Article Text

Abstract
Objective A score to distinguish Takotsubo syndrome (TS) from acute coronary syndrome would be useful to facilitate appropriate patient investigation and management. This study sought to derive and validate a simple score using demographic, clinical and ECG data to distinguish women with non-ST elevation myocardial infarction (NSTEMI) from NSTE-TS.
Methods The derivation cohort consisted of women with NSTE-TS (n=100) and NSTEMI (n=100). Logistic regression was used to derive the score using ECG values available on the postacute ward round on day 1 post-hospital admission. The score was then temporally validated in subsequent consecutive patients with NSTE-TS (n=40) and NSTEMI (n=70).
Results The five variables in the score and their relative weights were: T-wave inversion in ≥6 leads (+3), recent stress (+2), diabetes (−1), prior cardiovascular disease (−2) and ST-depression in any lead (−3). When calculated using ECG values obtained at admission, discrimination between conditions was very good (area under the curve (AUC) 0.87 95% CI 0.83 to 0.92). The optimal score cut-point of ≥1 to predict NSTE-TS had 73% sensitivity and 90% specificity. When applied to the validation cohort at admission, AUC was 0.82 (95% CI 0.75 to 0.90) and positive and negative predictive values were 78% and 81%, respectively. On day 1 post-admission, AUC was 0.92 (95% CI 0.87 to 0.97), with positive and negative predictive values of 77% and 91%, respectively.
Conclusion This NSTE-TS score is easy to use and may prove useful in clinical practice to distinguish women with NSTE-TS from NSTEMI. Further validation in external cohorts is needed.
- takotsubo syndrome
- non-ST segment elevation myocardial infarction
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known about this subject?
Patients with Takotsubo syndrome (TS) commonly present with symptoms similar to patients with acute coronary syndrome (ACS), therefore, the initial diagnosis and treatment remains challenging. A score that can be used at the bedside to distinguish TS from non-ST-segment elevation myocardial infarction (NSTEMI) would be useful to facilitate appropriate patient investigation and management.
What does this study add?
Our study derives and temporally validates a clinically focused score using history and ECG data to distinguish women with NSTE-TS from those with NSTEMI. Our score includes just five clinical parameters, which can be easily obtained at the initial evaluation of women with suspected NSTE-TS. The more positive the score, the more likely the patient is to have TS; the more negative the score, the more likely it is to be NSTEMI.
How might this impact on clinical practice?
Our score can be easily calculated on admission and on the post-acute ward round, and may be helpful in planning the initial evaluation of women who present with suspected ACS. In patients where TS is suspected, early echocardiography should be performed to identify the typical symmetric wall motion abnormalities. In women with scores >1, particularly those with typical echocardiogram appearances, it may be reasonable to undertake CT rather than invasive coronary angiography to assess atherosclerotic coronary artery disease.
Introduction
Takotsubo syndrome (TS) (also known as apical ballooning syndrome) is an acute heart failure condition characterised by acute but rapidly reversible left ventricular (LV) dysfunction with distinct wall motion abnormalities subtending more than one coronary artery territory.1–3 At presentation TS typically mimics acute coronary syndromes (ACS) caused by coronary thrombosis, but the pathophysiology differs and the two conditions need to be distinguished for appropriate treatment. The InterTAK diagnostic score uses a multivariable model to differentiate TS from ACS at admission in both men and women.4 However, over 90% of patients with TS are women.1 5 Moreover, in about one-third of patients with TS the initial ECG exhibits ST elevation6–10 and the patient will typically undergo immediate coronary angiography and LV imaging which will exclude an occluded coronary artery and confirm the TS diagnosis. The remaining two-thirds of patients with TS present without non-ST-segment elevation-TS (NSTE-TS) on ECG9 10 and are often investigated and managed initially as possible NSTE myocardial infarction (NSTEMI). It would be useful to have a simple clinical score, able to be done at the patient’s bedside soon after they present, to determine whether TS is a likely diagnosis in patients with suspected ACS without ST-elevation, and to aid the clinician in deciding on appropriate investigations and management.
Due to the differing pathophysiology of the two conditions, there are several possible distinguishing variables, which may contribute to such a score. The most obvious is that TS occurs predominantly in women, so any suspected ACS in a man is unlikely to be TS. Because of the very low incidence of TS in men, a score is unlikely to be useful in clinical practice to distinguish between TS and ACS. We, therefore, chose to develop a score specifically for use in women. Some clinical features may make a diagnosis of ACS more likely, including the presence of atherosclerotic risk factors11 12 and ST depression on the ECG.13 In contrast, the association of TS with acute physical or psychological stress may point towards TS. We recently reported that the evolution of ECG changes after admission differs between those with TS and ACS.13 In that study, the ECG finding which best distinguished between NSTE-TS and NSTEMI was the presence of widespread T-wave inversion (TWI) in six or more leads late after admission, with ST segment depression at and after admission also being useful.13
We aimed to develop a score using demographic, clinical and ECG data which could distinguish women with NSTEMI from those with NSTE-TS. We evaluated the discriminative value at admission and on day 1 post-admission, predicting that the score would perform best on the day after admission when the ECG changes have been shown to better differentiate the two conditions. Because TS is less common than ACS, a score with good sensitivity and specificity does not necessarily distinguish the less common from the more common diagnosis when used in practice. We, therefore, also assessed the performance of the score (temporally validated) in a prospectively recruited, consecutive cohort of women presenting with suspected NSTEMI.
Methods
Study population
Derivation cohort
The derivation cohort included consecutive patients with TS prospectively identified from three coronary care units in the public hospitals in the Auckland region (Middlemore Hospital, Auckland City Hospital and North Shore Hospital) between March 2004 and July 2015, and consecutive female NSTEMI patients who underwent both coronary angiography and echocardiography, from the same hospitals, between January 2014 and January 2015. There were 220 patients identified who fulfilled the InterTAK Diagnostic Criteria for TS.14 All patients had LV assessment by either echocardiography or left ventriculography at the time of their coronary angiography. Nine men, 4% of the cohort, were excluded. Of the remaining women, 73 were excluded because they had ST elevation on the admission ECG and 38 had either left bundle branch block or a paced rhythm. This left 100 consecutive NSTE-TS women, who were compared with 100 consecutive women presenting with NSTEMI (using the Third Universal Definition of Myocardial Infarction).15 Patients with a clinical and/or cardiac MRI diagnosis of myocarditis were excluded.
Validation cohort
After development of the TS score in the derivation cohort, a temporal validation cohort was acquired comprising consecutive women presenting with NSTEMI or NSTE-TS to one of the study hospitals (Middlemore) between February 2015 and January 2016. Diagnoses were made using the same criteria used for the derivation cohort. The TS score was not available to the clinicians caring for the patients.
Data items and definitions
Clinical variables
Age, smoking status and history of hypertension, dyslipidaemia, diabetes mellitus (DM) and prior cardiovascular disease (CVD) were obtained at the time of the index admission. For each patient, clinical staff made specific enquiry regarding possible stressors, where a stressful trigger was defined as an unusual emotional or physical stress occurring before symptom onset. The individual physical and emotional stressors identified in the derivation cohort are shown in online supplementary appendix table 1.
Supplemental material
ECG variables
A standard 12-lead ECG was obtained at admission and on the next day (day 1 ECG). All ECGs were recorded at a paper speed of 25 mm/s with a 10 mm/mV amplification. TWI was defined as negative T-waves>0.5 mm in amplitude, and the number of leads meeting criteria for TWI was recorded. Patients were dichotomised into those with or without TWI in ≥6 leads. ST depression was determined by measuring the vertical distance between the patient’s trace and the isoelectric line at a location 2–3 mm from the QRS complex and was considered significant if it was more than 1 mm in V5-V6, or 1.5 mm in aVF or III. ECG analysis was performed blinded to patient diagnosis.
Statistical analysis
Descriptive statistics for continuous variables were summarised as mean and SD. Categorical data are reported by frequency and percentage. For continuous variables, comparisons between groups were performed by the two sample Student’s t-test. For categorical variables, X2 or Fisher’s exact tests were used as appropriate. Our prior work demonstrated that ECG changes late after admission best distinguished the two conditions.13 Consequently, the score was developed using ECG data available on day 1 post-admission. Variables were initially considered for inclusion based on a priori assessment of their likely discriminative value. The ECG variables included were based on the prior published work.13 In that study, evolving TWI was a better discriminator than progressive QTc interval prolongation and was therefore chosen for use in this score. Variables were included in the final score if they were significant univariate predictors at the p<0.01 level. Multivariable logistic regression was performed to distinguish women with NSTEMI from those with NSTE-TS within the derivation cohort using the following variables: diabetes, stress, prior CVD, TWI in ≥6 leads and presence of ST-segment depression in any lead. The regression coefficients were then scaled and rounded to provide weights for each variable in an additive score.
The ability of the score to discriminate between NSTE-TS and NSTEMI patients on day 1 postadmission was assessed using receiver operating characteristic curve analysis, reporting the area under the curve (AUC) and associated 95% CI. An optimal cut-off was defined by the Youden index16 and was checked visually by examining the distribution of scores. Sensitivity, specificity, positive and negative predictive values of the score to distinguish NSTE-TS from NSTEMI were reported. The score and cut-off were developed and assessed using ECG data obtained on day 1 postadmission, and assessed using ECG data obtained on the day of admission for the same cohort. Other variables were unchanged. The score was then assessed in the prospectively acquired temporal validation cohort of women (NSTE-TS, n=40; NSTEMI, n=70). Calibration performance of the day 1 postadmission score in the validation cohort was assessed graphically by categorising patients into deciles of predicted probability of having TS and plotting the mean probability for each post-admission against the observed probability. The slope and intercept obtained by regressing observed against predicted probabilities and the 95% CI of the slope term, are reported.
Interobserver variability for the ECG criteria was also assessed. Two of the coauthors (J-LL and JG) independently read the ECGs in the validation cohort. The agreement regarding TWI in >6 leads was assessed using a kappa statistic, based on the classification of Landis and Kock.17 The interobserver variability on the ECG criteria analysis was very good (kappa coefficient 0.81).
Data were analysed using SAS statistical package, V.9.4 (SAS).
Results
Clinical characteristics
Table 1 summarises the clinical characteristics of the derivation cohort. In comparison to women with NSTE-TS, those with NSTEMI were more likely to have hypertension, diabetes and prior CVD. A stressful trigger was identified in 70% of women with NSTE-TS but only 15% of women with NSTEMI (p<0.0001). Widespread TWI ≥6 leads was present in 14% of NSTE-TS patients at admission and increased to 57% by day 1. No NSTEMI patient had widespread TWI at admission and only 10% did on day 1. In contrast, ST depression occurred in 28% of NSTEMI at admission and 11% on day 1, but was infrequent in NSTE-TS patients.
Clinical characteristics of patients in the derivation and validation cohorts
Clinical score derivation and performance
The score included five parameters which met the predefined criteria for inclusion (table 2). Each variable was given a weight based on its associated coefficient in the logistic regression model as follows: TWI in ≥6 leads (3 points), stress (2 points), diabetes (−1 point), prior CVD (−2 points) and presence of ST depression (−3 points). The score for an individual patient is obtained by adding up the points allocated to each of their five risk factors. The resulting score can therefore range from −6 to +5.
Multivariable logistic regression model to distinguish NSTE-TS from NSTEMI and final score weights
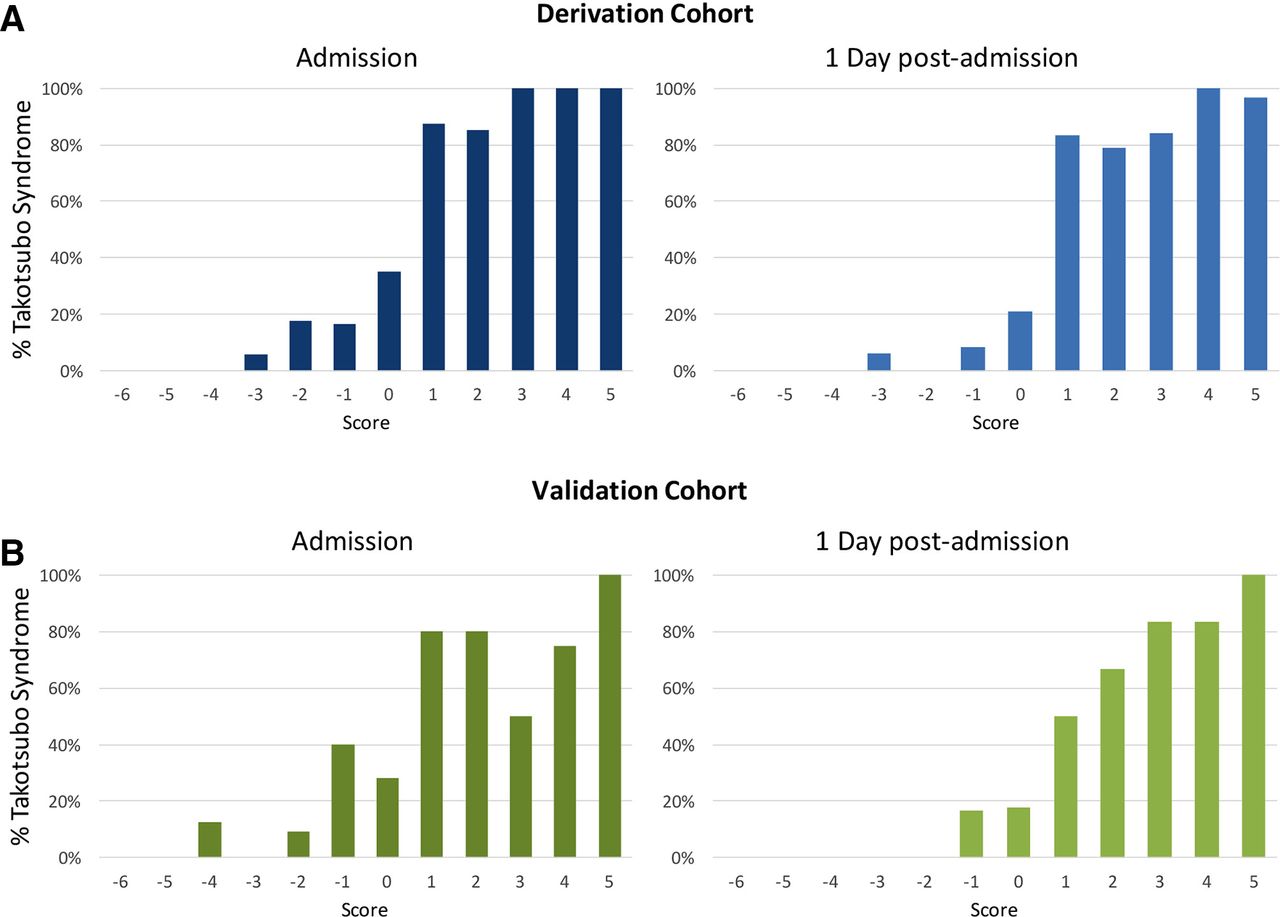
The relationship between the arithmetic NSTE-TS risk score and the predicted probability of TS using the multivariable logistic regression model is shown in figure 1. Translating this to the percentage of patients with NSTE-TS for each value of the TS score confirms the sigmoid relationship, which was consistent whether calculated using ECG data from the day of admission or day 1 post-admission, (figure 2A).
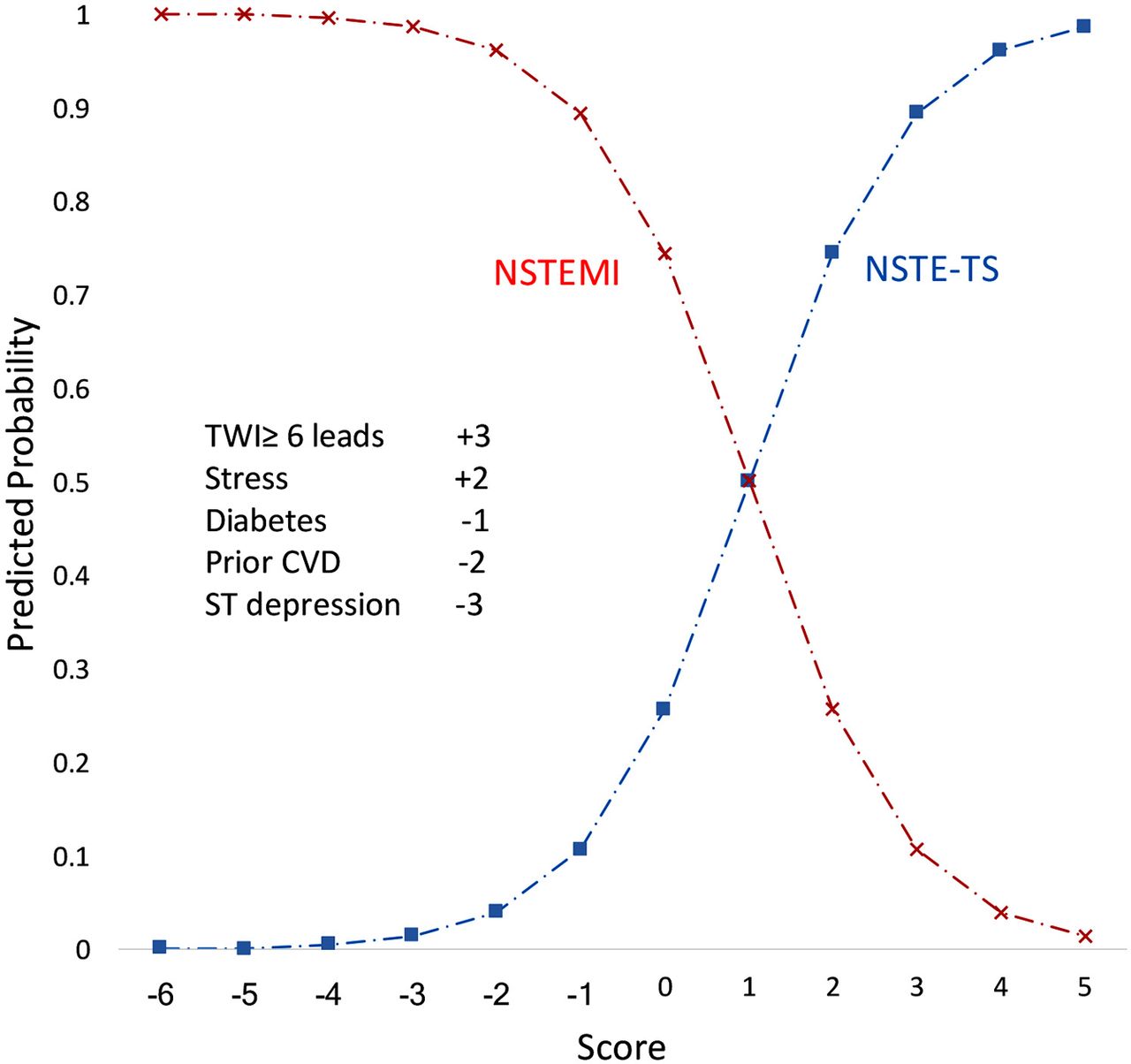
The relationship between the arithmetic NSTE-TS risk score and the predicted probability of TS on day 1 post-admission using the multiple logistic regression model (blue squares). The five variables and corresponding weights comprising the arithmetic score are displayed in the box. The score for an individual patient is obtained by adding up the points allocated to each of their five risk factors. For example, a patient who presented with “stress” (+2), who has T-wave inversion in six leads on the day 1 ECG (+3) and diabetes (−1), but who does not have ST depression on the day 1 ECG (0), diabetes (0) or CVD (0) has a NSTE-TS score of +4 and therefore has a predicted probability of TS of over 90%. The predicted probability of an NSTEMI (red crosses) is given by one minus the predicted probability of TS for each level of the TS score. CVD, cardiovascular disease; NSTEMI, non-ST segment elevation myocardial infarction; NSTE-TS, Takotsubo syndrome with non-ST-segment elevation; TS, takotsubo syndrome; TWI, T-wave inversion.
{kind=link}
{kind=link}
The percentage of patients diagnosed with NSTE-TS by the risk score calculated using ECG values recorded at admission (left panels) and recorded on day 1 post-admission (right panels), shown for the (A) derivation and (B) validation cohorts. NSTE-TS, Takotsubo syndrome with non-ST-segment elevation.
Using ECG data from day 1 post-admission (figure 2A), the median score for NSTEMI patients was −1 (IQR −3 to 0) compared with a median score of 2 (IQR 0– 2) in NSTE-TS patients. The AUC was 0.91 (95% CI 0.87 to 0.95) and the optimal cut-off for distinguishing NSTE-TS and NSTEMI identified by the Youden index was a score of 0.1. Above this cut-off (≥1), the score had a sensitivity of 88% and a specificity of 83% in predicting NSTE-TS, although in the cohort and time point used to derive the score.
When ECG values were replaced with those obtained at admission, the AUC was 0.87 (95% CI 0.83 to 0.92), with sensitivity of 73% and a specificity of 90%.
Validation
In the prospective, consecutively identified, validation cohort, there were 40 patients with NSTE-TS and 70 with NSTEMI (table 1). A NSTE-TS score ≥1 was more likely to correspond to a NSTE-TS than an NSTEMI diagnosis (figure 2B).
The performance of the score using ECG data on admission was very good, with an AUC of 0.82 (95% CI 0.75 to 0.90). The sensitivity and specificity of a score ≥1 to distinguish NSTE-TS from NSTEMI were 63% and 90%, with positive and negative predictive values of 78% and 81%, respectively.
The performance of the score using ECG values on day 1 postadmission was excellent with an AUC of 0.92 (95% CI 0.87 to 0.97). The sensitivity and specificity of a score ≥1 to distinguish NSTE-TS from NSTEMI were 85% and 86%, with positive and negative predictive values of 77% and 91%, respectively. The slope of the calibration line plotting the predicted versus observed probabilities of TS on day 1 post-admission was 0.96 (95% CI 0.60 to 1.32) and intercept is 0.02, indicating excellent calibration (see online supplementary figure).
Supplemental material
Discussion
This study derives and temporally validates a simple five-variable clinical score that can be used at the bedside to distinguish women with NSTE-TS from those with NSTEMI. The score was developed using ECG data available on the post-admission ward round on the day post-admission because prior work found that evolving ECG changes best distinguish these conditions later after admission. In the validation cohort, the score had excellent discrimination performance when applied on the first day after admission, and still performed well when applied to patients at admission. The ratio of women with NSTE-TS to NSTEMI was high (40:70) in the validation cohort, consistent with this being a more frequent diagnosis in these patients than previously described. The relatively high incidence of NSTE-TS combined with the good sensitivity and specificity of the score to differentiate between the two conditions resulted in very good positive and negative predictive values, which are the most important parameters when applying a score in routine clinical practice. In this cohort, a cut-off score of ≥1 at admission correctly identified 78% of women with NSTE-TS and a score of <1 identified 81% of those with NSTEMI. When applied on the day after admission, the corresponding values were 77% and 91%, respectively.
Score logic
Our clinical score comprises five clinical parameters, which can be easily obtained at the evaluation of women with suspected NSTE-TS. Prior reports have demonstrated that patients with TS are more likely to present after an acute stressful event18 than NSTEMI patients, and to develop characteristic ECG changes.13 19 These variables were positively weighted in the final score. Unlike TS, NSTEMI commonly occurs in patients with known CVD or with atherosclerotic risk factors,20–23 which is consistent with the negative weightings assigned to prior CVD, DM and ST depression in the final score. The more positive the score, the more likely the patient is to have TS, and the more negative the more likely it is to be NSTEMI. Because the most useful ECG feature, TWI, takes time to evolve, the score was derived using day 1 ECG data, and was best at distinguishing the two conditions on the day post-admission.
Clinical implementation
This score was designed to be used as part of a clinical diagnostic pathway. At initial presentation, approximately one-third of patients with TS have ST elevation and are usually managed via an acute reperfusion pathway with rapid coronary and LV imaging to distinguish TS from STEMI. Of the remaining two-thirds of patients with TS, very few are men. The score was, therefore, developed for use in women. In our validation cohort, the cut-off score that had been identified in the derivation cohort performed at a level which we consider to be clinically useful.
An NSTE-TS score of >1, either at admission or on the next day, should strongly raise the clinical suspicion of TS. The score performs slightly better on the day postadmission, with better specificity due to the greater sensitivity and specificity of the ECG criteria post-admission.
Comparison with other scores
The InterTAK diagnostic score, the only other TS score that we are aware of, uses a multivariable model to differentiate TS from ACS at admission in both men and women.4 Given the overwhelming female representation in the TS compared with ACS cohorts (95% vs 24%, respectively), female gender was unsurprisingly the single strongest predictor in their model. They also included all ACS subtypes with over half of their patients having STEMI. Therefore, only around 10% of their ACS cohort were women with NSTEMI, the group we sought to differentiate from TS using our score. While the InterTAK score performed well in their derivation and validation cohorts, it remains to be determined how well it would perform in distinguishing women with NSTE-TS from those with NSTEMI—the subgroup in which would be most clinically useful. Templin et al1 recently reported a higher prevalence of neurologic or psychiatric disorders in patients with TS, with 42% having a diagnosis of a psychiatric illness, of which half were identified as affective disorders. Others have also found an increased prevalence of premorbid psychiatric diagnoses, particularly anxiety disorders, in patients with TS.24 An advantage of the InterTAK score is the inclusion of psychological variables, which were unavailable to us. Inclusion of these variables into our model in the future may improve performance, particularly at admission, when ECG changes are less discriminatory.
Incidence of TS and ACS in women
A third of our temporal validation cohort had TS. This seems high compared with older reports of all-comer ACS cohorts which report a TS incidence of 1%–2.5%.25 However, it is likely that TS has often been under-recognised in the past. The InterTAK investigators quote an overall incidence of 4.1% in Zurich hospitals,4 and the incidence of TS in women with ACS has been found to be 5.9%–7.5%.26 Women typically comprise forty percent of all ACS admissions.27 If you consider that virtually all TS events occur in women, the true incidence of TS among women in the Zurich cohort may approach 10%–15%. Because our unit has had an active interest in TS for many years and maintains a prospective registry, it is likely that very few TS diagnoses are missed, contributing to the high observed incidence in the sample used as the validation cohort.
Clinical implications
Our score can be easily calculated on admission and on the postacute ward round, and may be helpful in planning the initial evaluation of women who present with suspected ACS. In patients where TS is suspected, early echocardiography should be performed to identify the typical symmetric wall motion abnormalities.28 In women with NSTE-TS scores >1, particularly those with typical echocardiogram appearances, it may be reasonable to undertake CT rather than invasive coronary angiography to assess atherosclerotic coronary artery disease.29 Early echocardiography to make the diagnosis is important as the typical LV dysfunction can recover quickly.1 30 Echocardiography also allows detection of LV outflow tract obstruction and mitral regurgitation due to systolic anterior motion of the mitral leaflet, both of which can complicate the management of TS.31 32
Limitations
A common feature of TS is preceding emotional or physical stress. We included stressors as part of the clinical score but did not divide these into physical and emotional triggers, which have different weights in the InterTAK score. As previously discussed, we were not able to include neurological or psychiatric disorders as part of the clinical scoring system. However, these conditions may be difficult to categorically define. There are other ECG features which might help to distinguish the two conditions and more sophisticated ECG analysis might allow the score to be improved. One additional candidate variable is the evolution of QTc prolongation. We chose not to include this variable because it was not as good as TWI in discriminating between NSTE-TS and NSTEMI in prior analyses.13 In addition, our aim was to develop a score that could be easily utilised at the bedside; a comparison between QTc intervals recorded on serial ECGs may be more difficult to reliably measure at the bedside. The score has less clinical utility when a coronary angiogram has already been performed. However, in current clinical practice few suspected patients with ACS at admission without ST-elevation require routine immediate invasive coronary angiography, and the score may, therefore, help guide the cardiac imaging strategy in the remaining patients, either at admission, or on the postacute ward round. Patients with ACS at high risk based on their Global Registry of Acute Coronary Events (GRACE) risk score are recommended to have angiography within 24 hours.33 In New Zealand, approximately one-third of patients with ACS have a high GRACE risk.34 In those patients, the TS score may need to be used with caution as predictive value was greatest on the postacute day. The validation cohort was collected prospectively with consecutive patients with ACS and TS over a year. Nevertheless, it is possible that the proportion of patients with TS in this cohort was higher than it would be over the longer run due to the play of chance, and that differences in population characteristics may also lead to varying incidence of TS. If the incidence in a population was lower, this would result in correspondingly lower positive and negative predictive values for the score.
Conclusion
This NSTE-TS score is easy to use at the bedside and may prove useful in clinical practice to distinguish women with NSTE-TS from those with NSTEMI. The score performs best when applied on day 1 after admission, but can also usefully distinguish between the conditions at admission. Further validation in external cohorts is needed.
References
Footnotes
Contributors J-LL, MW, AT and AJK are involved in the design of this study. J-LL, KP and AJK are involved in drafting and revision of the manuscript. KP and ML are involved in the statistics section. JG is involved in data collection and interobserver variability for the ECG criteria.
Funding ML is supported by the Middlemore Hospital Cardiac Trust. KP is supported by the Heart Foundation Hynds Senior Fellowship. AJK receives salary support from the NZ Health Research Council.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The study was approved by the New Zealand Health and Disability Ethics Committees as observational research (Research Registration Number: 1763).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement No data are available.