Article Text

Abstract
Neuroendocrine neoplasms arise from the gastrointestinal tract and can lead to carcinoid syndrome. Carcinoid heart disease affects more than half of these patients and is the initial presentation of carcinoid syndrome in up to 20 % of patients. Carcinoid heart disease typically leads to valve dysfunction, but in rare instances, carcinoid tumours can also metastasise to the endocardium and myocardium. Cardiovascular imaging plays an integral role in the diagnosis and prognosis of carcinoid heart disease. The use of multimodality imaging techniques including echocardiography, cardiac MRI, cardiovascular CT and positron emission tomography have allowed for a more comprehensive assessment of carcinoid heart disease. In this review, we discuss the features of carcinoid heart disease observed on multimodality imaging, indications for obtaining imaging studies and their role in carcinoid heart disease management.
- tricuspid valve disease
- cardiac remodelling
- echocardiography
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Neuroendocrine neoplasms most often arise in the midgut or bronchial system. These neoplasms can secrete vasoactive substances such as serotonin and produce symptoms including diarrhoea, hypotension and bronchospasm.1 This constellation of symptoms is known as carcinoid syndrome. Carcinoid heart disease (CHD) is the initial presentation in up to 20% of patients with carcinoid syndrome2 and affects over half of those with carcinoid syndrome.3 If neuroendocrine neoplasms metastasise to the liver, large amounts of vasoactive substances can eventually reach the right side of the heart, leading to fibrous deposition predominantly affecting the tricuspid and pulmonic valves.4 These vasoactive substances are metabolised in the pulmonary circulation and only infrequently reach the left side of the heart in active form; therefore, CHD is classically associated with right sided valve dysfunction and its sequelae.4 However, left-sided valvular pathology can also occur in patients and is associated with right-to-left shunting (ie, patent foramen ovale (PFO)), bronchial carcinoid or poorly controlled carcinoid syndrome.5 Furthermore, neuroendocrine neoplasms can infrequently metastasise and infiltrate the endocardium and myocardium.6
Cardiovascular imaging plays an integral role in the diagnosis and prognosis of CHD. Recent advancements in echocardiography, cardiac magnetic resonance imaging (CMR), cardiovascular CT (CCT) and positron emission tomography (PET) have allowed for a more thorough assessment of CHD. This review will discuss the prominent features of CHD noted on multimodality imaging, indications for obtaining these various tests and their utility in CHD management.
Echocardiography
Two-dimensional transthoracic echocardiography (2D TTE)
2D TTE in CHD often reveals thickening of the tricuspid and pulmonic valve leaflets caused by fibrous deposition. This leads to reduced excursion of the valves, which are often noted to be moving in an abnormal ‘board-like’ pattern.7 This impaired mobility of the valves typically leads to regurgitation and/or stenosis (figure 1A and B).
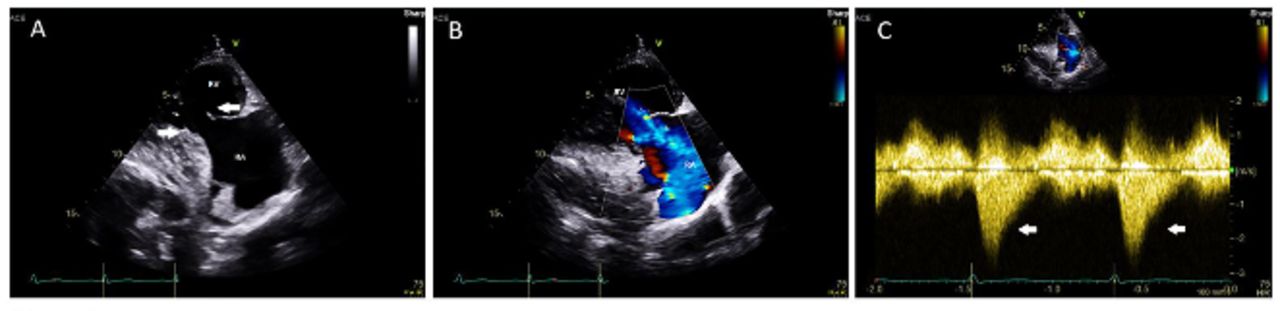
(A) Transthoracic echocardiogram of the right heart showing fixed, immobile TV (arrows) and resultant (B) severe tricuspid regurgitation. Doppler interrogation (C) reveals a characteristic ‘dagger-shaped’ (arrows) spectrum on Doppler profile (early peak pressure with a subsequent rapid decline). TV, tricuspid valve.
Valve regurgitation and stenosis in CHD is typically defined by the American Heart Association/American College of Cardiology guidelines.8 The most common valvular abnormality in CHD is tricuspid regurgitation. In a comprehensive study reviewing the echocardiograms of 74 patients with CHD, 100% of patients had tricuspid regurgitation. The presence of tricuspid regurgitation among patients with CHD typically reveals a characteristic ‘dagger-shaped’ spectrum on Doppler profile (early peak pressure rise with a subsequent rapid decline)9 (figure 1c). Furthermore, pulmonic regurgitation affected 81% of patients and pulmonic stenosis affected 53% of patients with CHD.9 The fibrous deposition in CHD can also affect chordae and papillae, worsening the functional abnormalities of the valve.10
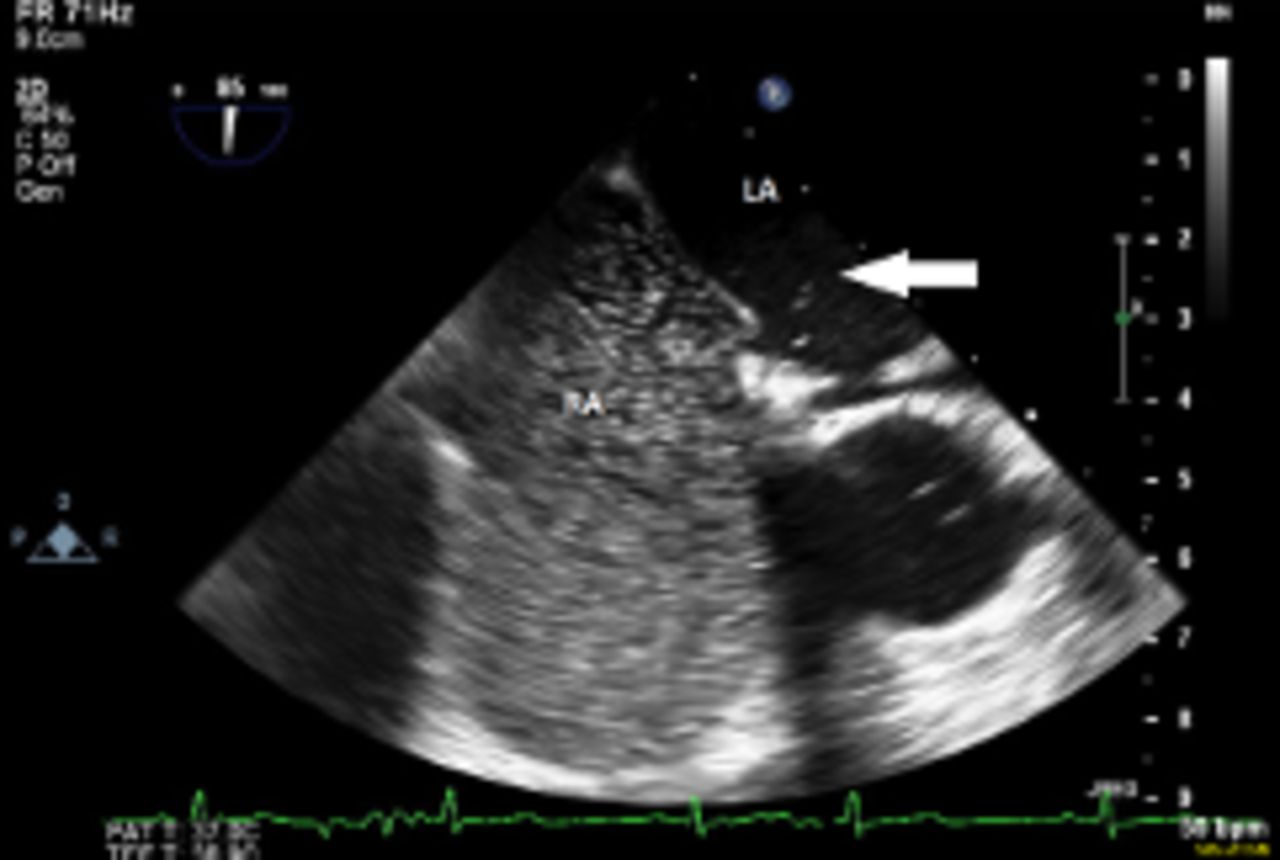
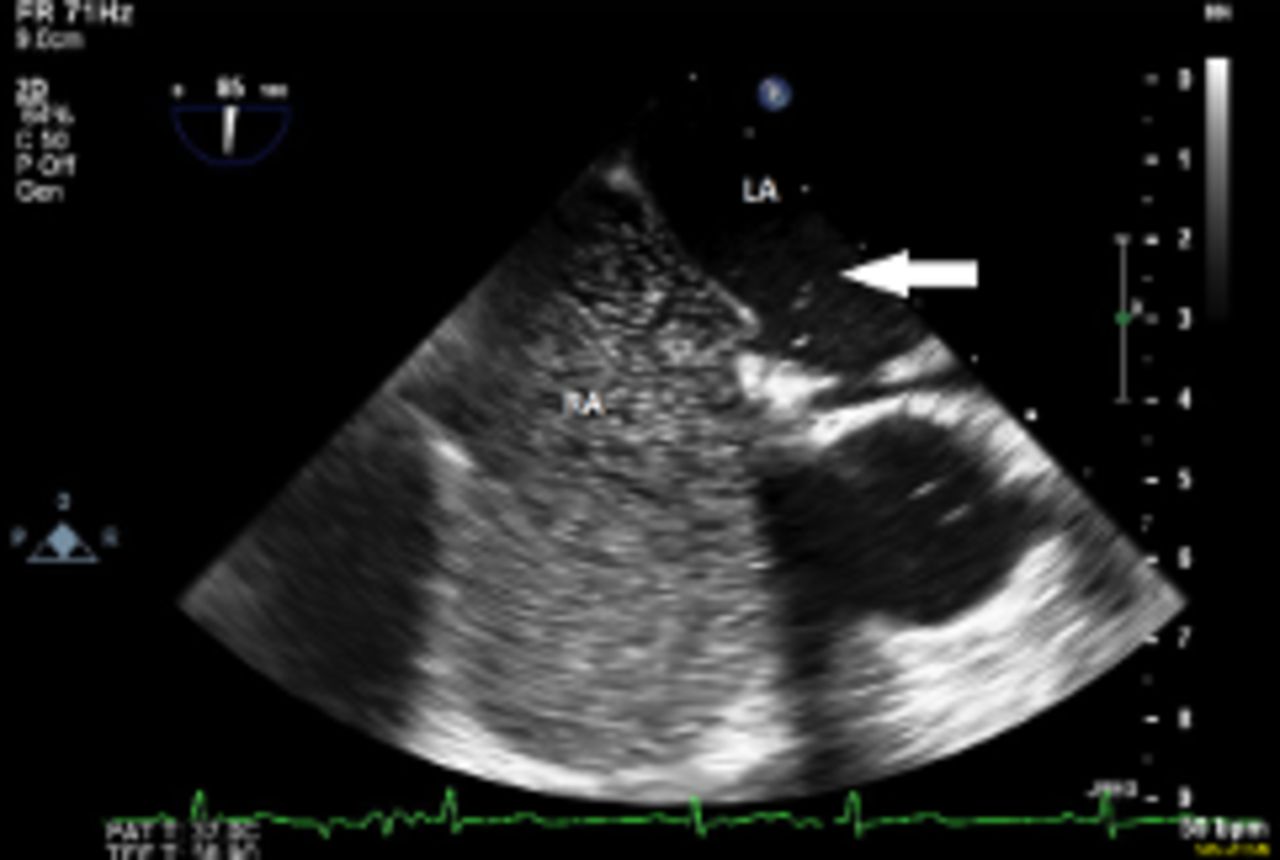
Although CHD typically affects right-sided valves, it can also affect left-sided valves in rare instances (figure 2). In the aforementioned study reviewing the echocardiograms of 74 patients with CHD, 7% of patients were noted to have left-sided involvement.9 One instance where CHD may demonstrate left-sided involvement is in the presence of a PFO, where vasoactive substances are able to bypass the lungs (where typically they are metabolised into inactive substances) and reach the left side of the heart.11 Alternatively, a primary neuroendocrine neoplasm affecting the lung may also lead to left-sided CHD. Lastly, a high disease burden can also cause left-sided CHD, as large amounts of vasoactive substances produced by the neoplasm(s) cannot be fully metabolised into inactive substances in lungs.12 An echocardiogram can be performed with ‘microbubble’ contrast in order to assess for the presence of a PFO (figure 3).

Transthoracic echocardiogram showing thickening of the mitral valve (arrowheads) in a patient with left-sided carcinoid heart disease. LA, left atrium; LV, left ventricle.
Transoesophageal echocardiogram performed with ‘microbubble’ contrast in order to assess for the presence of a right to left interatrial shunt (arrow showing bubbles on the left side of the heart). LA, left atrium; RA, right atrium.
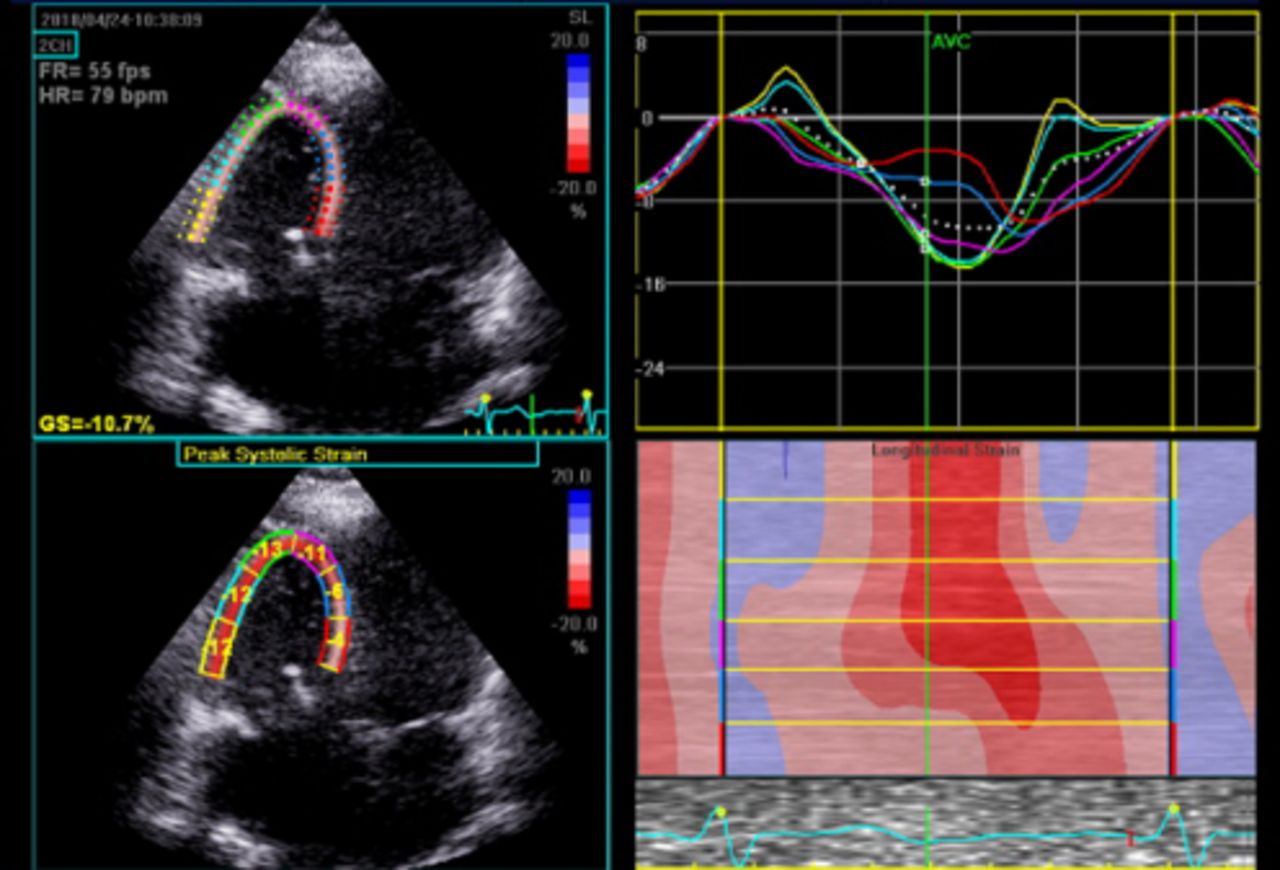
In addition to valvular abnormalities, CHD can also affect ventricular strain (figure 4). In one study, right ventricular (RV) strain was reduced in patients with CHD relative to controls (a mean of −20.6 compared with −26.9, respectively). Furthermore, RV strain was similar among patients with carcinoid syndrome regardless of whether they had obvious valvular involvement, suggesting that abnormal RV strain may be a sensitive and early indicator of CHD before the development of obvious valvular abnormalities.13 In addition to RV strain, global left ventricular (LV) strain is also slightly reduced among patients with CHD compared with healthy individuals. Furthermore, among patients with carcinoid syndrome, there was no difference in myocardial LV strain between those with and without overt CHD (ie, valvular abnormalities).13

Myocardial strain with region of interest over entire RV in the RV focused view in a patient with severe RV enlargement and carcinoid heart disease. Note average RV lateral wall strain was −10.7 (normal −26.9%±4.4%). Two-dimensional speckle tracking analysis was performed using the vendor apical two-chamber view region of interest. RV, right ventricle.
In addition to valvular abnormalities and alterations in ventricular strain, neuroendocrine neoplasms can actually metastasise to the myocardium in rare instances. 2D TTE allows for the identification of larger masses, but masses less than 1 cm in diameter may be difficult to visualise using two-dimensional echocardiography. Also, it may be difficult to distinguish their borders from surrounding structures on TTE, making it impossible to estimate the actual dimensions of the mass or fully appreciate its mass effects.7
Three-dimensional transthoracic echocardiography (3D TTE)
In comparison with 2D TTE, 3D TTE offers a few distinct advantages (figure 5). With respect to the tricuspid valve, 3D TTE allows for visualisation of all valve leaflets at the same time. This allows 3D TTE to be more sensitive for the identification of CHD, as some cases only involve a single leaflet.7 14 Single-leaflet involvement can lead to a moderate, eccentrically directed jet of tricuspid regurgitation.7 3D TTE also allows for a detailed view of subvalvular structures, such as chordae and papillary muscles, which can become involved by carcinoid ‘plaque’.7 With respect to the pulmonary valve, 3D TTE once again allows for simultaneous assessment of all valve leaflets at the same time. In severe cases, 3D TTE can also identify deformities of surrounding structures, such as poststenotic dilatation of the pulmonary artery.7

Three-dmensional image from the ventricular projection during systole showing closure of neighbouring mV (arrow), while TV remains fully open (arrowhead) due to severe TV leaflet retraction. MV, mitral valve; TV, tricuspid valve.
Also, 3D TTE may better allow for operative planning in patients who may benefit from surgical valve repair. 3D TTE also allows for the identification of metastasis to the myocardium in CHD with improved ability to distinguish their borders from surrounding structures compared with 2D TTE, allowing for a more accurate estimation of the actual dimensions and mass effects.7
Transoesophageal echocardiography (TOE)
TOE may be useful when TTE does not clearly identify valvular abnormalities. In particular, TOE allows for improved visualisation of the pulmonic valve in comparison with TTE15 and may elucidate subtle abnormalities with the tricuspid valve when TTE is equivocal. In particular, the superior spatial resolution of real time three-dimensional TOE (3D TOE) can help determine which patients require valve replacement and can also prove very useful in preoperative planning.16 Lastly, there is at least one example where TOE was used to identify an intramyocardial metastatic neuroendocrine neoplasm.17
Indications for echocardiography
According to an expert statement by the American College of Cardiology regarding the diagnosis and management of CHD, an echocardiogram should be obtained in all patients with carcinoid syndrome and high suspicion for CHD. In patients with known CHD, an echocardiogram should be repeated every 3–6 months or when a change in clinical status is observed.18 In contrast, the European Neuroendocrine Tumor Society (ENETS) guidelines recommend performing TTE annually among patients with known CHD.19
The portability, relatively low cost, lack of radiation and real-time haemodynamic/valvular assessment provided by echocardiography make it the test of choice for initial evaluation of CHD. However, echocardiography is not without its limitations; image quality may be limited by poor acoustic windows, and spatial resolution is limited compared with other techniques.
Although echocardiogram is the preferred initial test in the evaluation of suspected CHD, it should be performed judiciously among patients with carcinoid syndrome. In a study evaluating 200 patients with a neuroendocrine neoplasm originating in the midgut and a history of carcinoid syndrome, 19.5% of patients had evidence of CHD. However, when only screening patients with an -N-terminal pro B-type natriuretic peptide >260 pg/mL, the number of patients needed to screen with echocardiogram to diagnose one case of CHD decreased from 5.1 to 1.4.20 This suggests that elevated cardiac biomarkers may allow physicians to determine when echocardiogram is an appropriate screening test for diagnosis of CHD. Furthermore, ENETS guidelines suggest screening patients with carcinoid syndrome using TTE if they have significantly elevated 5-hydroxyindoleacetic acid levels.19
Application of echocardiographic findings
The constellation of findings on echocardiography can be used to assess the severity of CHD. Multiple scoring systems based on echocardiographic findings have been proposed, with the first (and perhaps the most recognised) scoring system based on tricuspid valve anatomy, tricuspid regurgitation severity, pulmonic stenosis severity and pulmonic insufficiency severity.21 Many of these scoring systems have been demonstrated to correlate with disease activity (5-HIAA levels) and cardiac biomarkers (NT-proBNP). Although more complex scoring systems may be more challenging and time consuming to implement, they may better allow for the monitoring of disease progression.22
Cardiac magnetic resonance
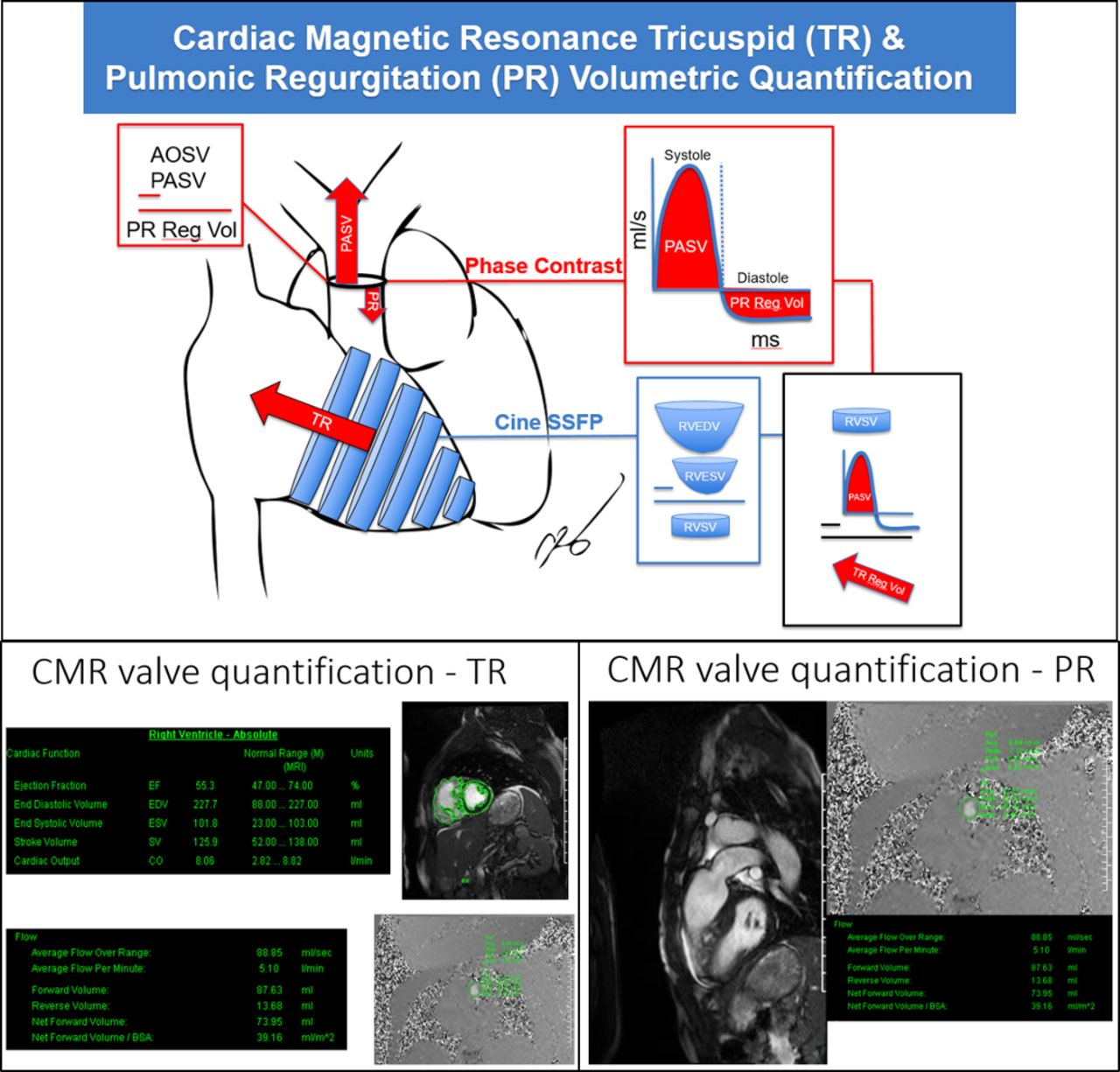
CMR is emerging as a prominent modality to identify CHD, especially when echocardiographic findings are equivocal.23 In particular, CMR is useful in detecting CHD when echocardiogram cannot provide adequate views of the pulmonic valve.7 With respect to estimating regurgitant volume, CMR has also been demonstrated to be more accurate than echocardiography24 (figure 6). Additionally, when valvular abnormalities are not obvious on echocardiography, late gadolinium enhancement of the tricuspid and/or pulmonic valves may provide evidence of CHD.25 However, this finding is not specific and may be seen in other cardiovascular diseases.

Pictorial representation of quantification of valvular regurgitation done by CMR, along with example calculation of volumetric quantification of regurgitation across the pulmonic and tricuspid valves. CMR, cardiac magnetic resonance.
In addition to better quantifying the degree of valvular dysfunction, CMR can also provide a more accurate assessment of chamber sizes in CHD, compared with echocardiography.26 This is essential, because in order to understand the severity of CHD, it is important to appreciate valvular abnormalities (such as tricuspid regurgitation) and the consequences of these valvular abnormalities (such as abnormal RV size or function as a consequence of tricuspid regurgitation). CMR provides a better estimate of RV size and function with less interobserver variability, compared with echocardiography27
Additionally, CMR more readily allows for the identification of infrequent metastatic spread of neuroendocrine neoplasm to the myocardium.7 Compared with echocardiography, CMR has the advantage of added spatial resolution that may lead to improved characterisation of an intracardiac carcinoid mass. Lastly, CMR also allows for the identification of neuroendocrine neoplasm metastasis to surrounding extracardiac structures.7 It is important to note that CMR also has some disadvantages, including increased cost in comparison with echocardiography and the need to potentially use contrast.
Cardiovascular CT
CCT may also play a role in the identification of CHD. In particular, CCT may have great utility in operative planning. It allows for measurement of RV dimensions.28 CCT also allows for the assessment of the degree of valvular damage, especially when heavy calcification is present.18
CCT allows for the unique advantage of being able to visualise the coronary arteries and determine if there is any haemodynamically significant stenosis that may confound the clinical presentation of CHD, which often includes shortness of breath and dyspnoea on exertion. Furthermore, CCT allows one to determine the proximity of the myocardial involvement to the coronary arteries, which is essential during operative planning. Postoperatively, it can be useful in assessing pulmonic prosthetic valve thrombosis (figure 7). Disadvantages of CCT include radiation exposure in addition to possible contrast exposure.
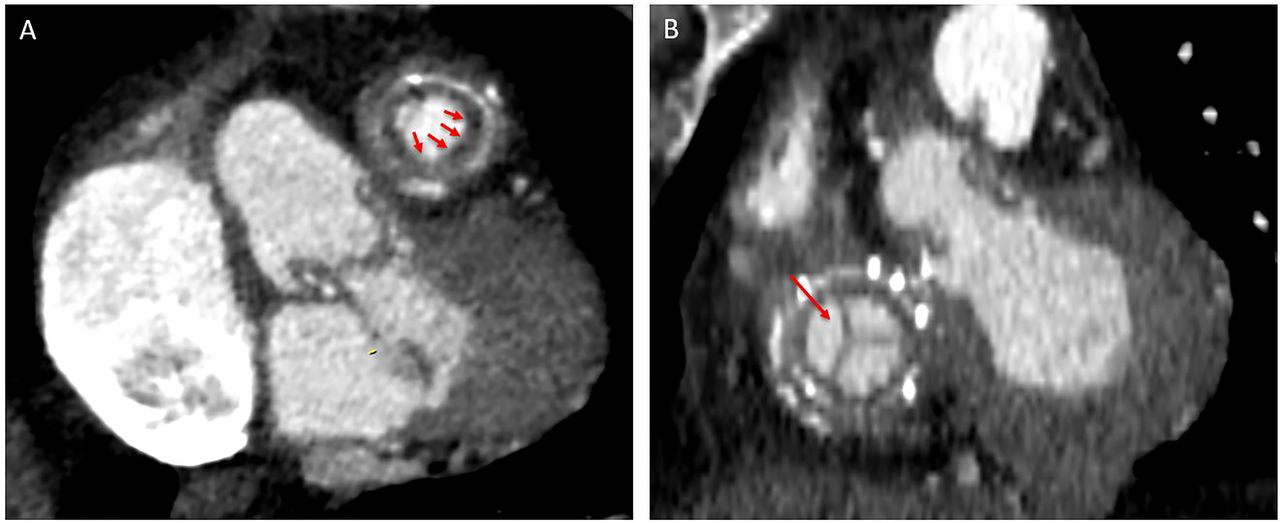
CCT of pulmonic prosthesis showing crescent shaped thrombus (red arrows) that obstructs the outflow (A) along with well seated normal functioning tricuspid valve prosthesis (red arrow) in the same patient (B). CCT, cardiovascular CT.
Positron emission tomography
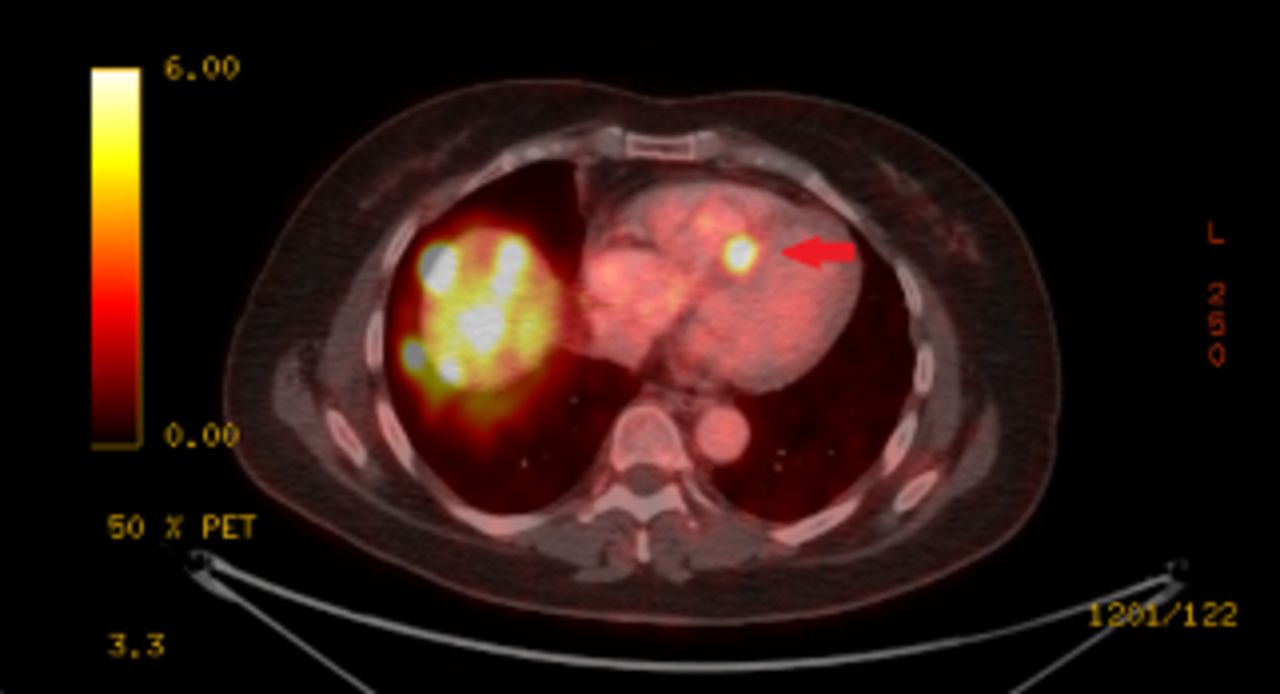
A hallmark of neuroendocrine neoplasms is their increased density of somatostatin receptors. PET takes advantage of this unique feature, as somatostatin analogues labelled with radioactive substances (typically Gallium-68) are avidly taken up by neuroendocrine neoplasms and are easily identifiable on PET scans.22 This is useful for identifying myocardial metastasis in CHD (figure 8). This method has been validated to be >97% sensitive and 92% specific for the identification of metastatic neuroendocrine neoplasms.29 Although potentially useful, PET is rarely employed in this setting because of its high cost and limited availability.
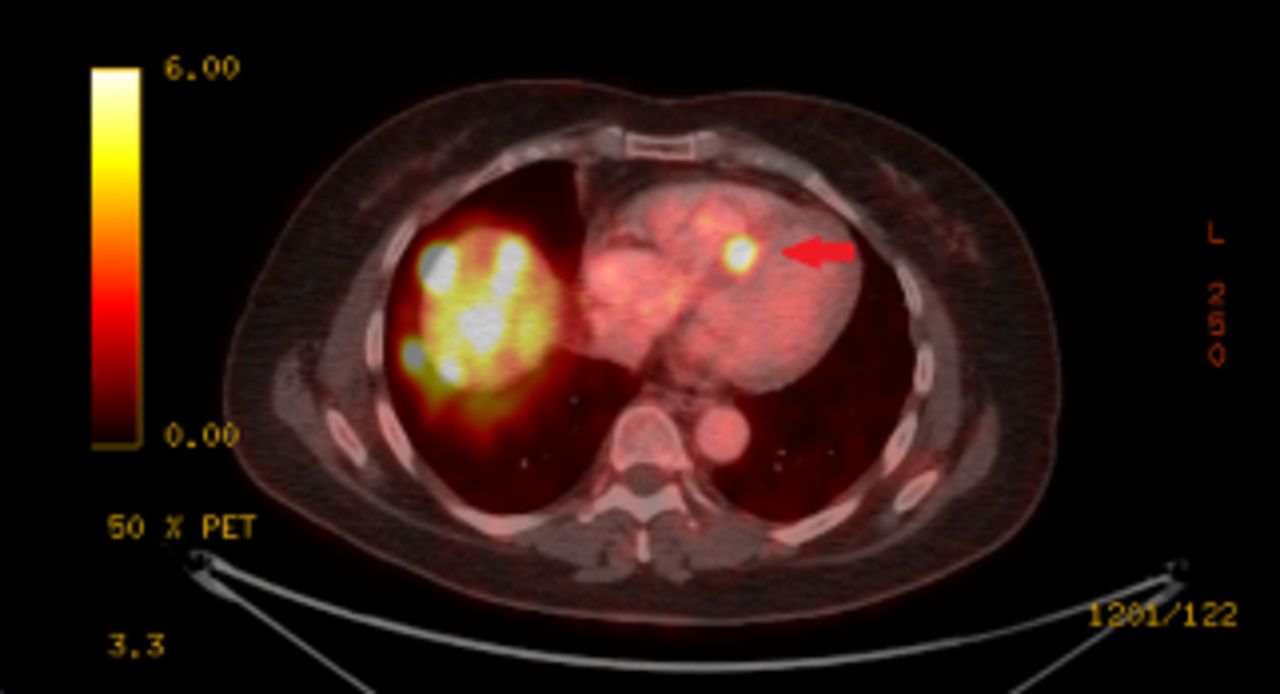
Gallium 68-DOTATATE PET-CT showing cardiac metastasis of a neuroendocrine tumour by tracer avidity (red arrow). PET, positron emission tomography.
Cardiovascular imaging and surgical intervention
Patients with severe symptomatic CHD may be considered for valve replacement surgery, and surgery may be the most effective treatment option for some patients with valvular CHD.30 A 1995 study that assessed the outcome of cardiac surgery for treatment of CHD demonstrated that surgery carried a high perioperative mortality risk, but those patients who survived noted a significant improvement in symptoms.31 One decade later, another study demonstrated an improvement in perioperative mortality and a more favourable outcome after valve surgery.32
The use of multimodality imaging plays an important role in the diagnosis of CHD, and each modality has its specific advantages and limitations (table 1). Furthermore, cardiovascular imaging plays an essential function in determining which patients may be surgical candidates, preoperative planning and postoperative assessment of surgical outcome. Echocardiography can help identify severe valvular abnormalities (most commonly tricuspid regurgitation), which may qualify symptomatic patients for valve replacement surgery in the setting of well-controlled systemic disease. According to the 2017 American College of Cardiology consensus statement on the diagnosis and management of CHD, preoperative planning should include an assessment of the coronary arteries with coronary angiography or coronary CT angiography, in addition to assessment of cardiac valves using TTE (possibly in addition to cardiac CT or CMR) and assessment of RV size/function using 3D TTE, CCT and/or CMR.18 Among patients with functional TR, one study demonstrated that an RV end-diastolic volume index of 164 mL/m2 served as a cut-off for predicting normal RV ejection fraction (RVEF) after surgical repair.33 Thus, CMR may be a useful tool in predicting the optimal time for surgical repair of tricuspid valves among patients with CHD and needs to be further investigated. A proposed algorithm of how to proceed with multimodality imaging is shown in figure 9.
Comparison of imaging modalities in CHD
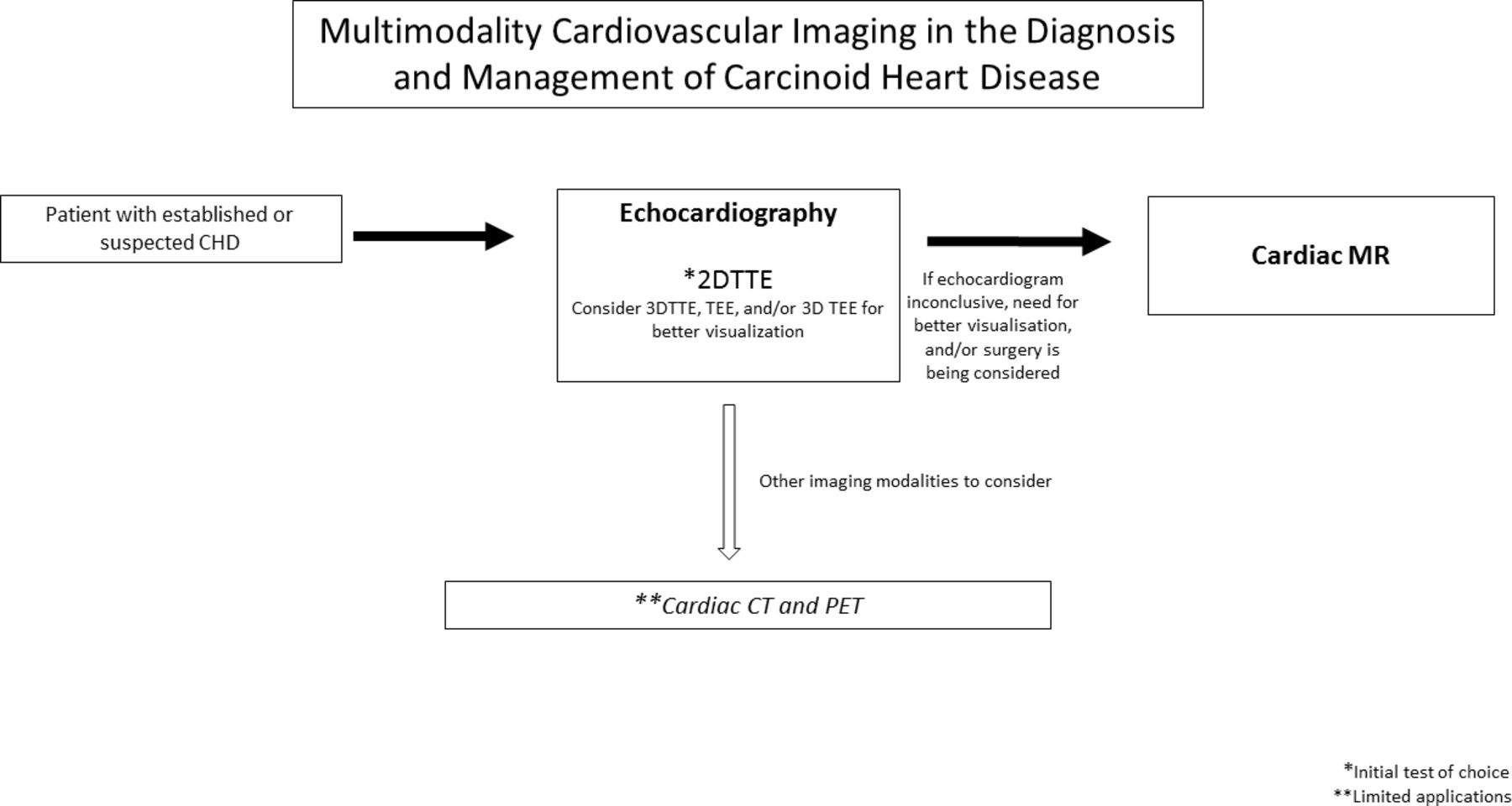
Multimodality cardiovascular imaging flow diagram in the diagnosis and management of carcinoid heart disease (CHD). 2D TTE, two-dimensional transthoracic echocardiography; 3D TTE, three-dimensional transthoracic echocardiography; PET, positron emission tomography; TOE, transoesophageal echocardiography; TTE, transthoracic echocardiogram.
Postoperatively, an echocardiogram is recommended soon after surgery, 3–6 months after cessation of anticoagulation, and then at 6–12 month intervals (figure 10).18 As previously mentioned, CMR may be more accurate than echocardiogram for estimating regurgitant volumes.24 In addition to estimating regurgitant volumes after surgical intervention, CMR can also allow for better estimation of RV volumes, LV volumes and cardiac index after repair of the tricuspid valve.33 These values may provide a more comprehensive assessment of surgical outcomes after tricuspid valve repair.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
(A) Postoperative transthoracic echocardiogram done in a patient with carcinoid heart disease with three bioprosthetic valves replacements (arrows). (B) 3D TOE in the same patient shows a well-seated tricuspid bioprosthetic valve. 3D TOE, three‐dimensional transoesophageal echocardiography; AV, aortic valve; PV, pulmonic valve; TV, tricuspid valve.
Lastly, transcatheter valve replacements are becoming increasingly common in the field of interventional cardiology and are typically preformed with the assistance of echocardiography. In fact, transcatheter pulmonic valve replacements have been performed among patients with CHD.34 35
Conclusion
CHD is a devastating sequela of carcinoid syndrome. Median survival is less than 5 years.32 However, the median survival appears to be associated with the time of diagnosis, with patients diagnosed in the 1980s having a worse prognosis than patients diagnosed in the 1990s.32 This may suggest that advancements in the diagnosis and treatment of CHD have led to improved outcomes.
Specifically, recent advancements in cardiovascular imaging, including echocardiography, MRI, CT and PET allow for a more comprehensive imaging assessment of CHD. Future advancements in cardiovascular imaging may allow for detection of CHD before patients become symptomatic and may even guide the development of cardiovascular interventions that will delay the progression or prevent CHD.
References
Footnotes
Contributors AMA and SH contributed to the planning, conducting, analysis, revision and reporting of the work described. TD, DB, CAI, JB, PYK, NLP, SY and GG engaged in conducting, analysis, revision and reporting of the work described.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information.