Article Text

Abstract
Introduction Ineffective hospital discharge communication can significantly impact patient understanding, safety and treatment adherence. This may be especially true for cardiology inpatients who leave the hospital with complex discharge plans delivered in a time-pressured discharge discussion. The goal of this pilot trial was to determine if providing supplemental audio-recorded discharge instructions is feasible and to explore its impact on cardiology patients' ability to understand and self-manage their care .
Methods and analysis We will conduct a parallel-group, randomised controlled trial in adult cardiology inpatients with balanced blocking by a physician. Patients (n=50) will be randomised to usual care (verbal discussion and written summary) or intervention (usual care, plus audio-recorded discharge discussion provided to patients on a portable electronic recording device). Enrolled patients will complete study assessments immediately prior to the discharge discussion, immediately postdischarge discussion and 1 week after hospital discharge by telephone. Primary outcomes include the proportion of eligible providers and inpatients who agree to take part in the trial, the proportion of inpatients who receive the audio recording in accordance with a fidelity checklist, and the proportion who use the audio recording. We will analyse preliminary data about the impact of audio recording on patient activation, health confidence, provider communication ability, adherence and 30-day readmissions.
Ethics and dissemination This trial was approved by The Committee for the Protection of Human Subjects (CPHS) at Dartmouth College (CPHS# 00031211). Findings will be disseminated in scientific journals and at meetings.
Trial registration number NCT03735342
Protocol version 1.0
- cardiology
- audio recording
- hospital discharge
- self-management
- understanding
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known about this subject?
Patients are beginning to audio record clinical interactions with their healthcare providers, and systematic reviews report improvement in patients’ recall, understanding and satisfaction, primarily in the outpatient setting, but the full utility of audio recordings as a tool to promote the review of discharge instructions has not been determined.
What does this study add?
The objective of the Heart Sounds pilot study is to determine if it is feasible to apply audio recordings as an adjunctive communication technology at discharge in a rapid-turnover inpatient cardiology unit, where the risk of communication errors and misunderstandings may be high.
How might this impact clinical practice?
If audio recordings are feasible and acceptable for complex cardiovascular patients and their providers, this intervention could be routinely offered and may have the potential to impact key patient outcomes such as understanding, self-management, adherence and readmission rates.
Introduction
Background and rationale
Ineffective discharge communication can impact patient safety, treatment adherence and readmission rates.1 2 Patients with cardiovascular disease, including those with congestive heart failure (CHF), dysrhythmia and acute coronary syndrome (ACS), represent a significant proportion of hospitalised patients and, as a result, are at elevated risk for discharge communication failure.3 Their discharge plans are complicated by long and dynamic medication lists, postprocedural care instructions and drastic lifestyle changes. Understanding these plans may be difficult since patients receive a large amount of technical information in a time-pressured discharge process. Studies confirm patients’ difficulty retaining this information, especially when it is provided verbally, citing failure to remember more than 80% of what was communicated within 1 minute. When patients do recall important information, 50% is recalled incorrectly.4 Multiple complex factors, including age, health literacy, education, preferred learning style and provider communication ability, affect the retention of medical information.5 Patients who understand their discharge instructions are more likely to adhere to treatment plans and are 30% less likely to be readmitted.6 Our hospital’s Hospital Consumer Assessment of Healthcare Providers and Systems (HCAPS) data corroborate the difficulty cardiology inpatients have recalling and retaining important information, indicating they routinely struggle to understand their discharge instructions compared with patients discharged from other inpatient units. This may result in difficulty managing their care at home and contributes to frequent postdischarge telephone calls7 (SL Schott, unpublished data, 2018).
Many discharge improvement plans have been attempted,6 and patients appear willing to engage in innovative information delivery strategies to help mitigate communication issues.8 9 One novel strategy to improve communication of discharge instructions is emerging in the form of sharing audio recordings. Reviews indicate that sharing audio-recorded clinic visits with patients, mainly in oncology and paediatrics, has resulted in improved patient recall, satisfaction and understanding.10 11 However, the true utility of provider–patient audio recordings has yet to be determined, and its routine practice is in its infancy. To date, the feasibility of implementing this strategy to improve the delivery of critical discharge information for cardiology inpatients has not been examined. This study may serve to further understand the capability of audio recording as a quality improvement tool at the fragile time of inpatient discharge. Our long-term goal is to improve health outcomes for patients by enhancing access to their health information. Making this information more understandable and actionable may provide greater health confidence and self-management ability. Ultimately, improving the efficacy of the discharge communication process for patients with ACS and CHF may affect adherence, thereby decreasing morbidity and 30-day readmission rates, an important care quality metric.
Aims and objectives
We will conduct a pilot, parallel-group, randomised controlled trial to determine the feasibility and acceptability of providing audio-recorded discharge instructions to patients discharged from an inpatient cardiology service. We will also explore the impact of audio recording on exploratory outcomes associated with self-management.
Specific aims:
Determine whether providing audio-recorded discharge instructions as a supplemental discharge communication tool will be feasible for cardiology providers and patients to use during the inpatient discharge discussion.
Determine whether patients and their families will use audio-recorded discharge instructions after their hospital discharge to self-manage care.
Explore the impact of audio recording on patient understanding of their discharge instructions, health confidence, patient activation, general medical adherence, medication adherence, provider communication ability and postdischarge telephone call rates.
Methods and analysis
Study setting
This pilot trial will be conducted at a single site: the general cardiology inpatient unit at Dartmouth Hitchcock Medical Centre (DHMC), a level I trauma and academic medical centre in Lebanon, New Hampshire, USA.
Eligibility criteria
Providers: We will recruit patients discharged by associate providers (APs, physician assistants and nurse practitioners). We chose to focus on our pilot on APs because they work most consistently on the inpatient unit and are responsible for creating their patients’ discharge instructions. Enrolled APs may perform the discharge discussion alone or may choose to participate in the discharge discussion with the patient’s bedside nurse, whichever reflects their preferred discharge style. To be eligible for inclusion, APs and nurses must (1) have previous experience participating in the discharge communication process with cardiology inpatients and (2) be willing to participate in the study including the possibility of having their discharge conversation recorded.
Patients: To be eligible for inclusion, patients must be (1) 18 years of age or older, (2) admitted to the inpatient cardiology unit at DHMC, (3) comfortable reading and writing in English and (4) willing to have their discharge conversation recorded. We will exclude patients (1) without capacity to provide consent to the project, as determined by the research assistant (RA); (2) with dementia, schizophrenia and other psychotic disorders, substance-abuse disorders, uncorrectable hearing or visual impairment, as determined by the discharging provider and (3) being discharged to facilities other than home, or patients living in skilled nursing homes or hospice, as determined by the discharging provider, because they engage far less in self-management. The majority of patients are admitted to this inpatient cardiology unit with either ACS or CHF. Given the exploratory nature of our research, we retained broad inclusion criteria to explore whether audio recordings are feasible, acceptable and potentially more beneficial for patients with particular diagnoses.
Intervention
Usual care: On the day of their hospital discharge, enrolled patients randomised to the usual care arm received a verbal discharge discussion with an AP and written discharge instructions.
Intervention: On the day of their hospital discharge, enrolled patients randomised to the audio recording arm (intervention) received usual care, plus a portable electronic device that contains a re-playable audio recording of the discharge discussion. In addition, participants will have the option to record the discharge discussion on a personally owned smartphone or receive access to the recording online using the Health Insurance Portability and Accountability Act (HIPAA)-compliant Open Recording and Logging Systems (ORALS).12 Prior to patient enrolment, the research team and the enrolled APs will be trained on how to use the recording device. Patients will also receive printed instructions detailing how to start, stop and retrieve recordings, and will be asked to demonstrate their use of the recording device to confirm understanding of these instructions prior to discharge.
Recruitment
Providers: APs and nurses will be invited to learn about the study’s purpose during department conferences, via recruitment emails and flyers. Interested APs and nurses will meet with a study team member to complete written informed consent. Those who decline will be asked to provide a reason for their decision.
Patients: When an enrolled AP is working on the inpatient cardiology unit, an RA will meet with the provider and multidisciplinary care team to identify eligible patients scheduled for discharge during the morning discharge huddle at 10 am each Monday through Friday. The RA will approach potential patients to determine their interest, confirm eligibility and complete informed consent. An approximate time for the discharge communication will be confirmed with staff and written on the unit ‘whiteboard’. The RA will be paged back to the inpatient unit when the discharging AP and nurse are ready to discuss the instructions at the patient’s bedside. The RA will proceed with study activities according to allocation assignment. All patients in the intervention arm will receive their recorded discharge instructions on a simple, reusable, portable MP3 playback device that requires no internet or computer access and will be introduced to two additional options for recording. The RA will return to the patient’s bedside at the predetermined discharge time to prepare the recording device(s).
Allocation
A member of the study team not involved in recruitment and data collection, primary investigator (PI) (PJB) will generate a study arm allocation list for each provider using a block randomisation at the provider level (blocks of four that are balanced in the number of allocations to each arm but randomised in terms of order, eg, ABAB and AABB). This method was chosen because of the small sample size and to ensure an equal number of patients were assigned to each study arm. The PI (SS) RAs, providers and patients will be blind to this allocation process, including the size of each block. After baseline data are collected (T0), the RA will open a sealed randomisation envelope to reveal the patient’s allocation assignment immediately prior to the discharge discussion.
Study procedures
Immediately following documentation of informed consent, the RA will collect patient demographics and the T0 baseline assessment. The RA will leave the unit and return to the patient’s bedside at the predetermined discharge time or when they are paged by the charge nurse or discharging provider. In both arms, the RA will leave the patient’s room during the discharge discussion and will return to complete the T1 assessment after the discharge discussion is complete, documenting time spent in the discussion.
Usual care arm: Patients will experience the usual discharge communication practice, which includes a bedside verbal review of written discharge instructions by the discharging provider(s) (online supplementary material 1). The APs may conduct this review alone or with the patient’s nurse.
Supplemental material
Intervention arm: When providers and the patient are ready for the discharge discussion, the RA will place a sign outside the patient’s room to alert providers and other caregivers that a recording is in process. The RA will set up one MP3 digital recorder and one backup MP3 digital recorder near the patient’s bedside and instruct the patient on how to stop should they choose to do so. If the patient chooses to record the discharge conversation using ORALS, an electronic tablet will be used to automatically record and securely transfer the recording to the HIPAA-compliant server. If the patient chooses to record on their personal smartphone device, the patient will be instructed on when to start and stop that recording. Patients will experience the usual discharge communication practice that includes a bedside verbal review of written discharge instructions by the discharging provider(s) (online supplementary material 1), but the conversation will be audio recorded. The RA will leave the room immediately after starting the recording(s) and will return after the discharge conversation ends. The RA will demonstrate the use of the MP3 device and provide instructions (playback and battery charging) for this and other types of recordings (ORALS and smartphone) chosen. The RA will document the type(s) of recordings the patient received.
Data collection, management and analysis
Data collection
Providers: We will obtain demographics from providers who agree to participate via survey, including age, sex, race, ethnicity, years in practice and specialty, and will invite enrolled providers to participate in a 15 min semistructured interview about their experience using audio recordings after the enrolment is complete. We will anonymously document reasons providers declined to participate. We will document time providers spent in the discharge discussion. Enrolled APs will report participating patients’ primary diagnosis to the RA.
Patients: At the time of enrolment, and before the discharge discussion, all patients will be asked to complete a baseline survey (on paper) consisting of sociodemographics, health literacy,13 14 health confidence questions15 and the Patient Activation Measure (T0).16 Additional outcome data will be collected on the inpatient unit immediately after the discharge discussion (T1) and by telephone 1 week postdischarge (T2) (table 1). On telephone follow-up, patients in the intervention arm will be asked additional interview questions about their experience using their audio recording device(s). DHMC data analytics will use the electronic medical record to report unit-level aggregate data on sociodemographics and disease burden via the Charlson Comorbidity Index so it may be compared with enrolled patients.17
Study outcomes
Outcomes
Participant timeline
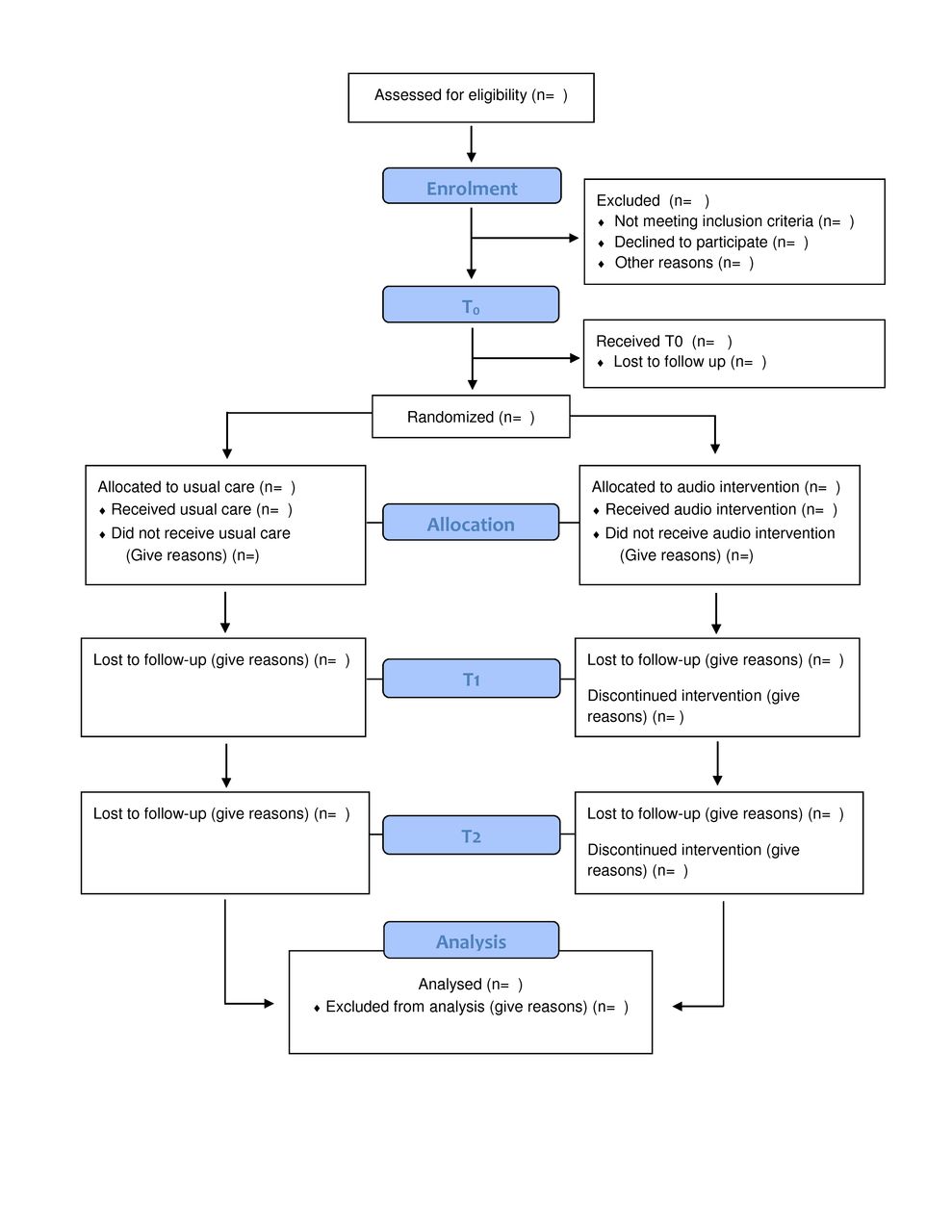
The participant timeline is outlined in figure 1.

{kind=link}
Consort diagram depicting participant timeline and progression through all phases of the study, including final data analysis.
Sample size
We plan to recruit 50 adult cardiology inpatients for this pilot trial: 25 patients in the usual care arm and 25 patients in the intervention (audio) arm. This number is based on the time constraint to complete all aspects of the study within 1 year and based on the number of daily discharges, including a conservative estimate of enrolling approximately three patients per week over a 16-week period. Prior to study initiation, we plan to recruit a minimum of five APs who will be routinely present on the inpatient cardiology unit to participate in both arms of the study.
Data management
Study data will be deidentified and securely managed in accordance with Committee for the Protection of Human Subjects (CPHS) by trained research team members using encrypted services licensed by Dartmouth College, including accessing and maintaining audio recordings on a HIPAA-compliant cloud storage system. (Please see data management plan in online supplementary material 2.
Supplemental material
Statistical methods
Quantitative analysis
Baseline data: We will compare baseline sociodemographics, patient activation and health literacy data between the usual care and intervention arms using χ2 tests for categorical data (Fisher’s exact test', where cell sizes of analysis are below 5) and Student t-tests for variables that are closer to continuous in form.
Primary outcome (aim 1): We will consider audio recordings feasible if >70% of eligible providers and patients agree to participate in the study and patients receive the intervention according to a fidelity checklist. We will consider audio recordings acceptable for patients if recording use is 70% or higher.11 We will also compare attrition rates and differences in use according to method selected for listening to recording (MP3, smartphone and ORALS system).
Exploratory outcomes and covariates (aim 2):
Within group analyses.
We will compare within-arm differences in health confidence and 13-Item Patient Actitvation Measure (PAM-13) scores before discharge and at 1 week postdischarge using the Wilcoxon Sign Test (continuous data) and a McNemars Test (categorical data).
Between group analysis.
We will compare between arm (usual care vs intervention) differences for continuous (PAM-13, Communication Assessment Tool (CAT), Medical Outcomes Study and Adherence to Refills and Medications Scale)16 18–20 and categorical (Health Confidence: Confident vs not confident, CAT top score) outcomes and baseline characteristics, using Mann-Whitney U test and Fisher’s exact test, respectively. We will control for provider by using a random effects model. We will compare differences in postdischarge telephone call counts, the reasons for calling and the difference in the proportion of patients who use (read) the written discharge instructions. In the intervention arm, we will explore the differences between patients who listen to their audio recording and those who do not. STATA-15 data analytic and statistical software will be used. A p value of <0.05 will be considered statistically significant.
Qualitative analysis
Interviews with patients and providers (APs and nurses) about their experience using audio recordings in the study will be recorded (when permission is granted) and transcribed. Interview data will be analysed using an iterative, inductive thematic approach.21 22 Two coders will independently review each transcript line-by-line using the qualitative research software ATLAS.ti, identifying possible descriptive codes then discussing codes to build a shared code structure for analysis, which will be used to code all data.21 When coding is complete, a three-person team will meet to discuss the data and codes, developing unifying analytic themes to help interpret the data and summarise the findings.21
Ethics and dissemination
Data monitoring
After the review of our data collection methods and monitoring plan with Research Operations at the Heart and Vascular Centre, Dartmouth-Hitchcock, we were not required to form a data safety monitoring committee, given the minimal risk to participants. As a substitute, we chose to engage independent research supervisors at the Heart and Vascular Centre and The Dartmouth Institute for Health Policy and Clinical Practice not directly involved in data collection to intermittently evaluate the progress of the project, fidelity to project protocol and data integrity. Data integrity will be assessed when 25%, 50% and 75% of participants are enrolled. After discussion with independent advisors, PIs will decide whether concerns regarding protocol adherence, data collection or provider–patient participation rise to the level of pausing or terminating the trial.
Harms
Minimal social, legal and psychological risks are anticipated as a result of this study. However, several steps to prevent harm were taken, and channels for reporting and addressing harms were established, including recording only information that reflects standard written discharge instruction, providing education about how to safely maintain and share recorded information and the provision of immediate contact information, including telephone numbers and email addresses for study PIs. Should a data leak occur or unexpected harm be reported, CPHS will be notified immediately and study procedures will cease until an action plan to address a leak is set up in collaboration with CPHS.
Auditing
The auditing plan includes weekly team meetings to review recruitment, data collection and technical delivery of recordings, a fidelity-to-study procedures checklist captured for every patient, a review of a random selection of 25% of survey data and audio recordings and observation of the recruitment and intervention process by PIs for five participants.
This research involves human subjects and has received institutional review board approval from the CPHS at Dartmouth College (CPHS#00031211).
Protocol amendments
Proposed amendments to the original protocol will be submitted to CPHS at Dartmouth College for approval prior to initiating any changes in study design, recruitment, data acquisition or data analysis. Any protocol amendments will be added to the study record on Clinicaltrials.gov.
Consent or assent
Written informed consent will be obtained by a member of the research team who has received the following: CITI certification, consent and interviewing training, electronic medical record access courses and audio recording training.
Confidentiality
Confidentiality of data are maintained by limiting audio recordings to reflect information typically provided in the written discharge instructions. Patients are instructed on how to stop and start recordings during the discharge discussion and on discharge, how to safely maintain and share audio recordings, similar to printed discharge instructions. The research team will store audio recordings, collected survey data and postdischarge telephone call data in Dartmouth-sponsored HIPAA-compliant encrypted systems. All survey, telephone data and qualitative interview data will be deidentified and analysed in aggregate to ensure confidentiality of individual responses.
Access to data
PIs and research team members at Dartmouth Hitchcock Medical Centre will have access to the final data set. Additionally, deidentified, aggregate data collected using the PAM-SF (PAM-13) will be provided to Insignia Health at the conclusion of the study as part of a licensing agreement to use this measure.
Dissemination policy
The findings will be disseminated through usual academic channels, including meeting presentations as well as peer-reviewed publications. Written materials and public presentations will not include any personally identifiable data. Based on journal requirements, we will make available a deidentified database of study data.
DISCUSSION
Findings from this project will contribute to our understanding of the feasibility and acceptability of implementing an inpatient care recording strategy as a tool for communicating critical, often forgotten, discharge information. Our study will also explore the potential of sharing recordings with patients to improve self-management, which in turn could contribute to a reduction in high readmission rates reported in cardiology patients. The potential applications of recordings are broad and growing. Advances in novel machine learning and natural language processing techniques open new avenues in medicine, such as automated documentation of clinical notes extracted from the recorded conversations to decrease provider burden.23 However, it is important to also consider the privacy and confidentiality implications of recordings, for example, recording and sharing of clinically sensitive conversations and medicolegal concerns of providers. Yet to date, the use of recordings for malpractice suits has not been documented in the small number of clinics where recordings are routinely made available to patients and in at least one case in Arizona, provider participation in recordings may be protective and may result in decreased malpractice premiums.10 11 Ownership of the recording is another issue to consider, for example, the application of HIPAA to recordings made and stored by patients (a non-health entity not subject to HIPAA) and not the health system.11 A lack of policies to guide the recording and sharing of clinical visits needs to be addressed,10 and findings from our project, both quantitative and qualitative, can contribute to this conversation. If managed securely as data in an electronic medical record, recordings could transform healthcare, providing more accurate clinical records and allowing patients and families to revisit medical information that is often forgotten.23
Acknowledgments
We thank the associate providers and nurses who participated in this study; Dr Mark Creager, Director, Heart and Vascular Center; Dr Jeffrey Kuvin, Section Chief, Cardiovascular Medicine; and Ms Allison Hawke, Research Operations Manager, Heart and Vascular Center, Dartmouth Hitchcock Medical Center.
References
Footnotes
Contributors All authors have provided substantial contributions to the conception or design of the work, or the acquisition, analysis or interpretation of data.
Funding This work was supported by a Pilot Award from The Hitchcock Foundation #250-4113.
Competing interests Primary investigator (PI) (SS) and co-investigators (MD, SD, JS, MC, MB and JOM) have no financial or competing interests to disclose. The PI (PJB) has no financial interests to disclose but does lead a research group, OpenRecordings, that studies sharing audio/video recordings with patients, caregivers and clinicians and has developed the online sharing technology offered in this project (http://www.openrecordings.org/orals).
Patient consent for publication Not required.
Ethics approval The research involves human subjects and has received institutional review board approval from the Committee for the Protection of Human Subjects, Dartmouth College (CPHS#00031211).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement There are no data in this work.