RV) function was performed from the apical four-chamber view. The severity of tricuspid regurgitation (TR) assessed by Doppler echocardiography was classified as none/trivial (0), mild (1), moderate (2), moderate-severe (3) or severe (4). Pulmonary artery pressure was also measured by TTE.
pMVR with MitraClip procedure
Prior to MitraClip implantation, all patients underwent coronary angiography to exclude relevant coronary artery disease necessitating revascularisation. All MitraClip procedures were performed by one experienced interventional cardiologist. All clips (arm length of 9 mm) were implanted according to standard practices under general anaesthesia with TEE and fluoroscopic guidance. Additional clips were placed until the residual mitral valve regurgitation (MR) corresponded to a maximum grade of 2 at a mean blood pressure of 60 mm Hg.
Postoperative course, endpoint and follow-up
All patients who were treated in our hospital between January 2013 and December 2017 were enrolled. After pMVR, all patients were admitted to the intensive care unit (ICU), before they were further moved to the cardiology ward. The clinical follow-up was closed on 31 December 2018, when the last enrolled patient had completed 1 year of follow-up. The median follow-up was 24 months (IQR: 11–34 months; range: 0.17–70 months). Follow-up data of clinical status were obtained from patients’ general practitioners or private cardiologists by phone calls and facsimile, and were completed in 98% of patients. The primary endpoints of the study were 1-year and 3-year survival.
Statistical analysis
Results are expressed as mean±SD or as median +25th–75th percentile IQR for continuous variables, and frequency and percentage for categorical variables. Univariable comparisons were performed with Student’s unpaired t-test for continuous normally distributed data. The Mann-Whitney U test was used for comparisons of non-parametric continuous data and Fisher’s exact test for categorical data. Data for survival and freedom from cardiac events and all-cause death were derived using the Kaplan-Meier method; comparisons were made using the log-rank test. The association between postinterventional TR severity and occurrence rate of 1-year cardiovascular event (cardiac death) was evaluated with Cox regression analysis, and the results were expressed as HR with 95% CI. Candidate covariates were chosen based on previous medical knowledge; then, a backward stepwise selection was performed. Differences were considered statistically significant at p<0.05. Statistical analysis was performed using SPSS for Windows V.22.0.
Results
Study cohort and characteristics
Eighty-five patients with moderate-to-severe FMR and HFrEF (≤30%) were treated with pMVR in our hospital between January 2013 and December 2017. Patients with acute emergency treatment, redo-pMVR, organic mitral or TV disease and those who were lost to follow-up (n=2) were excluded. Moreover, three (3.5%) patients with unsuccessful pMVR (defined as postoperative MR grade of 3 or more) were also excluded for the purpose of surveying the accurate impact of pMVR, resulting in 80 patients (age 72±8.7 years, 60% male) with end-stage cardiomyopathy (non-ischaemic n=41; ischaemic n=39) who underwent MitraClip therapy. Left ventricular ejection fraction (LVEF) showed a mean of 22%±5.3%. Preoperative echocardiography showed LVEF ≤15% in 13 (16%) patients. Baseline TR had a mean grade of 1.63±0.75. The characteristics of baseline and preoperative echocardiography are shown in tables 1 and 2.
Baseline characteristics of the full cohort
Baseline results of transthoracic echocardiography in the full cohort
Predictors of early cardiac death
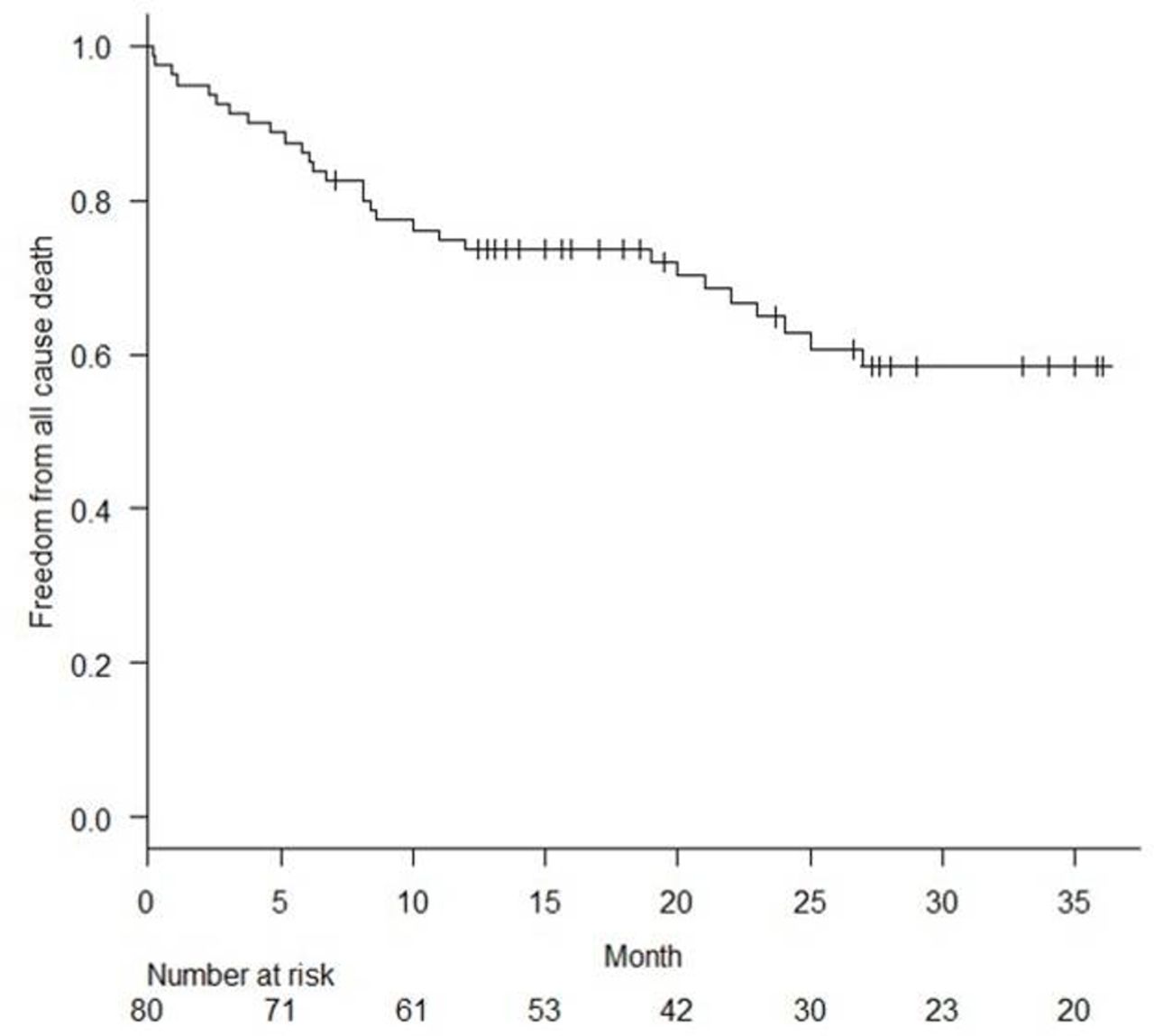
The Kaplan-Meier estimate for overall survival at 3 years was 57.4%. Survival rate at 1-year follow-up was 72.5%. All these 22 patients died of cardiac death within 1 year, although pMVR was successful (figure 1). Multivariate Cox regression analysis for 1-year survival identified preoperative TR grade (HR=1.765, 95% CI 1.007 to 3.093, p=0.047), preoperative New York Heart Association (NYHA) grade (HR=2.811, 95% CI 1.222 to 6.469, p=0.015) and peripheral artery disease (HR=5.376, 95% CI 1.642 to 17.6, p=0.0054) as independent predictors at 1-year survival (table 3). Other variables including ischaemic versus non-ischaemic origin, preoperative LVEF, and other parameters of echocardiography were not found as predictors.

{kind=link}
Clinical outcome of the full cohort. Kaplan-Meier curves for freedom from all-cause death estimated at 72.5% at 1 year and 57.4% at 3 years.
Cox regression model analysis for cardiac death at 1-year follow-up
Preprocedural characteristics and periprocedural results according to TR grade
According to preoperative TR severity, this cohort was divided into none-to-mild FTR group (36 patients, 45%) and moderate-to-severe FTR group (44 patients, 55%) (TR grade: 0.92±0.28 vs 2.2±0.42, p<0.001). When comparing these two groups, there were no significant differences in preoperative characteristics and echocardiography, including the parameters of RV dimension, pulmonary artery hypertension and tricuspid annual plane systolic excursion. The details of the baseline characteristics of the two groups are shown in table 4. In-hospital death occurred in two (2.5%) patients, regardless of extracorporeal membrane oxygenation and intra-aortic balloon pump, because of postoperative cardiogenic shock state, although postoperative MR severity was reduced to an MR grade of 1. Of these, one patient with a TR grade of 1 had a preoperative high value of logistic EuroSCORE of 44% with LVEF of 10% and died after 8 days. The other patient with a TR grade of 2 had high surgical risk of 30% with LVEF of 17% and died after 5 days.
Preprocedural characteristics and echocardiography between none/mild and moderate/severe TR grade
There were no cases of postoperative cardiac tamponade or new pacemaker implantation. There was no significant difference in postoperative MR severity (p=0.37) between the two groups. However, there was a trend towards higher number of implanted clips in the moderate-to-severe TR group (2.23±0.71 vs 1.92±0.69, respectively; p=0.053). In addition, extubation rate in the hybrid room (p=0.28), duration of ICU stay (p=0.39) and total hospital stay (p=0.24) were not significantly different between the two groups. The discharge rate to home was similar at 89% in both groups. Intraprocedural results and periprocedural outcomes are presented in table 5.
Perioperative course
Clinical impact of preprocedural TR severity
In the Kaplan-Meier analysis, the rates of freedom from cardiac death were significantly higher for preprocedural none-to-mild TR group at 1-year follow-up (p=0.048) (online supplementary figure 1). Clinical outcomes at 1-year follow-up are shown in table 6. Between the two groups, there were significant differences in rehospitalisation due to heart failure (p=0.021) and trend towards higher cardiac death (p=0.077). A total of five patients required LV assist device implantation (n=2) or mitral valve replacement (n=3) due to clip failure at 1-year follow-up, but this was not significantly different between the two groups. NYHA grade of survivors at 1 year was not statistically different.
Supplemental material
Clinical outcomes during 1-year follow-up
Postprocedural TR grade influencing survival
Postprocedural moderate-to-severe FTR grade was noted in 38 (47.5%) patients. The low TR grade in the none-to-mild pre-MitraClip TR group was preserved post-MitraClip (0.92±0.28 vs 1.03±0.45, p=0.103), whereas the TR grade of the moderate-severe group significantly improved (2.23±0.42 vs 1.93±0.62, p=0.0034). Online supplementary figure 2A,B shows the alteration of TR grade before and after MitraClip therapy. Overall, TR grade was reduced in 16 (20%) patients, preserved in 56 (70%) and increased in 8 (10%). Preprocedural moderate-to-severe TR grade was decreased to mild TR grade in 10 (23%) patients, but no improvement in TR grade in 34 (77%) patients postprocedure. In the Kaplan-Meier analysis, the rates of freedom from all-cause death were significantly higher for postprocedural none-to-mild FTR group at 1 and 3 years of follow-up (p=0.0007 and p=0.0020, respectively) (online supplementary figure 3). Moreover, in 34 patients with preoperative moderate-to-severe TR grade, all-cause survival rate was significantly higher in the 15 patients with postoperatively improved TR grade than in the 19 patients with non-improved TR grade at 1 and 3 years of follow-up (p=0.031 and p=0.012, respectively). Meanwhile, preprocedural none-to-mild TR grade was increased to moderate-to-severe TR grade in four patients (11.1%) (online supplementary figure 2A). One of these four patients died of heart failure during follow-up.
Clinical impact of postoperative moderate-to-severe TR in ischaemic versus non-ischaemic cardiomyopathy
Survival rate for all-cause death between the ischaemic and non-ischaemic groups, regardless of residual TR severity, was not significantly different (online supplementary figure 4A,B). Multivariate Cox regression analysis identified postprocedural TR grade as an independent predictor of 1-year survival in the non-ischaemic group, but not in the ischaemic group (table 7). In the Kaplan-Meier analysis, survival rate for all-cause death at 1 and 3 years of follow-up was not significantly different between patients with ischaemia with postoperative none-to-mild TR and those with postoperative moderate-to-severe TR (p=0.125 and 0.0748, respectively), but it was significantly different among the non-ischaemic patients (p=0.00426 and p=0.00433, respectively) (online supplementary figure 4C,D).
Cox regression model analysis for cardiac death at 1-year follow-up in ICM and DCM groups
Discussion
We studied the impact of FTR in patients with HFrEF (LVEF ≤30%) with high surgical risk undergoing pMVR.
The main findings of the current study are as follows. First, the periprocedural mortality (2.5%) is acceptable and not affected by FTR severity in patients with HFrEF. Second, preprocedural moderate-to-severe FTR grade is an independent predictor of cardiac death at 1 year in patients with HFrEF, even if the MitraClip therapy is successful with regard to the reduction of FMR. Third, residual moderate-to-severe FTR grade is a predictor of cardiac death at 1 year and all-cause mortality at midterm follow-up in patients with non-ischaemic, but not in ischaemic cardiomyopathy.
Residual moderate-to-severe FTR grade was significantly associated with early mortality. In our cohort, only 23% of cases with preoperative moderate-to-severe FTR grade could be reduced to mild FTR by pMVR, leaving 77% of patients at high risk of early mortality. As pMVR alone is not able to relieve FTR effectively in these patients, an additional intervention reducing FTR might be necessary in order to address left-sided and right-sided heart disease individually.
FTR is caused by TV annular dilation12 and is often related to increased tethering of tricuspid leaflets due to RV enlargement owing to pulmonary hypertension.13 14 A reported echocardiographic study emphasised that moderate-to-severe TR can increase the mortality rate regardless of pulmonary hypertension or low ejection fraction.15 According to the literature, dilation of the right ventricle correlates with poor prognosis in patients with severe LV dysfunction.16 In our two groups, none of the echocardiographic variables assessed were significantly different except for TR severity (table 2). Although there is no information about TV annulus diameter, we considered that these two groups might be different in terms of the preoperative TV annulus diameter influencing the FTR severity. However, it should be noted that the function of the right ventricle cannot be easily quantified by echocardiography due to its complex geometry. Recent studies have described that severe FTR or pulmonary hypertension may increase mortality after MitraClip procedure.17 18 In our cohort with severely reduced LV systolic function, mild-to-severe preinterventional FTR was a predictor of mortality after MitraClip therapy, but not pulmonary hypertension. Postcapillary pulmonary hypertension as an immediate consequence of MR usually decreases after the procedure, whereas TR, reflecting sustained RV volume and pressure overload, seems to represent a structural defect in itself when present. The relation between efficiency of MitraClip and pulmonary artery pressure over time needs to be further studied.
Although our study was performed at a single centre, our outcomes reflect real-world practice, at least for high-volume centres in Germany. Our patients had severe LV dysfunction (mean LVEF of 22%±5.3%), as reflected by a high risk for surgical mortality (mean logEuroSCORE 34%±20%). Our clinical outcomes compared well with a previous large cohort study.8
In our cohort, 55% of patients had preoperative moderate-to-severe TR grade, yet the difference in preoperative TR severity did not have any influence on perioperative mortality (table 5) or duration of ICU stay (1.22±1.2 vs 1.55±2.0 days, p=0.39). The proportions of patients with none-to-mild FTR and those with moderate-to-severe FTR who were discharged home were 88.9% and 88.6%, respectively (p=ns), showing that pMVR can be safely performed in patients with HFrEF and high surgical risk.
Some authors have suggested that moderate-to-severe FTR in patients undergoing mitral valve surgery alone is strongly related to lower survival at midterm follow-up.19 Generally, the residual MR grade after pMVR is greater than that after mitral valve surgery. Therefore, residual FTR severity is difficult to be reduced and seems to have more significant influence on cardiac death. In patients with HFrEF with postprocedural moderate-to-severe TR, attempts to treat FTR need to be discussed, even if pMVR is successful. Interestingly, 77% of patients with preprocedural moderate-to-severe FTR showed no improvement in FTR postoperatively and more than 40% died within 1 year because of heart failure. Echocardiographic variables of our two groups were similar, except for TR severity (table 4). As suggested in our study, preprocedural FTR severity seems to be an important predictor of poor survival.
Interestingly, early survival was not related to residual TR grade in patients with ischaemic cardiomyopathy (ICM), but was in patients with dilated cardiomyopathy (DCM). Most published reports concluded that survival both in patients with DCM and in patients with ICM is similar at midterm follow-up, which is in line with the findings of our study.20 However, this was not differentiated by residual TR severity so far. We hypothesise that high-grade residual TR in DCM represents a risk factor in itself and should be considered a therapeutic target in order to improve survival in patients with DCM.
As recent studies have suggested that transcatheter tricuspid edge-to-edge repair (TTVR) can reduce the severity of FTR,21 future studies should investigate if TTVR can improve survival in patients with residual moderate-to-severe FTR after pMVR in patients with HFrEF. We suggest that patients with moderate-to-severe preprocedural FTR should be observed carefully after MitraClip procedure. If FTR does not improve, additional interventional therapy should be considered early.
Limitations
This observational study was conducted at a single centre. Although patients were selected from a real-world clinical setting, the patient population was relatively small and the follow-up duration was relatively short. There were no CMR (Cardiovascular magnetic resonance) data available which would have allowed for more advanced analysis of RV function. In our study, preoperative NYHA grade was identified as an independent predictor of 1-year survival. However, preoperative NYHA grade might not entirely represent heart failure because of severe frailty in this cohort.
Conclusion
MitraClip therapy in patients with HFrEF was safe, regardless of preoperative FTR severity. However, preoperative FTR was not significantly improved. In our study, preoperative FTR was a major predictor of cardiac death at 1-year follow-up. Future studies are necessary to determine the value of additional TTVR in patients with residual moderate-to-severe FTR in the early phase after pMVR.
References
Footnotes
Contributors All persons who meet the authorship criteria are listed as authors, and all authors certify that they have participated sufficiently in the work to take public responsibility for the content, including participation in the concept, design, analysis, writing or revision of the manuscript. Furthermore, each author certifies that this material or similar material has not been and will not be submitted to or published in any other publication before its appearance in Open Heart. TG, DM: conception or design of the work, and acquisition, analysis and interpretation of data for the work. SS, KR, OG, SJ: conception or design of the work, and agreement to be accountable for all aspects of the work. DF, DM: final approval of the version to be published and agreement to be accountable for all aspects of the work.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval This single-centre study was approved by the Institutional Review Board of Sana Heart Center in Cottbus (Germany). The study complied with the Declaration of Helsinki. The study protocol was discussed with local ethics authorities (Ärztekammer Brandenburg, Germany), and ethical approval was waived due to the retrospective design of the study.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available in a public, open access repository. Data are available upon reasonable request. All data relevant to the study are included in the article or uploaded as supplementary information. Upon receiving approval from the Institutional Review Board of the Sana Heart Center, we retrospectively reviewed the records of consecutive patients who, between January 2013 and January 2018, had undergone medication therapy alone, repeat MitraClip therapy, or surgical revision for persistent or recurrent MR after percutaneous MitraClip therapy.