Article Text

Abstract
Objective Social determinants of health (SDH) have previously demonstrated to be important risk factors in determining health outcomes. To document whether the SDH are associated with hospitalisations for ischaemic stroke.
Methods This cross-sectional study examines data from fiscal year 2015. Patients from the national Medicare 100% Inpatient Limited Dataset were linked with SDH measures from the Robert Wood Johnson Foundation (RWJF) County Health Rankings. Medicare patients were included in the study group if they had either an admitting or primary diagnosis of ischaemic stroke. Counties without RWJF data were excluded from the study. Ischaemic strokes were compared with all other hospitalisations associated with characteristics of the SDH measures and benchmarked to above or below their respective national median. Estimates were performed with nested logistic regression.
Results Approximately 256 766 Medicare patients had ischaemic stroke hospitalisations compared with all other Medicare patients (n=6 386 180) without ischaemic stroke hospitalisations while 30 853 patients were excluded due to residence in US territories. Significant factors included air pollution exceeding the national median (OR 1.06; 95% CI 1.05 to 1.07), per cent of children in single parent households exceeding the national median, (OR 1.02; 95% CI 1.01 to 1.03), violent crime rates exceeding the national median, (OR 1.02; 95% CI 1.01 to 1.03) and per cent smoking exceeding the national median, (OR 1.02; 95% CI 1.01 to 1.03).
Conclusions When cross-sectional SDH are benchmarked to national median for ischaemic stroke hospitalisations and compared with all-cause hospitalisations, the effects remain significant. Further research on the longitudinal effects of the SDH and cardiovascular health, particularly disease-specific outcomes, is needed.
- stroke
- public health
- epidemiology
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known about this subject?
Various factors of the social determinants of health influence ischaemic stroke outcomes.
What does this study add?
This study fulfils a gap in knowledge of the effects of a group of measures representative of the social determinants on ischaemic stroke hospitalisations.
How might this impact on clinical practice?
Clinical practice will consider incorporating the social determinants in the prevention, screening, diagnosis and treatment of ischaemic strokes.
Introduction
Many biological and sociological factors have been attributed to cardiovascular health.1 A large number of these factors are considered the social determinants of health (SDH) and have been shown to predict health outcomes.2 According to the American College of Physicians, the SDH encompass six key domains: economic stability, neighbourhood and physical environment, education, community and social context, food and health.3 Subsequently, these factors have also been associated with care utilisation such as increased odds of hospitalisations, readmissions and utilisation of emergency department services.4 5
The effect of the SDH on individual health is framed in a conceptual logic that the longitudinal influence of community-level factors is highly likely to impact an individual’s health through environmental, mental conditional, nutrition, and other indirect and direct mechanisms, occurring over time—a longitudinal impact. Since the majority of available individual data (linked to outcomes) are cross-sectional, the SDH contextual data associated with these individual-specific data are most likely to be community-level aggregate characteristics and cross-sectional. Documenting the relationships of these community-based descriptors with cross-sectional outcomes of large populations will develop a body of important related evidence that can be useful for intervention design, planning and implementation. Since true longitudinal data of exposures to the SDH are beyond the realm of reasonable data collection in the USA, such cross-sectional associations are a reasonable substitute. A growing body of literature is incrementally clarifying the influence of the SDH in specific clinical and disease conditions.
Within the field of cardiovascular health, the American Heart Association (AHA) has highlighted the SDH as a major risk factor of cardiovascular disease. Studies have showed that socioeconomic status (SES), an element of the SDH, has been shown to be associated with cardiovascular disease presented by a review.6 More specifically, social factors, such as education, employment and income, have a significant relationship with cardiovascular disease outcomes.7 In addition, environmental factors, such as air pollution, have been considered risk factors of cardiovascular disease and stroke admissions.8 Food insecurity also has had a negative impact on cardiovascular health.9 However, currently, there has been an absence of studies exploring the association of all aspects of the SDH and cardiovascular health, with recent work solely focused on psychological factors as the SDH.10
In this study, we explored the relationship between the SDH and ischaemic strokes, using data previously used in examining ocular hospitalisations among Medicare beneficiaries in a national Medicare inpatient file linked with community health measures from the Robert Wood Johnson Foundation.11–15 The primary aim of this study was to illustrate the geographical variability of Medicare ischaemic stroke hospitalisations rates and subsequently to examine the association of select SDH on these hospitalisations. In this study, we considered the importance of the SDH in ischaemic stroke hospitalisations compared with all-cause hospitalisations.
Methods
We conducted a cross-sectional study using fiscal year 2015 data from the national Medicare 100% Inpatient Limited Dataset (LDS), merged with the 2015 Robert Wood Johnson Foundation (RWJF) County Health Rankings.16 17 This study abides by the Dataset Use Agreement (DUA) with a study exemption from Northwestern University Institutional Review Board. With the national Medicare Inpatient LDS, we identified patients who had either an admitting diagnosis or a principal diagnosis of an ischaemic stroke using ICD-9 codes 434.
The RWJF County Health Rankings are publicly available data (annually from 2011 to 2019) with 35 health measures incorporated into health rankings for almost every US county (3191 counties). Counties without RWJF data were excluded from the study. Each county’s health measure was characterised by data provided by the National Center for Health Statistics, Center Disease Control’s Behavioral Risk Factor Surveillance System, the American Community Survey and the US Department of Agriculture Food Environment Atlas.
Using Medicare LDS and the RWJ data, we linked individuals with their county health measure by combining Medicare’s LDS two-digit state and three-digit county codes to create the Social Security Administration’s (SSA) five-digit code. The RWJF datasets contain a Federal Information Processing Standards (FIPS) code, which is a combination of state and county codes, distinct from Medicare’s 5-digit SSA code, and thereby requires a cross-walk in merging the two datasets. Using the National Bureau of Economic Research data, we cross-referenced the SSA codes to FIPS codes and then merged them with the RWJF rankings data. Among all 6 673 799 Medicare patients, 30 853 patients were excluded due to residence of care received in US territories. Within the data, there were 256 766 patients with ischaemic stroke compared with all other patients without strokes (n=6 386 180). The key covariates adjusted in the Medicare datasets were patient-specific variables, age, gender and race.
We used the RWJF data to create characteristics at the county level that captured the six key domains of the SDH (economic stability, neighbourhood and physical environment, education status, food access, social and community context, healthcare). Variable selection for each domain was based from the literature and was selected from measures in the RWJF Community Health Rankings.18 To facilitate interpretation and discussion, we converted RWJF measures to binary variables, where ‘1’ represents a county above the national median for a selected measure and ‘0’ represents counties below the national median.
Across all six domains of the SDH, we used standardised measures published by Healthy People 2020 to ensure representation among each domain of the SDH for analysis.19 For economic stability, we used unemployment as a measure of the economic health of a community.20 For neighbourhood and physical environment, we included measures of air pollution and housing problems because of their association with residential isolation and poor environments in relation to health.21 We used high school education as a measure of education and has been previously associated with cardiovascular disease health outcomes.22 Food access was measured by food insecurity, as this measure has been associated with chronic disease and poor health.23 Social and community context was captured by single-parent households and volume of violent crime, as these have been linked to less social cohesion and poor cardiovascular health.24 25 Lastly, we accounted for healthcare with measures of rates of diabetes, smoking status, drug poisoning deaths and sexually transmitted diseases because these measures have been used to measure the access to healthcare and the health status of a community.26–28
For the analysis, we performed nested logistic regression using Proc Gen Mod in SAS. Patients with ischaemic strokes were converted to a binary measure of ‘1’ compared with those hospitalised but without ischaemic strokes, ‘0’. To capture the impact of the social determinant on patient hospitalisations, we nested Medicare patients in their respective counties to account for the potential effects of community-level characteristics and capture specific patient characteristics such as age, gender and race.
As a secondary analysis, we examined regional variation of ischaemic strokes among Medicare beneficiaries expressed as a rate per 10 000 using a national map at the county level, adjusted with US Census data. The data management and statistical analysis were conducted in SAS, V.9.4, and the map was developed using ArcGIS, V.10.5.1 Esri.
Results
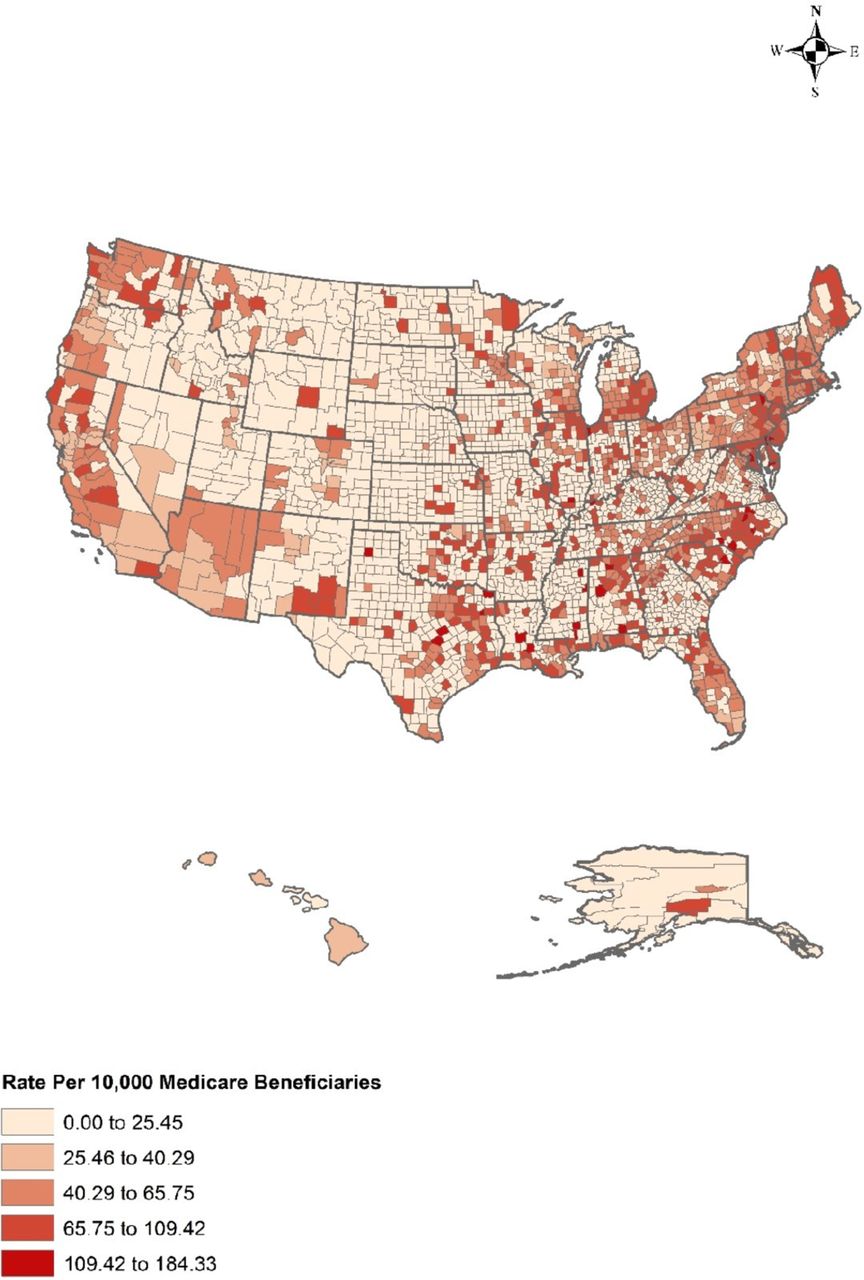
Among the 3191 counties in the USA, almost 96.6% has had at least one ischaemic stroke in 2015. In figure 1, the highest rates of hospitalisations were concentrated in the regions of the Northeast and Mid-Atlantic and in the states of North and South Carolina, Florida, Alabama, Michigan, Washington and California. Significant clustering of higher rates of ischaemic stroke hospitalisations also occurred around major urban areas and cities across the country.
{kind=link}
Regional variation in ischaemic strokes per 10 000 Medicare beneficiaries in 2015.
Table 1 presents 25 counties with the highest rate of stroke and select categories of the 2019 RWJF rankings. Overall, counties with the high rates of ischaemic strokes had poor rankings for health outcomes, health behaviours, socioeconomic and physical environment. For instance, Lynchburg City, Virginia, had the highest rate of Medicare ischaemic stroke hospitalisations at 184.33 per 10 000 with a health behaviour and physical environment ranking near the last quartile of all counties within the state. In general, counties listed in table 1 ranked at the bottom of the states on nearly all measures of the SDH.
Top 25 highest ischaemic stroke rates by county and select categories of the Robert Wood Johnson Foundation’s health rankings in 2019*†
Table 2 presents the main results of the nested logistic regression model at the county level, along with a description of the original data sources of key covariates, median estimates, ORs and corresponding 95% CI estimates. When we considered the SDH and compared them to the national median and compared with all-cause hospitalisation, the effects remain significant. For Medicare beneficiaries, the variables of youngest age and black race (OR 1.50; 95% CI 1.48 to 1.51) were significantly associated with ischaemic stroke hospitalisations while being female was negatively associated. The oldest age group among Medicare beneficiaries (older than 84 years) was 276% more likely to be hospitalised relative to those in the youngest (under 64 years) age group (OR 2.76; 95% CI 2.72 to 2.80). However, it should be noted that the youngest Medicare beneficiaries typically qualify for coverage because of end-stage renal disease or other medical disability.
County-level nested fixed effects model of Medicare ischaemic stroke hospitalisations on SDH (256 766 ischaemic stroke patients to 6 410 299 hospitalised non-stroke patients)
In assessing communities where Medicare beneficiaries with inpatient hospitalisations reside, we found that physical environment, economic, social and community, and health and disease measures were predictive of ischaemic hospitalisations, while housing problems and food insecurity were not. First, communities with air pollution exceeding the national median of 11.62 µg/m³ had a marginal significant association with ischaemic stroke hospitalisations (OR 1.06; 95% CI 1.05 to 1.07). Unemployment had a slightly significant effect on ischaemic strokes (OR 1.01; 95% CI 1.01 to 1.02). In contrast, communities with a higher high school graduation rate were significantly and positively associated (OR 1.03; 95% CI 1.02 to 1.04).
Among communities where the per cent of children in single parent households exceeded the national median of 32.12%, these locations were significantly and positively associated with ischaemic stroke hospitalisations (OR 1.02; 95% CI 1.01 to 1.03). This association was the same for those in communities where the violent crime rate exceeded the national median of 250.4 per 100 000 (OR 1.02; 95% CI 1.01 to 1.03). In the last SDH category of health and disease, those in communities with smoking rates greater than the national median of 21.23% were also significantly associated with ischaemic stroke hospitalisations (OR 1.02: 95% CI 1.01 to 1.03).
Discussion
This is the first study to examine the relationship between SDH derived from RWJF measures and ischaemic strokes. We showed regional variation in ischaemic stroke hospitalisations among Medicare recipients including the region known as the ‘stroke belt’ or southeastern USA, with higher rates of hospitalisations and lower health rankings. Although ischaemic stroke hospitalisation rates were high throughout the USA, there were substantial clustering of higher rates at metropolitan areas and major cities. This phenomenon may be due to the availability of tertiary care facilities in urban areas. Further research is necessary to examine how population density, availability of primary care providers and cardiologists and tertiary healthcare facilities influence ischaemic stroke hospitalisations among various insured and uninsured groups.
The study of the SDH continues to develop in health services research and has been understood as a major longitudinal factor in the studies of cardiovascular disease.29 However, inclusion of social determinants’ data and their influence on cardiovascular health has been limited.30 Our study found significant associations between ischaemic stroke hospitalisations and several domains of the SDH, namely physical environment, economic, social and community context, and health. However, these results were importantly considered in context of the national median. Hospitalisations for ischaemic stroke are only one condition among many other cardiovascular conditions. Policy-makers may find this information useful when implementing value-based care for underserved regions with limited resources.31 For instance, understanding which factors impact ischaemic stroke are important for the development and implementation of interventions that may lead to better prevention of this health condition or tertiary treatment centres.
The strengths of this study were the inclusion of all Medicare inpatient beneficiaries across the USA and use of at least one measure for each of the six SDH domains. The limitations of this study’s design include the potential variation at the county and individual level for SDH factors, attributed to individual outcomes at the county level, and the inability to incorporate the issues of multicollinearity among the SDH variables. Although this study does not unwind the complex interactions between the different components of the SDH, it provides insight into the direct relationships between these factors and ischaemic strokes. The development of an index measure of the SDH may provide a better understanding of its complex interactions with ischaemic stroke outcomes. For instance, a recent study has used a single neighbourhood deprivation index to examine socioeconomic factors to show an increased association of heart failure among deprived neighbourhoods, but lacked inclusion of many components of the SDH and was limited to 1 year of data.32 Since our study focused solely on the Medicare population, it is not generalisable to other populations groups and does not account for multiple counts of hospitalisations at multiple hospitals due to triage. Lastly, our study reported associations between the SDH factors and ischaemic stroke conditions but our results do not reflect causality.
Conclusion
Counties with high rates of Medicare hospitalisation for ischaemic strokes had lower RWJF rankings for health outcomes, health behaviours, socioeconomic and physical environment. When the SDH are benchmarked to the national median for ischaemic stroke hospitalisations and compared with all-cause hospitalisations, the effects remain significant. Further research on social determinants and cardiovascular health, particularly disease-specific outcomes, is needed.
References
Footnotes
Contributors AW, ANK and DDF planned the design of the study. AW and DDF collected and analysed the data. AW, ANK and DDF contributed to data analysis and interpretation. AW, ANK and DDF draft the manuscript and all authors critically revised the manuscript and contributed to the final version.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data may be obtained from a third party and are not publicly available.