Article Text

Abstract
Objectives To analyse the effect of the implementation of a transcatheter aortic valve replacement (TAVR) and multidisciplinary heart team programme on mortality in severe aortic stenosis (AS).
Methods A retrospective, observational cohort study was performed using the echocardiography, cardiothoracic surgery and TAVR databases between 1 January 2006 and 31 December 2016. Outcomes were compared between the pre- and post-TAVR programme eras in a tertiary referral centre providing transcatheter and surgical interventions for AS.
All-cause mortality within 5 years from diagnosis was determined for 3399 patients with echocardiographically defined severe AS.
Results Of 3399 patients, there were 210 deaths (6.2%) at 30 days and 1614 deaths (47.5%) at 5 years.
Overall, patients diagnosed in the post-TAVR programme era were older, with a lower ejection fraction and more severe AS, but were less comorbid.
Among 705 patients undergoing intervention, those in the post-TAVR programme era were older, with a lower ejection fraction and more severe AS but no significant differences in comorbidities.
Using an inverse probability weighted cohort and a Cox proportional hazards model, a significant mortality benefit was noted between eras alone (HR=0.86, 95% CI 0.77 to 0.97, p=0.015). When matching for age, comorbidities and valve severity, this benefit was more evident (HR=0.82, 95% CI 0.73 to 0.92, p=0.001).
After adjusting for the presence of aortic valve intervention, a significant benefit persisted (HR=0.84, 95% CI 0.75 to 0.95, p=0.005).
Conclusion The implementation of a TAVR programme is associated with a mortality benefit in the population with severe AS, independent of the expansion of access to intervention.
- aortic stenosis
- multidisciplinary communication
- transcatheter aortic valve replacement
- surgical aortic valve replacement
- cardiovascular outcomes
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- aortic stenosis
- multidisciplinary communication
- transcatheter aortic valve replacement
- surgical aortic valve replacement
- cardiovascular outcomes
Key questions
What is already known about this subject?
Patients with untreated severe aortic stenosis have poor outcomes.
Minimally invasive transcatheter aortic valve replacement (TAVR) has expanded the treatment population and improved mortality.
Multidisciplinary heart team (MDHT) discussions are a requirement for government funding, but a clear benefit for this process has not yet been demonstrated.
What does this study add?
Using an observational, retrospective database including patients before and after the introduction of a TAVR/MDHT programme, we demonstrated a mortality benefit in the post-MDHT era, independent of the expansion of intervention.
How might this impact on clinical practice?
This provides useful evidence of an objective benefit for the MDHT, separate from the TAVR procedure itself.
Introduction
Severe AS has long been known to increase mortality,1–7 but the development of effective new transcatheter-based interventions for elderly or comorbid patients with AS at intermediate to prohibitive surgical risk has reignited interest in the field of valvular heart disease. Despite increases in age and comorbidity in this population, both surgical aortic valve replacement (SAVR) and transcatheter aortic valve replacement (TAVR) remain superior to medical therapy in symptomatic, severe AS.8–11
The multidisciplinary team is being used with increased frequency in many medical disciplines, with varying impacts on outcomes.12–18 Many cardiac trials and therapies are now mandating the involvement of a multidisciplinary heart team (MDHT), primarily based on the methodologies and outcomes of the SYNTAX and PARTNER trials.8 12 19 20 Aortic stenosis (AS) is an ideal condition to use the variety of expertise inherent in an MDHT due to the increased age and comorbidity of these patients, and has a class 1 recommendation from the American and European cardiac societies.21 22 An MDHT review involving a structural heart specialist, a cardiothoracic surgeon and a non-implanting physician prior to TAVR is required for Commonwealth Medical Benefits Scheme funding20 in Australia. In reality, many more practitioners are often involved, including radiologists, vascular surgeons, geriatricians and nursing staff. Despite the organisational difficulty and high costs involved in such a requirement, the evidence for a clinical benefit of the MDHT in AS is lacking.23 24
We analysed the effect of the introduction of a TAVR programme, defined as the combination of the minimally invasive transcatheter therapy as well as the accompanying AS MDHT, on 5-year survival in a population of patients with echocardiographically defined severe AS, from the first echocardiogram demonstrating AS. We hypothesised that despite an older and more complex patient cohort, the implementation of the TAVR programme would result in an overall reduction in mortality in the population with severe AS. It was also hypothesised that the MDHT itself may reduce mortality independently of the expanded access to intervention, providing evidence for its use in the population with severe AS.
Methods
Patient population
A retrospective, observational cohort study of the echocardiography database for the Southern Adelaide Local Health Network in South Australia (SA) was designed to review all consecutive patients undergoing transthoracic echocardiography in a high-volume echocardiography department between 1 January 2006 and 31 December 2016. From this population, patients were included in the analysis if they had at least one severe criterion to define AS.
Definition of severe AS and echocardiographic parameters
A patient population was identified as having severe AS if any of the following echocardiographic criteria were achieved: aortic valve (AV) mean gradient ≥40 mm Hg, AV peak velocity ≥4.0 m/s, AV area ≤1.0 cm2 or Dimensionless Performance Index ≤0.25, as per the criteria outlined in the joint statement from the European Association of Cardiovascular Imaging and the American Society of Echocardiography.25 The year of the first echocardiogram demonstrating at least one marker of severe AS was taken as the time of diagnosis of AS, since clinic diagnosis data were not available. Since we aimed to determine the effect of the availability of the TAVR programme at the time of diagnosis on outcomes, rather than the effect of the intervention itself, this time was then used to define the era to which the patient was classified, including the pre- and post-TAVR programme era, as well as the sensitivity analysis subgroups (figure 1).

Flow chart for patient selection, exclusion and grouping. AV, aortic valve; AS, aortic stenosis; SA, South Australia; TAVR, transcatheter aortic valve replacement.
The cardiothoracic surgery database and the TAVR database were then reviewed over the same time period to determine whether an intervention in this population had occurred. All patients included in this analysis who underwent intervention had echocardiography data in the database.
Baseline demographics, comorbidities and outcomes
Baseline demographics, comorbidities and outcomes for this population were determined using the International Classification of Diseases, 10th Revision, Australian Modified (ICD-10 AM) diagnostic classification codes in the Integrated South Australian Activity Collection (ISAAC) database as well as from the department of Births, Deaths and Marriages and the Clinical Reporting Repository databases. Renal function was recorded using biochemistry results in the ISAAC database and was estimated using the Modification of Diet for Renal Disease formula for the glomerular filtration rate (GFR). Body mass index (BMI) was calculated using height and weight data in the echocardiography database. All comorbidity data, including renal function, were defined as having a prior diagnosis of the comorbidity in question using ICD-10 AM codes from the time of the inclusion echocardiogram, to exclude comorbidities which developed after the echocardiographic diagnosis of AS. Data linkage was performed between these and the echocardiographic database in a deidentified and confidential manner by an experienced data manager. Patients were excluded from the analysis if they had no SA Health data for linkage to the echocardiography database (figure 1). The Human Research Ethics Committee of the South Australian Department of Health approved this study, and all aspects comply with the Declaration of Helsinki.
The TAVR programme
The TAVR programme is defined as an MDHT discussion with the availability of TAVR as an intervention option. The MDHT at Flinders Medical Centre was introduced with TAVR in late 2008 to provide a streamlined process for the selection and periprocedural investigation of potential TAVR candidates. Patients are referred to the MDHT by a structural heart disease specialist who, in turn, takes referrals from both cardiac and non-cardiac medical practitioners and reviews initial results and organises subsequent investigations. The MDHT consists of one or two operating structural heart specialists trained in TAVR, one or two cardiothoracic surgeons, one or two non-interventional cardiologists specialising in heart failure (HF)/imaging/cardiogeriatrics, one or two vascular surgeons, a radiologist specialising in structural cardiac imaging, one or two cardiac anaesthetists, fellows, and nursing staff. While not every patient with severe AS will be discussed at the MDHT, all TAVR and most complex SAVR cases are included. Cases that are clearly for continued medical management due to no symptoms or extreme risk as well as patients considered low risk for SAVR are often not discussed as the added expertise of the MDHT is not required. Cases are discussed biweekly with a review of the relevant history, comorbidities and investigations. A consensus is sought regarding the appropriateness of intervention, the intervention modality, the access site and the time frame. A decision can also be made to continue medical management and observe or to seek additional information.
Analysis
Categorical variables were reported as frequencies and proportions. Baseline characteristics were compared using Pearson’s χ2 test for categorical variables and analysis of variance or Mann-Whitney-Wilcoxon for continuous variables, where appropriate. Given the age and comorbidity of the cohort, the outcome of interest for this analysis was time to death from any cause from the date of the first echocardiographic diagnosis of AS.
Mortality was reviewed in our cohort of patients with severe AS. A comparison Kaplan-Meier curve for the general population was derived using age-specific and sex-specific life expectancies from the Australian Bureau of Statistics Life Table Data and the application of these data to our population to determine an expected time of death.
Comparison was then made between groups in the time period prior to the introduction of the TAVR programme in late 2008 and the post-TAVR programme era. The pre-TAVR programme era was therefore defined as before 1 January 2009, and the post-TAVR programme era was defined as after 1 January 2009. Differences in the baseline characteristics were examined between the pre- and post-TAVR programme eras, including age, sex, BMI, left ventricular (LV) dysfunction, renal dysfunction, liver dysfunction, diabetes mellitus, hypertension (HTN), chronic obstructive pulmonary disease (COPD), prior history of HF, acute coronary syndrome (ACS), cerebrovascular accident (CVA), cancer, dementia and prior coronary artery bypass grafting (CABG). Differences in severity of AS using the echocardiographic markers of AS were also compared, as well as the number of qualifying markers of severe AS.
These clinical and echocardiographic variables were then used to develop and validate the inverse probability weighted (IPW) cohorts based on the probability of ‘presenting’ in either of the eras. Specifically, using baseline clinical and echocardiographic characteristics, the propensity for AS diagnosis within the pre- or post-TAVR programme era was modelled in a logistic regression model and the cohort was weighted for the inverse of the probability for being diagnosed within the specific eras. Assessment of the balance of these two populations by key clinical variables associated with survival was carried out by standardised errors. This reweighted population was used to assess survival. Unadjusted Kaplan-Meier estimates of 5-year survival demonstrates a non-proportional difference in the survival differences related to the era of care, and therefore a flexible parametric approach was used, where the relative hazards for the TAVR programme era were allowed to vary over time. To further ensure adjustment for the key prognostic variables of age; gender; LV function; GFR; and prior histories of HF, HTN, ACS, CVA, dementia, COPD, diabetes, liver disease, cancer and CABG, these were also entered together with the era in the final model using the IPW cohort.
We then adjusted for the presence of intervention to account for the effect of the expansion of intervention by TAVR to include patients previously considered too high-risk for SAVR. We were then able to determine if between-era differences other than intervention and comorbidities led to a difference in survival. Any remaining difference in outcome between eras is presumed to be related to the MDHT itself, which is the only other significant management change between eras.
As a sensitivity analysis, to explore the impact of the evolving MDHT and operator proficiency, a transition period was defined as all diagnoses of AS made in 2009. Furthermore, two subgroups of the post-TAVR programme era, the early and late sub-eras were defined as between 1 January 2010 and 31 December 2013 and 1 January 2014 and 31 December 2016, respectively. To explore whether or not evolving MDHT proficiency impacted the outcomes, the transition period was excluded. Furthermore, comparison was made between the subgroups of the post-TAVR programme era to determine whether improvements in operator experience or technology continued to improve outcomes after the introduction of the TAVR programme.
All reported p-values were two-sided, and statistical significance was set at p<0.05. Statistical analysis was undertaken using STATA MP 14 (Stata, College Station, Texas, USA).
Results
Patient characteristics
Within the study period, 104 928 patients had 190 670 echocardiograms. In total, 3478 patients were identified as having severe AS using the above criteria. Seventy-seven observations were removed due to having no SA Health data available for linkage. Two patients were excluded due to not meeting probable severe AS criteria after removing clearly erroneous data. After exclusions, there were 3399 patients available for analysis (figure 1).
The median number of AS severity factors was two markers per patient in both the intervention and medical groups, with a mean of 2.49 (SD=1.14) in the intervention group and 1.85 (SD=1.00) in the medically managed group (p<0.001). The median time from diagnosis to TAVR was 238 days, and to SAVR was 127 days. The population baseline characteristics, including number of AS factors, are included in table 1.
Baseline characteristics of patients with severe AS, with comparisons of characteristics prior and subsequent to the era defined by the MDHT
Survival of population with AS relative to general population
Long-term observed mortality in our population was high. Of the 3399 patients, there were 210 deaths (6.2%) at 30 days and 511 deaths (15.0%) at 6 months. By 1-year and 5-year follow-up, 722 (21.2%) and 1614 (47.5%) were deceased. The overall survival data, as well as survival data according to management strategy are presented in table 2.
Unadjusted mortality in a population of patients with severe AS between 2006 and 2016, with a comparison of mortality stratified by intervention strategy
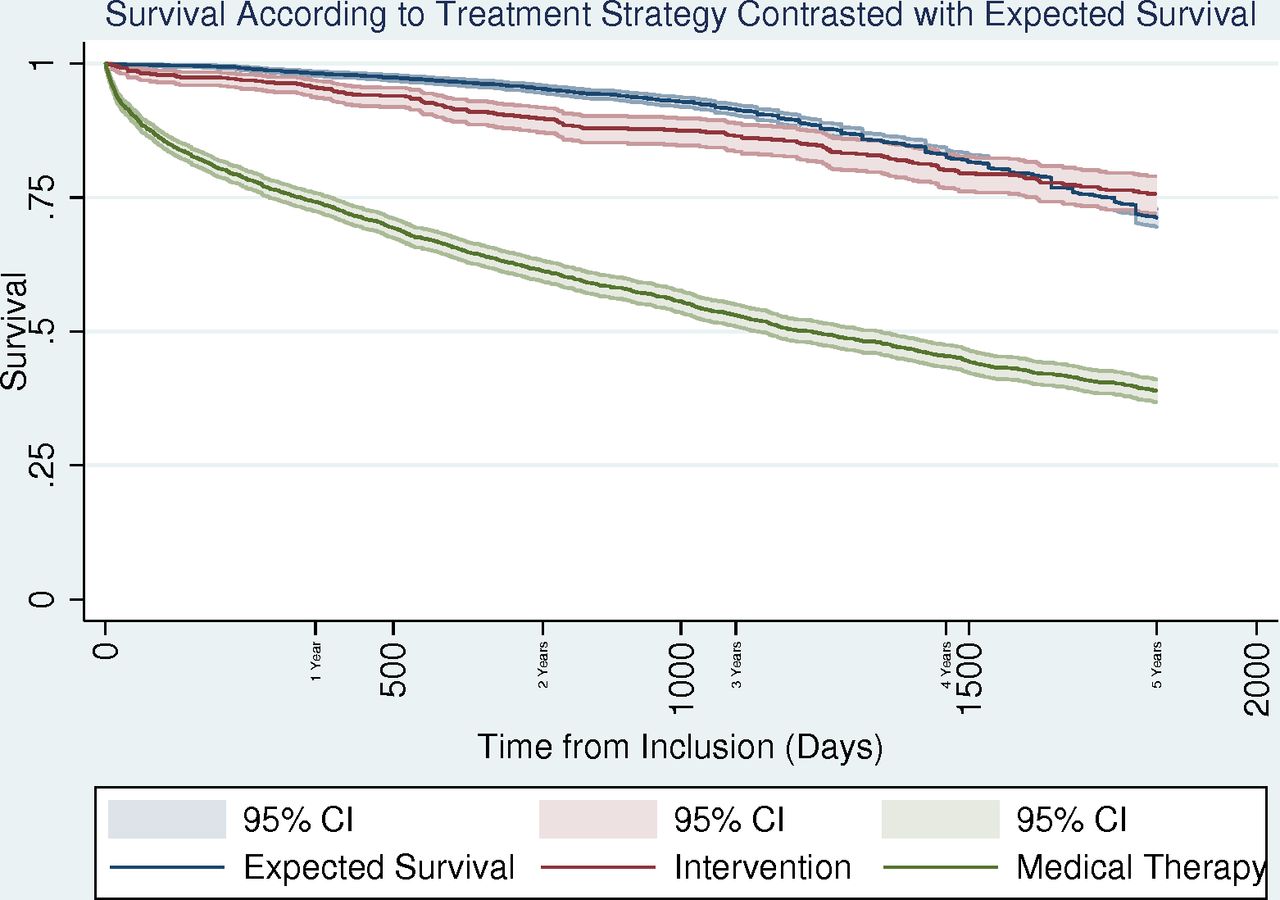
To explore mortality in the population with AS in the modern era, we contrasted our population with severe AS with expected survival in an age-matched and gender-matched general population in SA. It was observed that the population with severe AS appeared to die prematurely. Patients receiving intervention with SAVR or TAVR were much more likely to survive than those treated with medical therapy (figure 2).
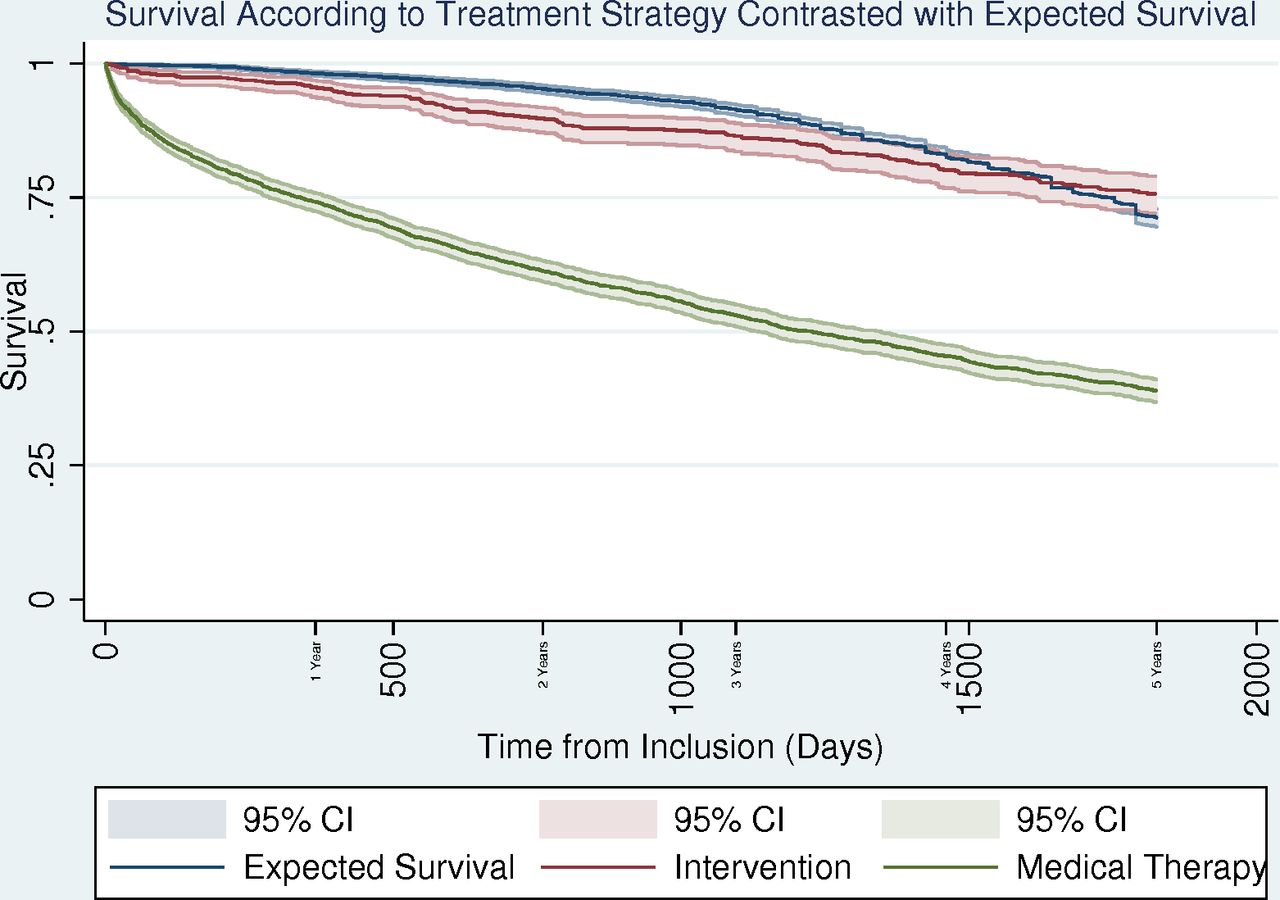
Expected 5-year survival of an age-matched and gender-matched general population according to Australian Bureau of Statistics life tables, contrasted with the observed 5-year survival in the population with aortic stenosis stratified by treatment strategy.
Population characteristics by era
There were 999 patients diagnosed with AS in the pre-TAVR programme era and 2400 in the post-TAVR programme era. Significant differences are noted between eras (table 1). Patients diagnosed with severe AS after the introduction of the TAVR programme were older, more likely to be male and had a higher GFR. Although a lower proportion of patients had severe LV dysfunction in the post-TAVR programme era, overall ejection fraction was lower. AS severity was worse in the post-TAVR programme era, but patients were less likely to have a previous diagnosis of HF, ACS and COPD.
Among the 705 patients undergoing intervention between 2006 and 2016 inclusive, those in the post-TAVR programme era were older, with a lower ejection fraction and more severe AS. There were no significant differences in the rates of analysed comorbidities (table 3).
Baseline characteristics between eras in patients undergoing intervention for severe AS
The number of patients identified with severe AS by echocardiography per year is outlined in table 4. The number of patients diagnosed within a given year who are eventually treated with intervention is also included, rather than the year of intervention itself, to better model the outcomes related to presenting in a specific era. The total number of interventions per year were not significantly different, but there was a notable shift in intervention modality from SAVR to TAVR over time.
Rate of diagnosis of AS per year, with the number and proportion of patients diagnosed in each year going on to eventual intervention and the intervention modality
Effect of the post-TAVR programme era
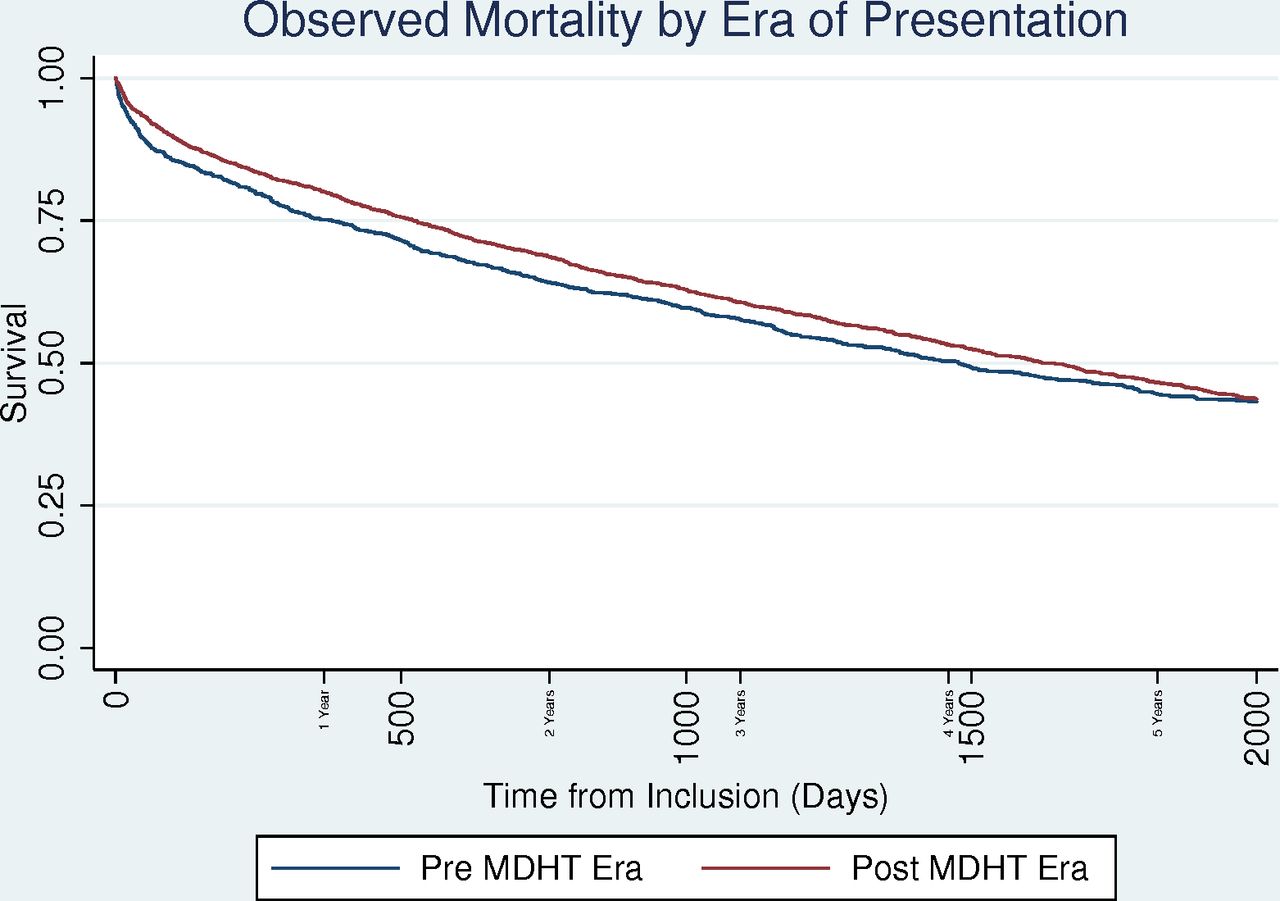
The unadjusted mortality in patients prior and subsequent to the introduction of the TAVR programme was not significantly different at 5 years although an early separation in the mortality curves was noted (figure 3). After IPW, the eras were balanced on key clinical characteristics (online supplementary table 1). Using this flexible parametric model, a significant benefit was noted with the post-TAVR programme era (HR=0.86, 95% CI 0.77 to 0.97, p=0.015). With age, comorbidities and AS severity in the model, this association was more prominent (HR=0.82, 95% CI 0.73 to 0.92, p=0.001).
Supplemental material
{kind=link}
{kind=link}
{kind=link}
Observed 5-year survival in the population with AS stratified by era of presentation. AS, aortic stenosis; MDHT, multidisciplinary heart team.
When the provision of AV intervention, by SAVR or TAVR, in addition to age, comorbidities and valve severity was included in the model, the era-associated benefit persisted (HR=0.84, 95% CI 0.75 to 0.95, p=0.004). No significant mortality difference was noted between SAVR and TAVR treated patients (HR=1.43, 95% CI 0.89 to 2.30, p=0.141).
Sensitivity analyses
For the sensitivity analyses, a further 379 patients were excluded from the survival analysis due to presenting in the TAVR transition era, defined as a diagnosis within the first year of the programme, 2009. Excluding the transition period yielded virtually identical results, and therefore this period was included in the main analysis. The early and late post-TAVR programme subgroups were similar in baseline characteristics, and no differences in outcomes were found between groups in a similarly adjusted IPW analysis (HR=1.09, 95% CI 0.93 to 1.28, p=0.276) and when adjusting for the presence of intervention (HR=1.09, 95% CI 0.93 to 1.27, p=0.305).
Discussion
Improvement in outcomes
Our results suggest that the availability of a TAVR programme significantly impacts mortality in a population of patients with severe AS, independently of the increased access to AV intervention using TAVR or SAVR.
Although patients diagnosed with severe AS after the implementation of the TAVR programme were generally less comorbid, the patient population treated by intervention was older with significantly poorer cardiac function, which suggests that the less invasive nature of TAVR led to an expansion in the treatment population to include those patients previously considered inoperable or high risk for a SAVR. It is well documented, including with our own results, that treatment of severe AS leads to a significant mortality benefit in this population,8 and that improvements in technology which expand the treated population lead to an overall benefit in the population with severe AS as a whole. In line with the PARTNER data,8 when adjusting for age and comorbidities, our population had no significant difference in mortality between SAVR and TAVR, indicating the noted difference in mortality between eras cannot be attributed to the implementation of a novel therapy with regional patterns of outcomes better than the published data.
Benefit of the MDHT and potential mechanisms
Although the implementation of the TAVR programme led to a population-wide benefit, at least partially due to the expansion of access to intervention, there remained a significant mortality benefit in the post-TAVR programme era, even when adjusting for the expansion of intervention. We propose this may be due to the MDHT itself.
Potential mechanisms for this benefit include an improvement in patient selection for intervention, the improved use of diagnostic tools, reduced loss of follow-up, improved procedure, device and access modality selection, and reduced access complications or other potential periprocedural hazards. While not every patient with severe AS needs to be discussed in the MDHT, the availability of the MDHT since the implementation of TAVR is potentially a powerful tool at the disposal of the treating cardiologist, and we propose that potentially it is the availability of such an expert panel when required, rather than the review itself which could improve survival outcomes.
There are likely additional benefits of MDHT involvement apart from improving procedural outcomes, such as improving timelines and consistency of therapy, more complete therapies and improvements in patient knowledge and satisfaction.12
Improvement in technology and experience over time
We considered that the improvement in outcomes could be related to improved operator experience or improved device technology. At Flinders Medical Centre, there was a single operator for the entire study period, so no interoperator differences were contributory. We performed a subgroup analysis splitting the post-TAVR era subgroup into roughly equal early and late TAVR period groups, with the late TAVR era group the recipients of a more experienced operator and the latest valve technology. We found that the mortality benefit seen after the implementation of the TAVR programme occurred at the time of this implementation and then remained relatively static, with no continued improvement in mortality seen between the post-TAVR subgroups, suggesting that operator experience or improvements in technology were unlikely to contribute significantly.
Limitations
While our observational data cannot directly attribute the demonstrated improved survival to the MDHT in a causal manner, we were unable to offer any other significant inter-era alterations in the protocol as an explanation for these results, although unmeasured confounders may exist. The limitations of our data did not allow accurate comment on changing periprocedural complication rates over time, in particular due to improvements in operator experience or device technology, and so only mortality data were reported. Surgical risk scores such as the STS Score or the EuroScore were also unavailable for our population. While a formal MDHT may not have existed prior to TAVR, informal collegial discussion between cardiologists and cardiothoracic surgeons have been present for decades, although without the additional medical and surgical specialties of the current programme. There was also a relatively short duration of the pre-TAVR programme era included in the analysis due to the limitations of electronic data capture in the echocardiography database.
Conclusions
The involvement of an MDHT in a TAVR programme is a class 1C recommendation from both American and European societies as a central concept of AS management, but as far as we are aware, no prior data exist supporting its efficacy.24 Our data suggest that the addition of TAVR to the long-standing surgical programme for the management of AS along with a functional MDHT is associated with a mortality benefit in the population with severe AS. Even when adjusting for the expansion of the intervention population, a significant mortality benefit remains, possibly due to the MDHT itself, supporting the use of this collaborative method despite the increased organisational difficulty and cost.
References
Footnotes
Contributors DRJ is the primary author and researcher for the manuscript. DPC, SJL, JSB and JB are PhD co-supervisors and contributed to the review and accuracy of the manuscript. DPC, assisted by AM-YC assisted with the statistical analysis. MJH is the data manager responsible for the extraction and linkage of the various databases. ARS, MXJ and RAB are the custodians for the TAVR, echocardiography and Cardiothoracic Suregery Unit (CTSU) databases, respectively. All coauthors reviewed the final manuscript and approved submission.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests DRJ received a Flinders University Research Scholarship to assist with his PhD studies.
Patient consent for publication Not required.
Ethics approval The Human Research Ethics Committee of the South Australian Department of Health approved this study (approval number: HREC/17/SAC/79).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement No additional data are available.