Article Text

Abstract
Objective The role of transoesophageal echocardiography (TOE) in identifying ischaemic stroke aetiology is debated. In 2018, the American Heart Association/American Stroke Association (AHA/ASA) issued class IIa recommendation for echocardiography, with the qualifying statement of use in cases where it will alter management. Hence, we sought to determine the rate at which TOE findings altered management in cases of confirmed ischaemic stroke.
Methods We retrospectively analysed TOE cases with confirmed ischaemic stroke at our centre between April 2015 and February 2017. We defined a change in management as the initiation of anticoagulation therapy, antibiotic therapy or patent foramen ovale closure as a direct result of TOE findings.
Results There were 185 patients included in this analysis; 19 (10%) experienced a change in management. However, only 7 of the 19 (4% of all subjects) experienced a change in management due to TOE findings. The remaining 12 were initiated on oral antigoagulation as a result of discoveries during routine workup, mainly atrial fibrillation on telemetry monitoring.
Conclusions This work suggests an overuse of TOE and provides support for the 2018 AHA/ASA stroke guidelines, which recommend against the routine use of echocardiography in the work up of cerebrovascular accident due to a cardioembolic source.
- stroke
- echocardiography
- transoesophageal
- anticoagulation
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known about this subject?
To determine a stroke’s aetiology, transoesophageal echocardiography (TOE) may be used if a cardioembolic source is suspected; however, the benefit of TOE over other procedures is debated and comes with additional risks. In 2018, the American Heart Association/American Stroke Association (AHA/ASA) issued a class IIa recommendation for the use of echocardiography for cases in which it will alter management.
What does this study add?
This study revealed that of 185 subjects hospitalised with confirmed acute ischaemic stroke (AIS) who underwent a TOE, only 4% experienced a change in management as a result of TOE.
How might this impact on clinical practice?
This low rate of medical management alteration due to TOE findings provides support for the 2018 AHA/ASA stroke guidelines. Given that AIS aetiology is often discovered via less invasive technologies, the use of TOE must be used in the appropriate clinical setting, likely after a thorough neurological workup has been performed. Limiting the use of TOE may reduce cost, limit exposure to unnecessary testing and potentially facilitate earlier discharge for patients.
Introduction
Ischaemic and haemorrhagic stroke remain the fifth leading cause of death in the USA, accounting for 1 in every 19 deaths.1 Every year in the USA, over 795 000 patients experience their first stroke, with an additional 180 000 having a recurrent event.1 Costs associated with treating strokes account for approximately 1.5% of total healthcare spending.2 Of all strokes, 87% are ischaemic, and 15%–40% of those are due to a cardioembolic source.2 To determine a stroke’s aetiology, transoesophageal echocardiography (TOE) may be used if a cardioembolic or cryptogenic source is suspected. However, the benefit of TOE over other procedures (eg, MRI and transthoracic echocardiogram (TTE)), is debated and may come with additional risks including exposure to anaesthesia, prolonged hospital stay and incurred expense. In 2018, the American Heart Association/American Stroke Association (AHA/ASA) issued a class IIa recommendation for the use of echocardiography for cases in which it will alter management.3 As it is our hypothesis that TOE is overused in patients with ischaemic stroke, we sought to identify the rate at which management changes due to TOE in patients hospitalised with acute ischaemic stroke (AIS).
Methods
We performed a retrospective analysis using the Baylor University Medical Center’s Lumedx Apollo database to identify patients with AIS who underwent a TOE for the indication of cerebrovascular accident (CVA) between April 2015 and February 2017. This was accomplished by first limiting cases to TOEs, confirming AIS via imaging and filtering based on indication. We reviewed qualifying patient charts and categorised strokes based on the Trial of Org 10172 in Acute Stroke Treatment (TOAST) classification.4 In short, the TOAST classification system uses clinical features, imaging and laboratory assessments to diagnose five subtypes of ischaemic stroke (large artery atherosclerosis, cardioembolism, small-vessel occlusion, stroke of other determined aetiology and stroke of undetermined aetiology) with probable or possible certainty.4 We additionally abstracted information on patient comorbidities and medications from electronic medical records. We defined a change in management as the initiation of anticoagulation therapy, antibiotic therapy or patent foramen ovale (PFO) closure as a direct result of TOE findings. We calculated the rate of management change for all patients with confirmed AIS who underwent a TOE for CVA. This study was approved by the Baylor Scott & White Research Institute’s Institutional Review Board with a waiver of informed consent. Categorical variables are presented as frequency (percentage) and continuous variables as mean±SD or median (quartile 1, quartile 3), as appropriate. Data management and analyses were performed using SAS V.9.4.
Patient and public involvement
Neither patients nor the public were involved in the design, or conduct, or reporting, or dissemination of this research.
Results
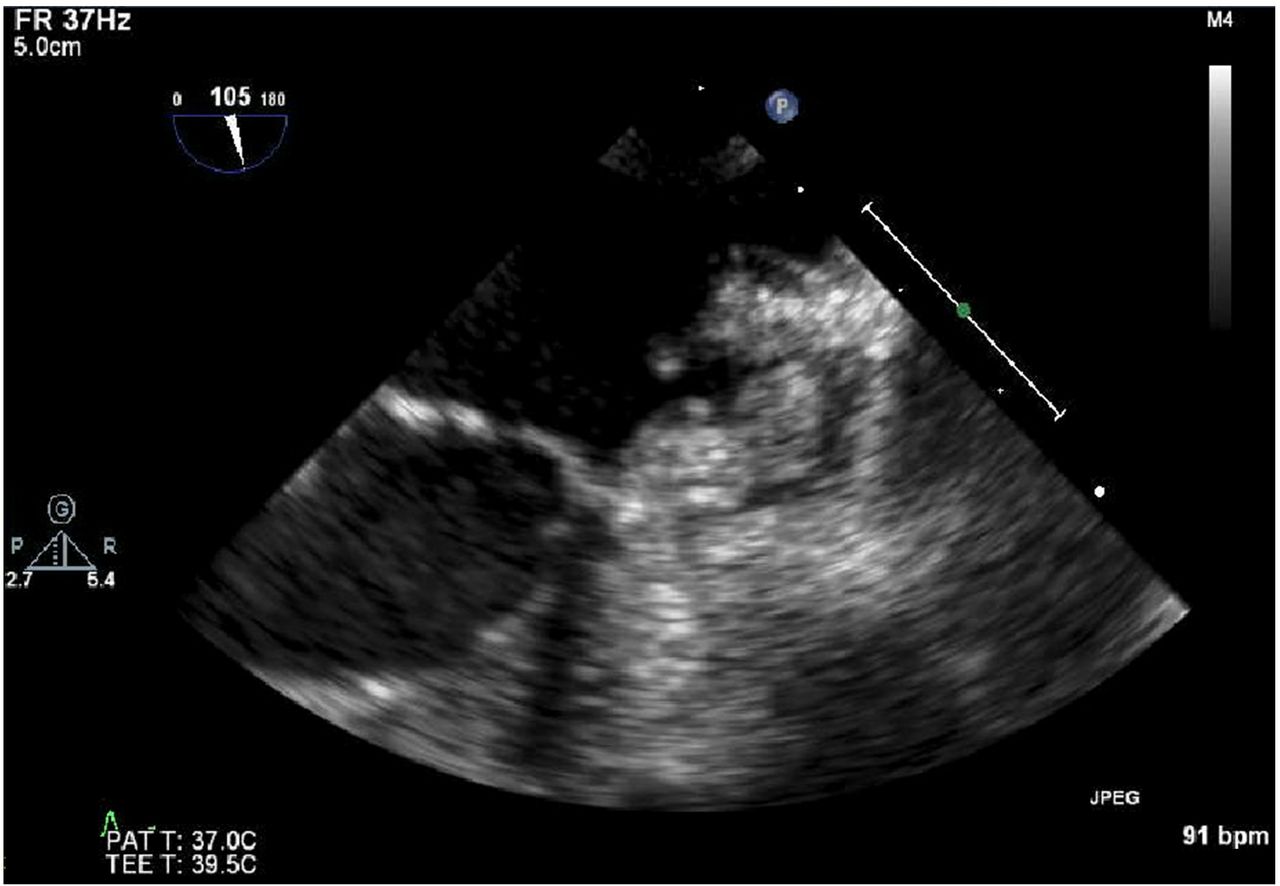
There were 280 patients who underwent a TOE for the indication of ischaemic stroke during the study period; 185 (66%) met this study’s criteria of having a confirmed AIS by imaging and indication of CVA (table 1). Nineteen (10%) patients were initiated on OAC at discharge; however, only 7 of the 19 (37%; 4% of all subjects) actually experienced a change in medical management due to TOE findings (table 2). The remaining 12 were initiated on OAC as a result of discoveries during routine workup, mainly atrial fibrillation on telemetry monitoring. There were two (1%) thrombus cases identified via TOE (figure 1). Interestingly, there were 22 (12%) PFO cases, five (23%) of which were initiated on OAC prior to discharge; however, none were started on OAC for the indication of PFO alone. Closure recommendations are provided by neurologists at our centre; however, no patients with a PFO underwent device closure prior to discharge in this study.

{kind=link}
Large mobile thrombus in the left atrial appendage as detected via transoesophageal echocardiography.
Patient characteristics (n=185)
Transoesophageal echocardiography findings leading to change in management
Discussion
In this study of 185 subjects hospitalised with confirmed AIS who underwent a TOE, only 7 (4%) experienced a change in management, as defined as the initiation of anticoagulation therapy, antibiotic therapy or PFO closure as a direct result of TOE findings. The majority (63%) of patients initiated on OAC were started based on the findings from routine, less invasive and more cost-effective testing such as telemetry, TTE and carotid ultrasound.
As it relates to CVA, TOE is more sensitive to assess for valvular vegetations, left atrial appendage thrombus and PFO than is TTE.5 Multiple studies have investigated the role of TOE in the work up for stroke and have mixed conclusions and recommendations.6–9 In spite of these studies, previous guidelines remained vague with respect to the proper use of TOE, and there are limited observational data showing how TOE findings impact management.10 Furthermore, the rates of TOE findings causing a change in management vary across studies. For example, Pallesen and colleagues and Katsanos and colleagues showed 9% of cases resulted in management change, while Marino and colleagues revealed that, despite having high diagnostic value, TOE findings changed medical management in only 0.4% of cases in their study.11–13 Hence, our result of 4% is intermediary. The AHA/ASA 2018 updated guidelines for AIS deviate from prior iterations by directly addressing cardiac work up in stroke, acknowledging the role of prolonged cardiac monitoring, with a IIb recommendation in ‘select patients’. In addition, and in line with our findings, ‘the routine use of echocardiography in all patients with acute ischaemic stroke to plan subsequent secondary preventive treatment is not cost-effective and is not recommended’.3 The American Society for Echocardiography (ASE) published guidelines in 2011 for the use of echocardiography in the evaluation of cardiac source of embolism. The indications include having a non-diagnostic TTE, evaluating for cardiovascular source of embolus without other non-cardiac source, to assess valvular structure and to diagnose infective endocarditis.5 Significant valvular structural problems that pose a risk for thromboembolic phenomenon should be detectable by TTE. In addition, the diagnosis of infective endocarditis (a separate indication for TOE) should be accompanied by consistent clinical findings. The ASE guidelines state that the use of TOE is ‘inappropriate and not reasonable’ when TOE results would not change management.5
Newer studies have demonstrated increased detection of atrial fibrillation in patients with prolonged monitoring after AIS.14–16 While often clinically suspected, the role of and proper treatment for silent atrial fibrillation has been difficult for physicians to decipher. The absence of left atrial thrombus on TOE does not confer the absence prior to AIS.16 Initiation of OAC therapy without evidence of thrombogenic rhythm is not recommended at this time; hence, increased bleeding risk has justifiably prevented most physicians from initiating OAC. Instead, the focus has been on antiplatelet therapy, which has demonstrated a marginal benefit in reducing subsequent stroke.17–20
This single centre study has notable limitations. In our institution, a TOE is often ordered on admission by a hospitalist (per protocol) or by neurologists as a component of initial stroke work up. It is even occasionally performed prior to a TTE or confirming stroke by imaging due to heavy MRI use among hospitalised patients and its time-consuming nature compared with CT imaging. However, we acknowledge that not all centres operate in the same manner. We could not adequately compare the value of TTE versus TOE, as many patients underwent TOE alone. Additionally, our definition of change in management was limited to the time period of the initial hospitalisation; if a patient was started on OAC, had extended cardiac rhythm monitoring as an outpatient or underwent percutaneous PFO device closure after discharge, those results were not captured in this analysis. Finally, although recent clinical trials indicate that PFO closure in addition to long-term antithrombotic treatment likely reduces the recurrence of stroke in patients aged 60 years or younger such that the benefits outweigh the risks, our study was conducted during a time of more uncertainty about PFO closure outcomes.21
Conclusion
A change in medical management due to TOE findings occurred in only 4% of patients who underwent a TOE for AIS in this study. This low rate provides support for the 2018 AHA/ASA stroke guidelines, which recommend against the routine use of TOE in the work up of AIS. Given that AIS aetiology is often discovered via less invasive technologies, the use of TOE must be used in the appropriate clinical setting, likely after a thorough neurological workup has been performed. Further consideration is needed for prolonged rhythm monitoring for atrial arrhythmias and the initiation of novel oral anticoagulation. Limiting the use of TOE may reduce cost and exposure to unnecessary testing, as well as potentially facilitate earlier discharge for patients.
References
Footnotes
Contributors ZPR contributed to the design, interpretation and draft. KFK, BRM, KMT and AV contributed to data acquisition and critical revision. PAM, PAG and JMS contributed to interpretation and critical revision. All authors approve and agree to be accountable of this work.
Funding This work was partially funded by the Baylor Heath Care System Foundation.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval This retrospective study was approved by the Baylor Scott & White Research Institute’s Institutional Review Board with a waiver of informed consent.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data from this study will not be made available.