Article Text

Abstract
Background ST-segment elevation myocardial infarction (STEMI) outcomes are influenced by the location of the culprit vessel with worse outcomes portended with a left anterior descending (LAD) culprit lesion. However, relatively little is known about the independent association of LAD involvement with clinical outcomes of patients with STEMI with and without out-of-hospital cardiac arrest (OHCA).
Methods We identified 91 patients with and 929 without a preceding OHCA within the Vancouver Coastal Health Authority who presented with an acute STEMI and underwent primary percutaneous coronary intervention between 26 June 2007 and 31 March 2016.
Results Patients with STEMI with OHCA had higher rates of in-hospital cardiac arrest (43.3% vs 8.3%, p<0.001), heart failure (50.5% vs 11.3%, p<0.001), cardiogenic shock (49.5% vs 5.7%, p<0.001), mortality (35.2% vs 3.3%, p<0.001) and reduced left ventricular ejection fraction (LVEF; 42.9% vs 47.3%, p<0.001) compared with those without OHCA. Among patients without OHCA, LAD involvement was associated with increased heart failure (18.1% vs 5.2%, p<0.001), in-hospital cardiac arrest (10.7% vs 6.2%, p<0.014), cardiogenic shock (8.4% vs 3.3%, p<0.001), reduced LVEF (43.0% vs 51.2%, p<0.001) and mortality (5.2% vs 1.3%, p=0.003) compared with patients without LAD involvement. With the exception of LVEF, these associations were not seen among patients with STEMI with OHCA and an LAD culprit. The presence of an LAD culprit was not independently associated with increased hospital mortality among patients with OHCA after adjusting for potential confounding factors.
Conclusion Our study has demonstrated a differential impact of LAD involvement on clinical outcomes among patients with STEMI who present with and without OHCA. Our data highlight the complexity surrounding the prognostication following OHCA complicating STEMI and demonstrate that other mechanisms other than LAD involvement contribute to the high mortality associated with OHCA as a result of STEMI.
- resuscitation
- sudden cardiac death
- coronary artery disease
- coronary intervention (PCI)
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known about this subject?
There are conflicting data with smaller studies examining the impact of angiographic features on outcomes in patients with out-of-hospital cardiac arrest (OHCA). Tofler et al found that there were no differences in long-term mortality of patients presenting with ventricular tachycardia or ventricular fibrillation (VT/VF) compared with those without VT/VF when they were separated into those with anterior ST-segment elevation myocardial infarction (STEMI) or inferior or posterior STEMI. In contrast, a multicentre analysis by Velders et al with 224 patients with STEMI with OHCA described an association between culprit artery and OHCA, with the risk being highest for proximal left coronary lesions.
What does this study add?
Prior to our study, little was known about whether angiographic features (and, in particular, left anterior descending (LAD) involvement) independently conferred higher in-hospital mortality and worse in-hospital outcomes among patients with STEMI with OHCA. Our study is one of the largest studies using contemporary STEMI data evaluating the association of LAD on outcomes among patients with STEMI with and without OHCA. Our data demonstrated that there was no independent association of LAD with mortality among patients with STEMI presenting with OHCA.
Key questions
How might this impact on clinical practice?
Our study highlights the complexity surrounding the prognostication following OHCA while suggesting that mechanisms other than LAD involvement confers a higher mortality and worse hospital outcomes in patients with OHCA following successfully reperfusion with primary percutaneous coronary intervention. Clinicians treating patients with STEMI and OHCA should continue to use management strategies that emphasise early identification of patients with STEMI with OHCA and rapid reperfusion but should also focus on identifying and managing other concomitant high-risk features driving poor outcomes in these patients, such as shock and neurological injury.
Background
Out-of-hospital cardiac arrest (OHCA) remains a significant public health issue associated with high mortality1 2 with an overall survival of only 10% to hospital discharge.3 4 An acute coronary syndrome is a frequent cause of OHCA and rapid access to emergent primary percutaneous coronary intervention (PCI) in OHCA caused by ST-segment elevation myocardial infarction (STEMI) is associated with improved survival.5–7 Current North American and European cardiac arrest and resuscitation guidelines indicate a strong recommendation for angiography and PCI in patients with OHCA with STEMI.8 9
Predictors of poor outcomes in patients with OHCA with STEMI include increased age, delayed cardiopulmonary resuscitation (CPR), initial asystole rhythm, renal insufficiency, delayed time to return of spontaneous circulation (ROSC) and reduced ejection fraction on hospital admission.10 The location of the culprit vessel is also an important clinical predictor of outcomes in STEMI. STEMI due to a left anterior descending (LAD) culprit vessel is associated with worse clinical outcomes due to the extent of myocardial involvement.11–13 An anterior location of a myocardial infarction is an important independent predictor of mortality among patients with STEMI undergoing primary PCI (PPCI).11 14 However, little is known about the independent impact of coronary territory involvement, in particular the LAD, on outcomes acute STEMI associated with OHCA.15–19
Our objective was to describe the characteristics of patients with STEMI who presented with and without OHCA, and to describe any differences in the distribution of an LAD culprit vessel among patients with STEMI with and without OHCA. We also aimed to compare the in-hospital outcomes in patients with STEMI with and without OHCA and outcomes of patients with STEMI with and without OHCA based on the presence of an LAD culprit. The final aim of this study was to determine if there was any independent association between an LAD culprit vessel and in-hospital outcomes among patients with STEMI with and without OHCA.
Methods
Data source
This study was a retrospective analysis of prospectively collected data on consecutive patients with STEMI who presented to a Vancouver Coastal Health Authority (VCHA) hospital between 26 June 2007 and 31 March 2016. The VCHA STEMI database is a quality improvement tool that includes 13 participating hospitals in this region of which two are PCI-capable centres (and perform all the pPCIs in the region), and four are geographically close enough to refer patients with STEMI for pPCI. Patients at the other seven centres would not have been eligible for pPCI due to their distance from the PCI-capable centres.
Patient population
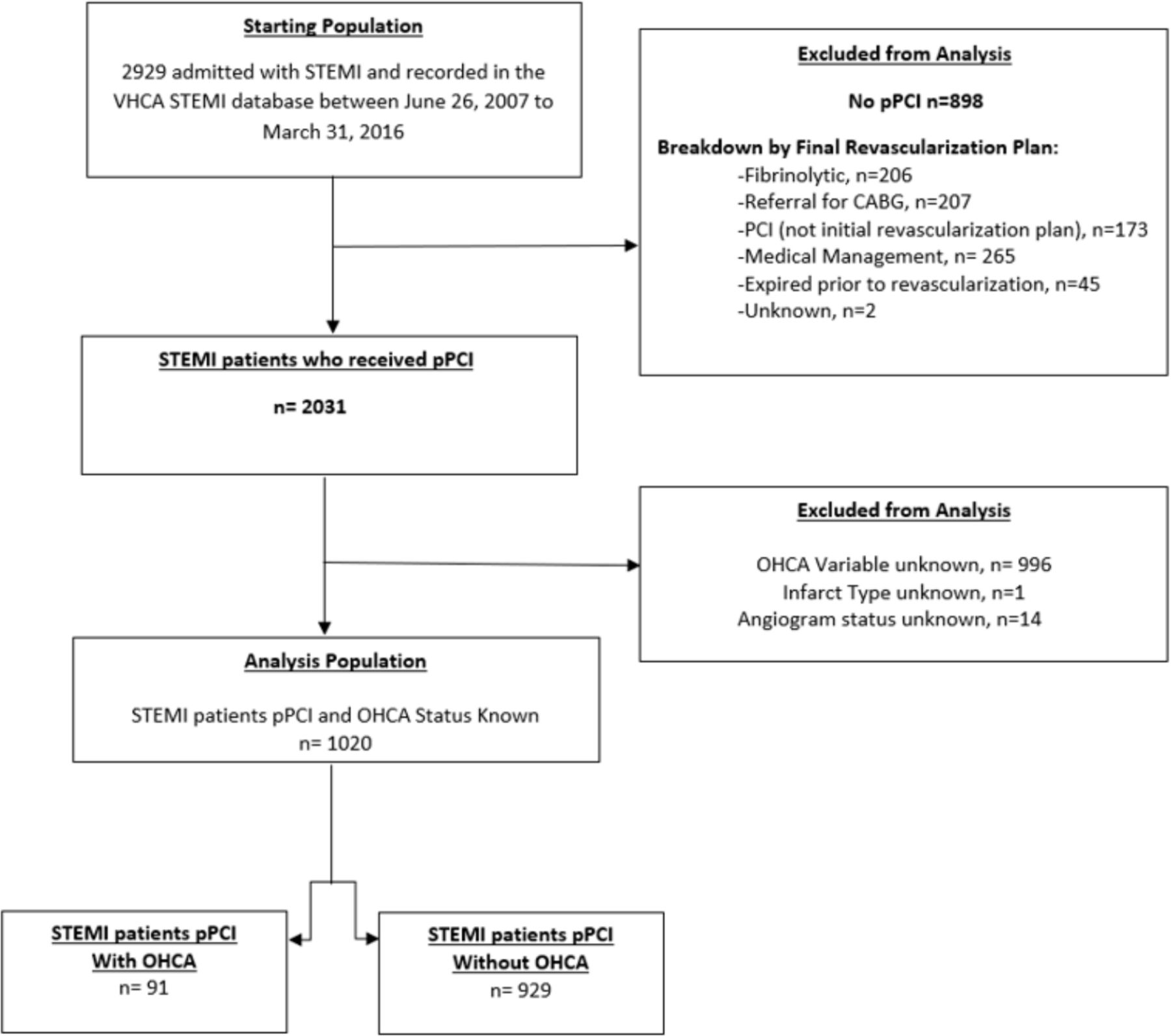
We identified 2929 consecutive patients with STEMI within VCHA who presented with an acute STEMI who survived to hospital admission between 26 June 2007 and 31 March 2016. Of these 2929 patients, 1020 patients underwent successful pPCI and were included in the analysis. We excluded patients who did not undergo a coronary angiogram (n=130), those who did not undergo pPCI (n=898; 206 received fibrinolytic therapy) and patients with missing data (including OHCA status (n=996) or angiogram status unknown (n=14)). OHCA status data were not systematically collected prior to 2012; therefore, there were only 36 patients between 2007 and 2012 whose OHCA status was known. Patients with STEMI were divided into those with (n=91) and those without (n=929) preceding OHCA (figure 1).

The cohort derivation from the initial study population, through exclusions, to the final study population. OHCA, out-of-hospital cardiac arrest; PCI, percutaneous coronary intervention; pPCI, primary percutaneous coronary intervention; STEMI, ST-segment elevation myocardial infarction; VHCA, Vancouver Coastal Health Authority; CABG, Coronary artery bypass grafting.
Definitions
Patients with STEMI were identified after assessment by emergency medical services or by physicians in the emergency department. STEMI was defined using both clinical criteria (symptoms of ischaemia persisting for 20 min or longer) and ECG Criteria (ST elevation of 1 mm or more in any of the following areas: two or more anterior leads, two or more inferior leads, two or more posterior leads or presumed new left bundle branch block). A lesion was considered a culprit lesion if there was a fresh occlusion seen on angiography that resulted in subtotal or total occlusion. The occlusion was considered acute if there was a thrombus present at the site of the occlusion or if the guide wire was able to be passed through the occlusion easily. If there was no acute occlusion on angiography, it was at the angiographer’s discretion to identify the lesion with the most severe reduction of lumen diameter along with corresponding localisation of ST-segment elevation on ECG. OHCA was defined as either having received attempts at defibrillation or chest compressions by lay bystanders or emergency medical services or being pulseless but not having received attempts at defibrillation or CPR. All data were collected in the VCHA STEMI database. Cardiogenic shock during the index hospitalisation was defined as a sustained episode of systolic blood pressure <90 mm Hg and/or cardiac index <2.2 l/min/m2 determined to be secondary to cardiac dysfunction, and/or the requirement for inotropic or vasopressor agents or mechanical support (ventricular assist devices, intra-aortic balloon pump or extracorporeal circulation) to maintain perfusion above 90 mm Hg and/or cardiac index <2.2 l/min/m2. Heart failure on presentation was defined as physician documentation or report of heart failure on presentation or any description of rales or pulmonary oedema on physical examination or chest X-ray, jugular venous distention, shortness of breath, Killip class 2, 3 or 4 or presence of an S3. Major bleeding was defined as a suspected bleeding event during the index hospitalisation that was associated with significant blood loss (haematocrit drop of at least 10% and/or a haemoglobin drop of at least 30 g/L), transfusion of whole blood or packed red blood cells, or use of a surgical or procedural intervention to stop bleeding.
Statistical analysis
Baseline patient demographics and clinical characteristics were summarised using means (SD) or proportions as appropriate. Three separate comparisons were made: LAD versus non-LAD artery involvement within the OHCA group (P1); LAD versus non-LAD artery involvement in the non-OHCA group (P2); combined OHCA group versus the combined non-OHCA group (P3). Differences were tested using the t-test, χ2 test or Fisher’s exact test, as appropriate. In-hospital outcomes were reported across the groups (P1–P3) and differences were tested using t-test for continuous variables, χ2 test for categorical variables or Fisher’s exact test, as appropriate. Comparison of the effect of OHCA by LAD involvement (pinteraction) was based on linear regression or logistic regression, as appropriate. For all analyses, a p-value of <0.05 was considered significant.
Multivariable logistic regression analysis was used to examine the independent impact of ischaemic territory (LAD vs non-LAD) and OHCA on mortality. For left ventricular ejection fraction (LVEF), linear regression was used. We adjusted for age, diabetes, heart failure on presentation, cardiogenic shock on presentation and first medical contact to device time >90 min (or >120 min if first presented to a non-PCI capable hospital). These variables were selected a priori to determine the strength of the association between LAD territory and OHCA on mortality while adjusting for potential confounders. This regression model contained an interaction term between OHCA and ischaemic territory to examine the OHCA effect on mortality by ischaemic territory.
Results
A total of 1020 patients with STEMI were identified. There were 91 patients with STEMI who had a preceding OHCA and 929 who had STEMI without OHCA. The culprit vessel and in-hospital outcomes for each patient was identified. Baseline characteristics of the cohort are described in table 1. The mean age of patients with STEMI with OHCA was 63.6 (±12.6) years and 65.8 (±13.1) years among those without (p=0.135). A left anterior coronary artery (LAD) culprit was identified in 57.1% of patients with STEMI with OHCA and in 47.7% of patients with STEMI without OHCA (difference=9.4%, 95% CI −1.2% to 20.1%, p=0.085).
Clinical characteristics of study patients
Unadjusted analysis
Patients with STEMI with OHCA had higher rates of in-hospital-cardiac arrest (43.3% vs 8.3%, p<0.001), heart failure (50.5% vs 11.3%, p<0.001), major bleeding (22.0% vs 8.6%, p<0.001), cardiogenic shock (49.5% vs 5.7%, p<0.001), mortality (35.2% vs 3.3%, p<0.001) and reduced LVEF (42.9% vs 47.3%, p<0.001) compared with patients with STEMI without OHCA.
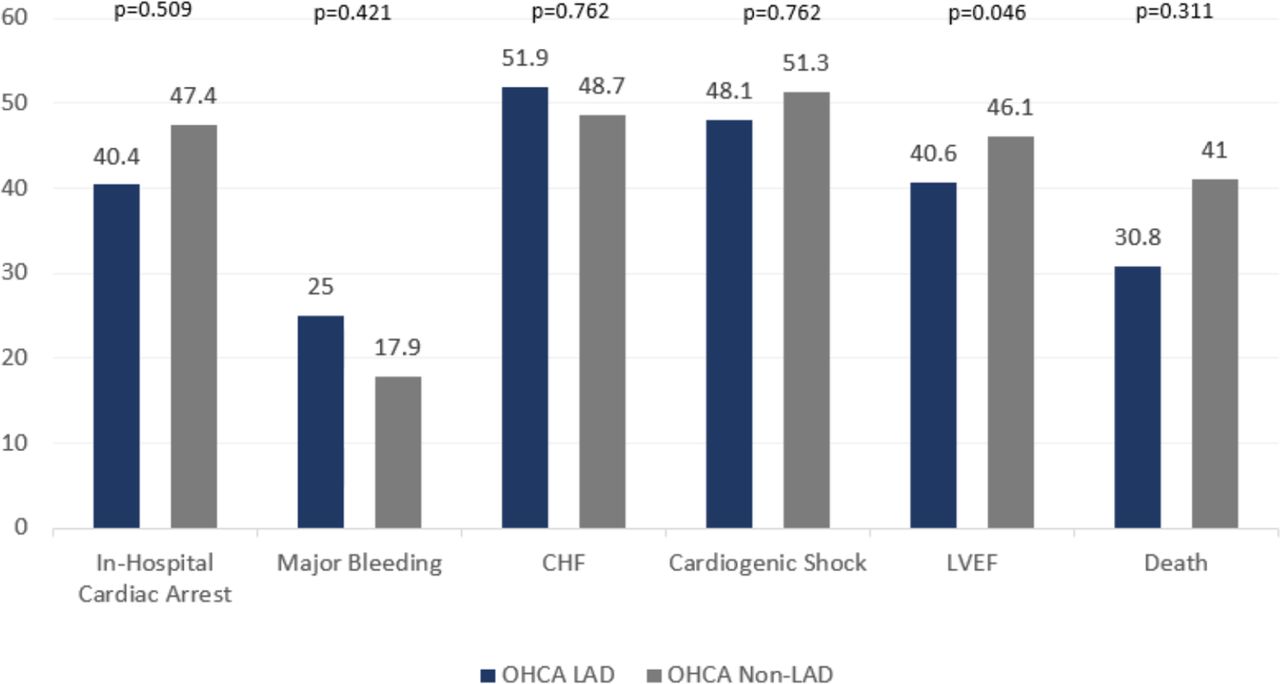
Among patients with STEMI with OHCA, the presence of an LAD culprit was not associated with increased risk of in-hospital mortality but was associated with a lower LVEF (40.6% vs 46.1%, p=0.046; figure 2). Conversely among patients with STEMI without OHCA, the presence of an LAD culprit vessel was associated with increased rates of heart failure (18.1% vs 5.2%, p<0.001), in-hospital cardiac arrest (10.7% vs 6.2%, p=0.014), cardiogenic shock (8.4% vs 3.3%, p<0.001), reduced LVEF (43.0% vs 51.2%, p<0.001) and mortality (5.2% vs 1.3%, p=0.003) compared with patients without an LAD culprit (figure 3).

Unadjusted in-hospital outcomes in patients with ST-segment elevation myocardial infarction with out-of-hospital cardiac arrest (OHCA), by left anterior descending (LAD) involvement. CHF, congestive heart failure; LVEF, left ventricular ejection fraction.

Unadjusted in-hospital outcomes in patients with ST-segment elevation myocardial infarction without out-of-hospital cardiac arrest (OHCA), by left anterior descending (LAD) involvement. CHF, congestive heart failure; LVEF, left ventricular ejection fraction.
Examining the outcomes of in-hospital cardiac arrest, major bleeding and LVEF revealed that the impact of OHCA was not significantly different by the presence of an LAD culprit vessel (LAD=40.4%, no LAD=47.4% pinteraction=0.077, LAD=25.0%, no LAD=17.9% pinteraction=0.405, and LAD=40.6%, no LAD=46.1% pinteraction=0.232, respectively). Conversely, the presence of an LAD culprit significantly altered the association between OHCA and congestive heart failure, cardiogenic shock and mortality (LAD=51.9%, no LAD=48.7% pinteraction=0.009, LAD=48.1%, no LAD=51.3% pinteraction=0.033 and LAD=30.8%, no LAD=41.0% pinteraction=0.007, respectively).
Adjusted analysis
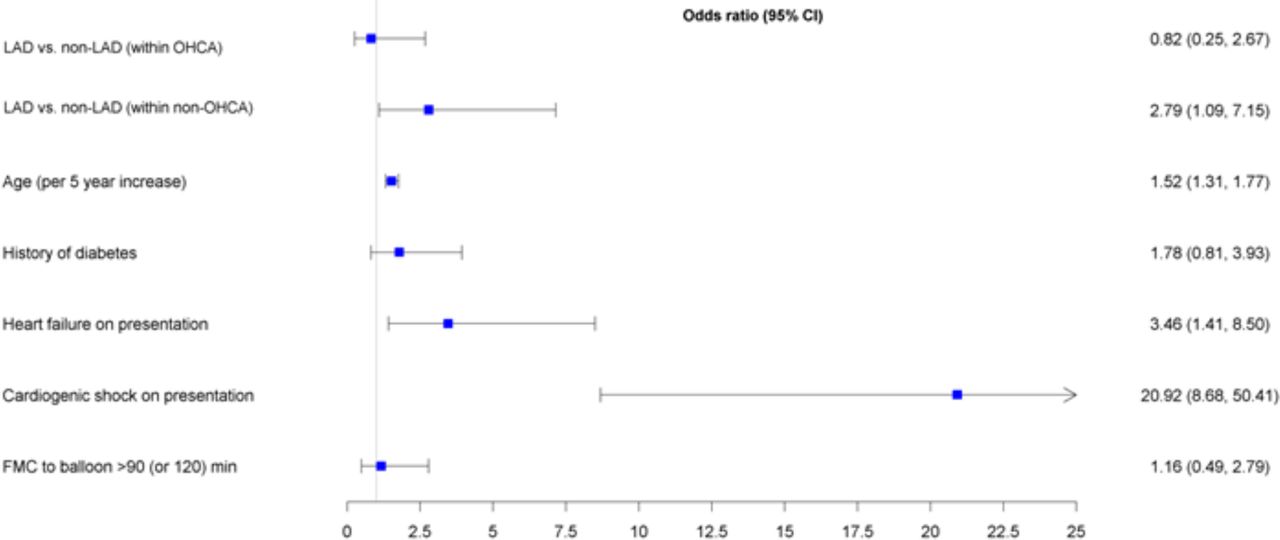
Logistic regression models demonstrated that the presence of OHCA was independently associated with mortality among patients with STEMI without (OR 7.75, 95% CI 2.03 to 29.68) but not with (OR 2.28, 95% CI 0.76 to 6.87) LAD involvement. However, the association between OHCA and mortality was not significantly different between each group (pinteraction=0.112, figure 4). The presence of an LAD culprit was independently associated with mortality among patients with STEMI without OHCA (OR 2.79, 95% CI 1.09 to 7.15) but not with OHCA (OR 0.82, 95% CI 0.25 to 2.67).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Logistic regression examining the impact of ischaemic territory (left anterior descending (LAD) vs non-LAD) and out-of-hospital cardiac arrest (OHCA) on mortality. FMC, first medical contact.
Additionally, the presence of an LAD culprit was not independently associated with in-hospital cardiac arrest or major bleeding among patients with or without OHCA. In contrast, an LAD culprit was independently associated with heart failure and cardiogenic shock in patients without OHCA and not among patients with OHCA. An LAD culprit was independently associated with reduced ejection fraction in patients both with and without OHCA.
Discussion
The current analysis sought to determine an association between an LAD culprit with in-hospital outcomes of patients with STEMI with and without OHCA. Our data confirmed that patients with STEMI with OHCA experienced worse in-hospital outcomes compared with those without. However, there was no independent association of an LAD culprit with mortality among patients with STEMI presenting with OHCA. Conversely, with the exception of in-hospital cardiac arrest, an LAD culprit retained an independent association with worse clinical outcomes among patients with STEMI without OHCA.20 Although a recent study has shown no clinical benefit of early angiography among OHCA survivors in the absence of acute ST elevation,21 non-randomised data have suggested favourable clinical outcomes with early angiography among OHCA with acute STEMI.22 However, prior to our study, little was known about whether specific angiographic features (and, in particular, LAD involvement) were independently associated with in-hospital mortality and other in-hospital outcomes among patients with STEMI with OHCA.
Although there is a suggestion of an increased incidence of left main coronary artery and multivessel disease involvement in patients with STEMI with OHCA compared with those without OHCA,10–12 the literature has yielded inconsistent signals regarding the presence of an LAD culprit and OHCA complicating STEMI10–12 16 18 nor the association between an LAD culprit and clinical outcomes among OHCA survivors with STEMI.10–12 18 19 23–25 Our study is one of the largest evaluating the association of LAD on outcomes among patients with STEMI with and without OHCA and extend on those from previous analyses. Our findings differ from previously described poor outcomes in non-OHCA presenting with acute anterior territory STEMI compared with non-anterior-related STEMI.11 13 14 We hypothesised that there would be a higher incidence of LAD involvement among patients with STEMI with OHCA who survive to hospital admission, and that LAD involvement would confer worse in-hospital outcomes among patients with STEMI irrespective of OHCA status. Instead, we found similar rates of LAD involvement among patients with STEMI with and without OHCA. Moreover, our data also showed a differential association of LAD involvement with adverse in-hospital outcomes among patients with STEMI with and without OHCA, with a finding that LAD involvement was only associated with increased mortality among those patients without OHCA.
Our data would therefore suggest that the worse prognosis seen among patients with STEMI with OHCA is mainly driven by clinical characteristics other than the presence of high-risk angiographic anatomy, and that alternative mechanisms other than LAD involvement contribute to the higher mortality and worse hospital outcomes in patients with OHCA following successful reperfusion with pPCI. Several prehospital features have been associated with worse prognosis, including increased age, delayed CPR, initial unshockable rhythm, renal insufficiency, >30 min to ROSC and reduced ejection fraction on hospital admission.15 17 Indeed, integer-based risk scores based on clinical variables have been constructed to try and define which patients presenting with acute coronary syndromes are at increased risk of developing cardiac arrest.26
Clinicians treating patients with STEMI and OHCA should continue to use management strategies that emphasise early identification of patients with STEMI with OHCA and rapid reperfusion. However, clinicians should also focus on identifying and managing other concomitant high-risk features such as shock and neurological injury that drive poor outcomes in these patients given that approximately two-thirds of patients with OHCA who survive to hospital admission die from neurological injury, and the remaining one-third die from cardiogenic shock.27 28 As such, our study further highlights the complexity surrounding the prognostication following OHCA and underscores the need for further studies to delineate high-risk features in patients with STEMI with OHCA to help support clinical decision-making.
We acknowledge some limitations to our study. First, our data are observational and we cannot control for potential selection bias. In the present study, only patients who had ROSC and presented with ST-segment elevation were included in the analysis and we cannot exclude the possibility that the culprit artery of the successfully resuscitated patients could have varied significantly from those who did not have ROSC and never underwent angiography. In this way, it may be possible that there was either a higher incidence and/or a potential association of LAD with worse clinical outcomes among this cohort of patients who were not successfully resuscitated. However, we found no difference in the distribution of LAD involvement versus no LAD involvement among those patients who were sent for angiography. Second, our finding that there was no statistical association between OHCA and LAD may be a result of being underpowered with only 91 patients in this subgroup. There were relatively fewer patients with STEMI with OHCA than patients with STEMI without OHCA. However, there was a greater proportion of patients with LAD involvement in the OHCA group than in the non-OHCA group, though the lower number of patients with OHCA in this cohort may account for our inability to demonstrate a statistically significant difference in LAD involvement. Finally, the VCHA STEMI Registry does not contain detail regarding the precise location of the culprit lesion within the infarct-related artery; previous data have suggested that the presence of a proximal LAD culprit portends poorer outcomes among patients with STEMI. Therefore, it is possible that the presence of proximal versus non-proximal LAD disease may have impacted our results.28
Conclusion
Compared with patients with STEMI without OHCA, those with OHCA experienced worse in-hospital outcomes. While the presence of an LAD culprit was associated with worse outcomes among patients with STEMI without OHCA, this association was not seen among those with OHCA. LAD involvement was not independently associated with mortality in patients with OHCA but was seen in patients with STEMI without OHCA. These data suggest that there is a differential association of LAD culprit with poorer outcomes among patients with STEMI with and without OHCA and that other high-risk features may contribute to poor outcomes among patients with STEMI with OHCA. Further studies are needed to identify these high-risk features to support postarrest care clinical decision-making.
References
Footnotes
Twitter @nimamogh
Contributors GW, CBF and MB conceived the paper and drafted the article. All authors contributed to the data analysis and interpretation. All authors were involved in the critical revision of the article and the final approval of the version to be published.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval This study was approved by the University of British Columbia Clinical Research Ethics Board (H17-00375).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information. All data relevant to the study are included in the article or uploaded as supplementary information.