Article Text

Abstract
Objective Clinical data on the effect of non-steroidal anti-inflammatory drugs (NSAIDs) in myopericarditis are limited. Since NSAIDs are standard therapy in pericarditis, we retrospectively investigated their safety in myopericarditis.
Methods In a retrospective case-control study, we identified 60 patients with myopericarditis from September 2010 to August 2017. Diagnosis was based on clinical criteria, elevated high-sensitivity troponin T and cardiac magnetic resonance imaging (CMR). All patients received standard heart failure therapy if indicated. Twenty-nine patients (62%) received NSAIDs (acetylsalicylic acid: n=7, average daily dose =1300 mg or ibuprofen: n=22, average daily dose =1500 mg) for an average duration of 4 weeks. To create two cohorts with similar baseline conditions, 15 patients were excluded. Three months after diagnosis, 29 patients were re-evaluated by CMR to measure late gadolinium enhancement (LGE).
Results Baseline characteristics of those treated with or without NSAIDs were similar. Mean age was 34 (±13) years, 6 (13%) were women. Mean left ventricular ejection fraction (LVEF) was 56% (±5). 82 % of the patients (14 of 17) treated with NSAIDs experienced a decrease in LGE at 3 months, while it was only 58 % (7 of 12) of those without NSAIDs (p=0.15). At 12-month follow-up, one of the patients treated without NSAIDs experienced polymorphic ventricular tachycardia (VT) with cardiac arrest, while one of the patients with NSAIDs experienced non-sustained VT.
Conclusions This is the first case-control study demonstrating that NSAIDs are safe in patients with myopericarditis and preserved LVEF. Our data suggest that this drug class should be tested prospectively in a large randomised clinical trial.
- nonsteroidal anti-inflammatory drugs
- myocarditis
- magnetic resonance imaging
- late gadolinium enhancement
- myocardial inflammation
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- nonsteroidal anti-inflammatory drugs
- myocarditis
- magnetic resonance imaging
- late gadolinium enhancement
- myocardial inflammation
Key questions
What is already known about this subject?
Recommendations about the use of non-steroidal anti-inflammatory drugs (NSAIDs) in myopericarditis have been controversial in the literature. Since pericarditis requires anti-inflammatory treatment to prevent severe complications such as constrictive pericarditis, the involvement of the myocardium has often caused a clinical dilemma, as the recommendation for myocarditis is to avoid NSAIDs.
What does this study add?
Our retrospective case-control study shows that high-dose ibuprofen and aspirin appear to be safe in the setting of acute myopericarditis with normal left ventricular ejection fraction (LVEF). A decrease in late gadolinium enhancement (LGE) on cardiac magnetic resonance imaging after 3 months was more frequent in those patients treated with NSAIDs as compared with those not treated; however, the difference did not reach level of significance.
How might this impact on clinical practice?
NSAIDs are a valid and safe treatment option in the setting of acute myopericarditis. This finding is of high clinical relevance as prior mouse studies suggested this drug class to be associated with a higher mortality in myocarditis. Our study is the first case-control study in humans to assess the effect of NSAIDs in myocarditis on top of standard heart failure therapy. We suggest that NSAIDs should be tested prospectively for efficacy in a large randomised clinical trial.
Introduction
The treatment of myocarditis remains a clinical challenge.1–3 Current position statements recommend standard heart failure therapy and symptomatic treatment in haemodynamically stable patients with myocarditis.4 Thus, the first-line medication is standard heart failure therapy in those with markedly depressed left ventricular function.5 6 In patients with aggressive autoimmune myocarditis, such as giant cell myocarditis or eosinophilic necrotising myocarditis, a combination of high-dose steroids and cyclosporine is recommended, sometimes in combination with muronomab CD3.7–9 Non-steroidal anti-inflammatory drug (NSAID) therapy has been a cornerstone of the symptomatic therapy of uncomplicated pericarditis.10 However, experimental studies in murine models suggested that NSAIDs may deteriorate the clinical course of myocarditis.11–14 Similarly, deleterious effects such as worsening inflammation and cell necrosis,11 increased mortality,12 viral titres13 and focal ventricular thinning14 were reported in the 1980s and 1990s. Also, NSAIDs have been shown to increase blood pressure15 and may impair renal function.16
Recently, cardiac magnetic resonance imaging (CMR) has evolved as the gold standard of non-invasive diagnostic imaging in haemodynamically stable patients with myocarditis.17 18 Signs of disease activity can be found in the myocardial and pericardial layer or both leading to the term myopericarditis. Patients with myopericarditis frequently experience chest pain,19 which can be challenging to treat. Drugs with limited anti-inflammatory effects such as acetaminophen may have inadequate analgesic function, increase blood pressure20 and impair renal function21—effects that may further deteriorate left ventricular performance. To our knowledge, there have been two studies examining the effects of NSAIDs in myopericarditis.22 23 In the first study, Buiatti and colleagues investigated the management and outcome of 62 patients with myopericarditis who were treated with NSAIDs.22 Diagnosis of pericarditis was based on clinical presentation (chest pain, influenza-like symptoms weeks prior, pericardial friction rub). Myocardial involvement was defined by elevated troponin I levels or wall motion abnormalities on echocardiography. Out of 62 patients, 61 (98%) received NSAIDs as first choice. During a minimal follow-up of 1 year, there were no events of death, new onset heart failure or wall motion abnormalities on echocardiogram.22
The second study was a multicentre study using CMR in addition to standard clinical tests for the diagnosis of myopericarditis in 140 patients of an overall population of 486 cases with pericarditis with and without myocardial involvement. There were 106 patients with myocardial involvement receiving NSAID therapy. Median follow-up was 36 months with no cases of death or heart failure being reported.23y
In summary, there have been only two clinical studies investigating outcomes of patients with myopericarditis receiving NSAID therapy.22 23 Both studies suggested that this drug class could be used safely in this patient population. However, NSAIDs continue to be a grey area in the field of myopericarditis. In that regard, guidelines for myocarditis recommend to avoid this drug class,4 while guidelines for pericarditis with myocardial involvement suggest that data for NSAID use are controversial.10 Since insufficient treatment of pericarditis can be detrimental and lead to irreversible complications, there is a great need to treat the pericardial component of myopericarditis.24 25
To the best of our knowledgye, there is no literature comparing the effects of NSAIDs with standard heart failure therapy in myopericarditis and no study evaluated the effect of NSAIDs on the dynamics of late gadolinium enhancement (LGE) in myopericarditis—a major risk marker for adverse cardiovascular events.26–28
In this work, we sought to address both of these issues by performing a retrospective case-control study in patients with myopericarditis to evaluate (1) if the use of NSAIDs is safe as compared with standard heart failure therapy and (2) if NSAIDs affect the time course of LGE on CMR 3 months post diagnosis.
Methods
Patients and controls
We performed a retrospective case-control study of patients who have been diagnosed with myopericarditis at the University Hospital Zurich between September 2010 and August 2017. Myopericarditis was diagnosed in 60 patients based on clinical presentation, elevated cardiac enzymes, ECG and CMR after the exclusion of obstructive coronary artery disease by coronary angiography by cardiac catheterisation or CT.19 29 To create a homogenous cohort that only reflects acute myopericarditis, the analysis was restricted to patients with recent symptom onset (≤10 days).
In this selected group of patients with myopericarditis, we compared those who were treated with standard heart failure therapy versus those receiving NSAIDs in addition to standard heart failure therapy. The two groups were matched according to baseline criteria such as left ventricular ejection fraction (LVEF) and age. Standard heart failure therapy contained beta-blocking agents, ACE inhibitors, angiotensin II receptor blockers and diuretics. NSAIDs used in this study included acetylsalicylic acid (ASA) or ibuprofen. Patients using other types of NSAIDs such as selective cyclooxygenase-2 inhibitors or steroids were excluded to reduce possible confounding factors by creating homogenous groups. Additional exclusion criteria were malignant arrhythmias, other pre-existing cardiomyopathies and fulminant myocarditis. Evaluation of patients was performed with local ethics committee approval and written informed consent from all patients.
Clinical follow-up
Patients were scheduled for follow-up examination 3, 6 and 12 months post diagnosis of myopericarditis. Data from these visits were screened for major adverse cardiovascular events defined as worsening LVEF, malignant arrhythmias (eg, ventricular tachycardia or fibrillation), worsening of LGE on CMR, all-cause mortality and cardiovascular death. Clinical history was obtained to screen for symptoms such as severe chest pain, dyspnea or palpitations. After a complete physical examination, routine blood tests were obtained including serum creatinine to screen for deterioration in renal function under NSAID therapy. Patients underwent clinical examination including echocardiography, 12-lead ECG, 48-hour Holter monitoring and exercise stress testing with bicycle and ramp protocol.
CMR examination at baseline and at 3-month follow-up
CMR examinations were performed on a 1.5 or 3.0 Tesla scanner (SiemensSkyra, Erlangen, Germany or Philips Achieva, Best, The Netherlands) using an ECG-gated breath-hold protocol. Myopericarditis was diagnosed based on cine-CMR, T2-weighted imaging and T1-weighted LGE imaging as described previously.19 29 Ten minutes after intravenous administration of a gadolinium-based contrast agent, LGE short-axis images were generated. Routine CMR reporting included the evaluation of wall motion abnormalities and LVEF. Definition of pericardial involvement included pericardial thickening or effusion on CMR. Starting in 2016, our internal protocol also included follow-up CMR 3 months after diagnosis to identify LGE dynamic. The extent of LGE was evaluated in each slice and LGE dynamic from baseline to 3-month follow-up (increase, decrease or complete disappearance of LGE) was stated in the radiology report.
Statistical analysis
Data are presented as mean±SD. Numerical values were analysed with Wilcoxon rank sum test, and χ2 test was used for categorical values. Fisher’s exact test was used to detect differences for sparse binary data in baseline conditions. A p value <0.05 was considered statistically significant. Analyses were performed with SPSS V.23. The first authors had full access to the data and take responsibility for the integrity of data analysis.
RESULTS
Patient characteristics
To reduce the risk for potential confounding factors, we excluded patients who received other anti-inflammatory medications such as steroids (n=2) or celecoxib (n=1). Three patients had to be excluded because they met exclusion criteria. Of those, one patient presented with pre-existing dilated cardiomyopathy. The second patient was hospitalised after resuscitation due to ventricular fibrillation and the third with cardiogenic shock requiring treatment with extracorporeal membrane oxygenation in the intensive care unit. After the initial enrolment, patients without NSAID therapy were older and had lower LVEF. In order to create two groups with similar baseline conditions, another six patients were excluded due to LVEF and three patients were excluded due to age. Details of patient enrolment are illustrated in figure 1.
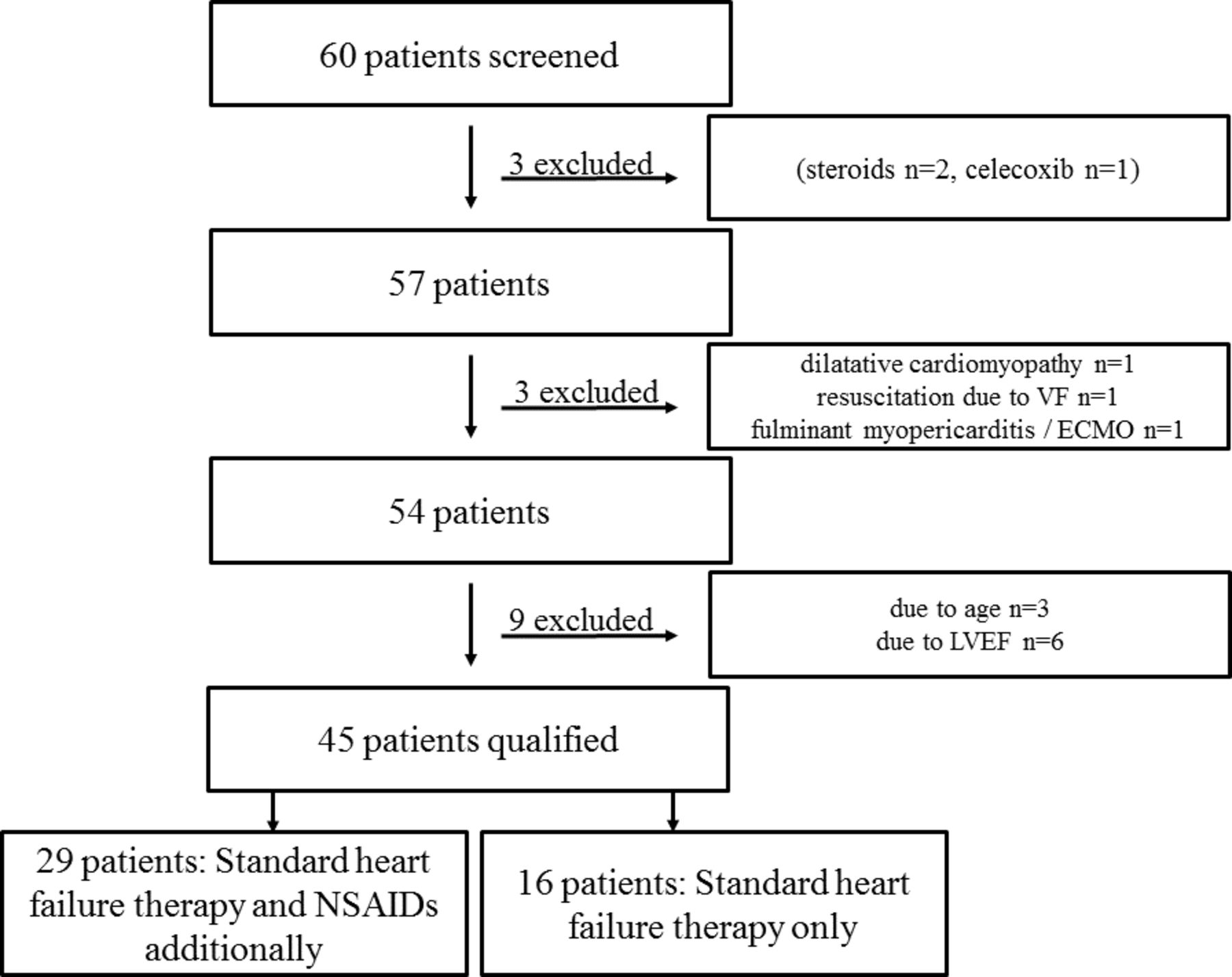
Patient enrolment. This flow chart shows the recruitment of patients and exclusion criteria. ECMO, extracorporeal membrane oxygenation; LVEF, left ventricular ejection fraction; NSAID, non-steroidal anti-inflammatory drug; VF, ventricular fibrillation.
Forty-five patients with myopericarditis qualified for our retrospective case-control study. Patients treated with (n=29) and without NSAIDs (n=16) were by design similar at baseline (table 1). Importantly, there was no significant difference in age, gender, body mass index (BMI), tobacco use, cardiac enzymes and inflammatory parameters. Thirty-nine patients (87%) were men and mean age was 34±13 years. LVEF (calculated by MRI) was normal or mildly decreased (>50%) in all patients treated with NSAIDs while it was normal in 13/16 patients (81%) treated without NSAIDs. Three out of 16 patients treated without NSAIDs presented with mildly impaired LVEF. Mean LVEF in the overall patient population (n=45) was 56%±5% (57±4 in the group treated with NSAIDs vs 55±6 in the group without NSAIDs, p=0.09). Eighteen patients were smokers (40%) and mean BMI was 26±4 kg/m2. Mean high sensitivity troponin T was 757±1453 ng/L, mean NT-pro-brain natriuretic peptide 635±1051 ng/L and mean myoglobin 82±85 µg/L. Mean C reactive protein was 45±45 mg/L and mean leucocyte count 8.8±2.9 G/L. Presenting symptoms at the time of diagnosis included chest pain in 42, dyspnea in 10 and syncope in 2 cases.
Baseline conditions of patients with and without non-steroidal anti-inflammatory drug (NSAID) therapy
Medication
A total of 29 patients received ASA (n=7, mean daily dose=1300 mg) or ibuprofen (n=22, mean daily dose=1500 mg) for an average duration of 4 weeks in addition to standard heart failure therapy. Five patients treated with NSAIDs received additional therapy with colchicine. The remaining 16 patients received standard heart failure therapy as indicated. Heart failure therapy included beta blockers (n=9), ACE inhibitors (n=18), angiotensin receptor blockers (n=2) and diuretics (n=1). None of the patients received aldosterone antagonists.
Clinical follow-up at 3 months
All patients were scheduled for clinical follow-up at 3 months. Follow-up data were obtained from 40 patients, while 5 were lost to follow-up (4 in the NSAID group and 1 in the standard heart failure group). Mean follow-up time was 12.1±9.6 months (median 11 months, range 1–47 months). Eight patients (18%) continued to report occasional brief episodes of chest pain at 3-month follow-up; six of them were in the NSAIDs group (6/29 patients=21%, ASA: n=2, ibuprofen: n=4), two of them in the standard heart failure therapy group (2/16 patients=13%). One patient (6%) in the standard heart failure therapy group reported episodes of dyspnea on exertion (New York Heart Association II), whereas none of the patients treated with NSAIDs reported dyspnea.
Blood pressure
Blood pressure values at the time of the initial hospital admission were similar for both groups with a mean of 123/75±15/10 mm Hg for patients who were later treated with NSAIDs additionally and a mean of 127/79±16/13 mm Hg for patients later receiving standard heart failure therapy only (p=0.5 for systolic values and p=0.18 for diastolic values). NSAID use did not significantly change blood pressure values during follow-up with a mean blood pressure of 124/75±14/9 mm Hg for patients having received NSAIDs and 123/75±13/9 mm Hg for patients receiving standard heart failure therapy only at 3 months (p=0.81 and 0.83) and a mean of 124/75±11/8 mm Hg and 124/76±9/5 mm Hg at 6 months (p=0.73 and 0.4), respectively.
However, there was a significant decrease in overall blood pressure values from initial hospital admission to hospital discharge in the general patient cohort (mean 124/76±15/11 mm Hg on admission and mean 116/69±12/10 mm Hg at discharge, p=0.006 and p=0.001) with blood pressure values returning to baseline values during follow-up.
Exercise capacity
A total of 28 patients (62%) underwent bicycle stress testing (standard heart failure therapy, n=12; NSAIDs n=16). There was no difference in exercise capacity between the two groups: the group receiving NSAIDs performed with 202±50W/9.7±2.7 metabolic equivalents, while the group with standard heart failure therapy performed with 200±67 W/ 9.6±2.8 metabolic equivalents, p=0.87). One patient (1/12=8%) receiving standard heart failure therapy developed increasing ventricular ectopy, syncope and convulsions during exercise stress testing. Monitoring revealed sinus tachycardia. The episode was interpreted as a seizure and was treated successfully with intravenous midazolam.
48-hour Holter monitoring
The rate of premature ventricular contractions (PVC) on 48-hour Holter monitoring was overall low among both patient populations. In patients treated with NSAIDs, mean PVC rate was 0.007%±0.02%, while it was 0.25%±0.48% (p=0.44) in the group on standard heart failure therapy.
Renal function
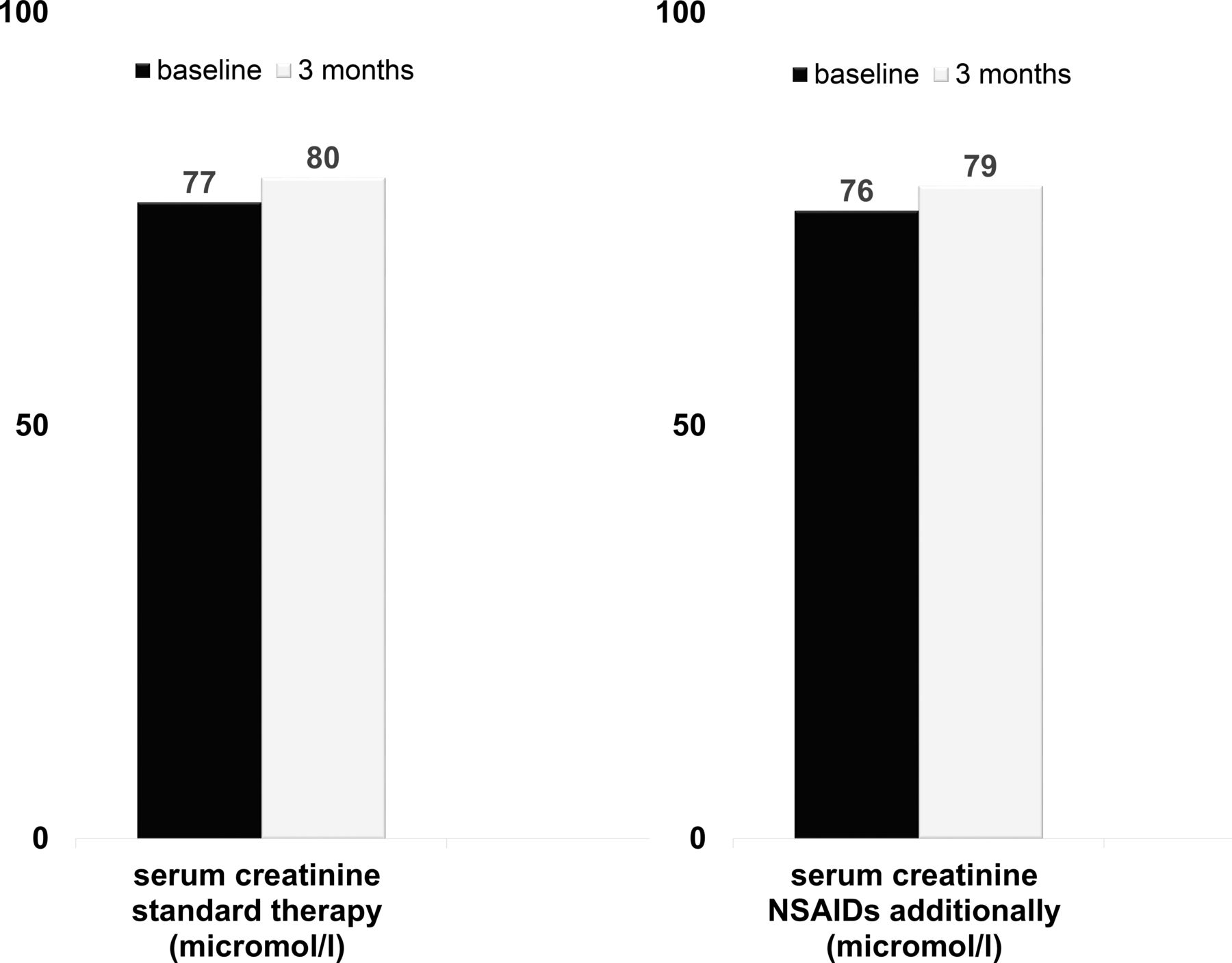
Based on serum levels of creatinine obtained at 3 months, there was no significant difference in kidney function between the two groups: average creatinine level in patients with NSAIDs was 76±11 µmol/L at baseline and 79±12µmol/L at 3-month follow-up while it was 77±15 µmol/L at baseline and 80±15 µmol/L at 3-month follow-up in patients with standard heart failure therapy (p=0.97, figure 2).
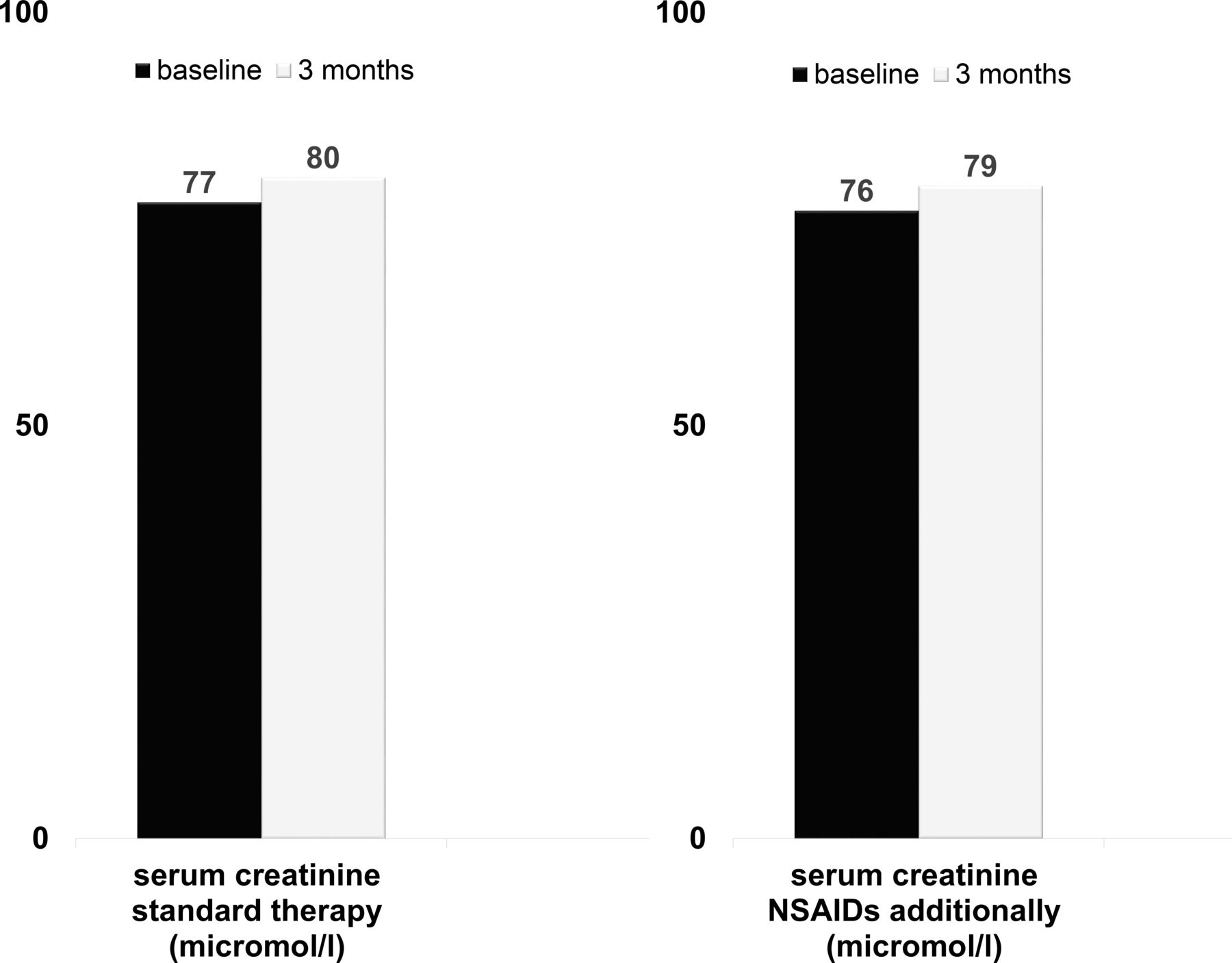
No significant change in serum creatinine. The left diagram indicates mean creatinine levels of patients with additional non-steroidal anti-inflammatory drugs (NSAIDs); the right diagram shows mean creatinine levels of patients with standard therapy only.
CMR examination at baseline and 3-month follow-up
All patients (n=45) presented with LGE in the pericardium and myocardium at baseline. Twenty-four of those (53%) also presented with myocardial oedema according to T2 imaging. Twelve patients (27%) had pericardial effusion without impact on haemodynamics and three (7%) showed pericardial thickening according to MRI imaging.
Twenty-nine patients (64%) underwent follow-up CMR at 3 months. Among the 29 patients with CMR both at baseline and at 3-month follow-up, 17 received NSAIDs (ASA: n=6, ibuprofen: n=11). Eighty-two per cent of the patients (14 of 17) treated with NSAIDs experienced a decrease in LGE at 3 months as compared with 58% (7 of 12) in those not receiving NSAIDs (figure 3). However, the level of significance was not reached (p=0.15). In one of the patients treated with NSAIDs, there was an increase in LGE at 3 months—no increase in LGE was observed in the group without NSAIDs. LGE resolved entirely in three patients (NSAID group: n=2, standard therapy group: n=1, p=0.77). At 3-month follow-up, oedema was still present in one patient (1/29; 3%), five patients (17%) continued to have signs of pericardial effusion, while one patient with pericardial effusion continued to have pericardial thickening.

{kind=link}
{kind=link}
{kind=link}
Trend towards improved late gadolinium enhancement (LGE) under non-steroidal anti-inflammatory drug (NSAID) therapy. In 14 of 17 patients treated with NSAIDs, there was a decreased LGE extent at 3 months compared with 7 of 12 in those with standard therapy only. LGE remained unchanged in 2 of 17 with NSAIDs and 5 of 12 without NSAIDs. One patient with NSAIDs experienced an increased LGE, while no increase of LGE was observed in those without NSAIDs.
Adverse events during follow-up
There was one adverse event (6%) in the group with standard heart failure therapy: One of the patients experienced polymorphic ventricular tachycardia with cardiac arrest at 6-month follow-up, requiring resuscitation and implantation of a cardioverter defibrillator. This patient initially presented with an almost normal LVEF of 50% but had previously been diagnosed with LGE persistence on CMR at 3-month follow-up. One adverse event (3%) occurred in the group with NSAIDs. The patient experienced an asymptomatic episode of non-sustained ventricular tachycardia on 48-hour Holter at 3-month follow-up, which lasted for 9 beats. In this case, the initial LVEF was 56% and follow-up MRI showed a decrease in LGE.
Discussion
This is the first case-control study to evaluate the effect of NSAIDs on the clinical course of myopericarditis on top of standard heart failure therapy. The results demonstrate that NSAIDs are safe over an observation period of 12 months both clinically as well as regarding blood pressure, renal function, arrhythmias and exercise tolerance in such patients. Furthermore, CMR suggests that NSAIDs may even be protective and reduce LGE, an index of myocardial damage, although significance was not reached due to low numbers.
In a previous study by Buiatti and colleagues,22 62 patients were diagnosed with myopericarditis based on clinical presentation, laboratory parameters, ECG and echocardiography. Similar to our case-control study, among 61 patients treated with NSAIDs, no cardiovascular adverse events were reported after 1 year of therapy. However, no control group was provided in this study. In a multicentre study by Imazio and colleagues,23 myocardial involvement was determined by CMR at baseline. In an overall patient population of 486 cases with pericarditis, there were 140 patients with myocardial involvement. Out of these, 76% or 106 patients were treated with NSAIDs with ASA being the predominant drug. For treatment of pericarditis, a dose of 750–1000 mg orally every 6 or 8 hours for 7–10 days was chosen with gradual decrease of the dose over 2–3 weeks until treatment was stopped. However, patients with myocardial involvement were given a lower dosage of 500 mg every 8–12 hours, which is somewhat less than the dosage generally used for anti-inflammatory effects in pericardial disease.10 After a median of 36 months, no deaths or heart failure were recorded.
Very recently, Ammirati and colleagues published data from a retrospective multicentre registry examining characteristics, in-hospital treatment and long-term outcome of patients with acute myocarditis.30 The final study population included 443 patients. NSAIDs were used in 267 out of 433 patients (44% NSAIDs in cases with complicated myocarditis and 67.6% NSAIDs in uncomplicated myocarditis) suggesting safety for this drug class. CMR at baseline and at follow-up was obtained; however, time course of LGE was not examined. Main finding of this study was that adverse events after acute myocarditis were lower than previously reported and mainly driven by reduced LVEF, ventricular arrhythmias or low cardiac output at presentation. However, Ammirati and colleagues suggested safety of NSAIDs and findings of this registry did not support the findings of NSAIDs leading to worse prognosis in viral myocarditis as observed in murine models.
Thus, although adverse effects of NSAIDs have been observed in animal studies in the setting of experimental myocarditis, our findings support prior, but less well-controlled studies in humans, which found no major adverse cardiovascular events under NSAID therapy during long-term follow-up in myopericarditis. Follow-up in these prior studies included a clinical examination, blood examinations, echocardiography22 and exercise treadmill testing.23 In one recent study in patients with acute myocarditis receiving NSAID therapy, CMR follow-up was included but time course of LGE was not examined. Our case-control study substantiates these preliminary findings by others and provides additional information with CMR demonstrating a trend for a reduction in LGE at 3 months in those receiving NSAIDs.
Conclusion
Our data suggest a notion of safety for NSAIDs in myopericarditis and preserved LVEF. We conclude that further evaluation of NSAIDs in patients with myopericarditis in a prospective double-blinded randomised trial should be considered.
Limitations
Given the small sample size, significance levels of LGE dynamic may vary in a larger patient cohort. Nine patients among the standard therapy group had to be excluded from analysis to create two groups with homogenous baseline conditions in this matched case-control study. Excluded patients were older and had worse LVEF. Five patients were lost to follow-up.
Acknowledgments
The authors would like to thank the clinical staff and nurses of the Division of Cardiology at the University Hospital Zurich for their help with patient enrolment. Also, they would like to thank the Swiss National Science Foundation, the University of Zurich, the Holcim Foundation and the Walter and Gertrud Siegenthaler Stiftung for financial support of this project.
References
Footnotes
JB and ML contributed equally.
Contributors All authors contributed in either clinical follow-up on patients or giving valuable input in order to improve the manuscript.
Funding Project Grant of the Swiss National Science Foundation, Forschungskredit of the University of Zurich FK-17-047; the Holcim Foundation, Walter and Gertrud Siegenthaler Stiftung at the University of Zurich.
Competing interests None declared.
Patient consent for publication Obtained.
Ethics approval Ethics committee of the Kanton of Zurich.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request.