Article Text

Abstract
Objective In order to avoid effects of referral bias, we assessed risk factors for disease-related mortality in a geographical cohort of patients with hypertrophic obstructive cardiomyopathy (HOCM), and any therapy effect on survival.
Methods Diagnostic databases in 10 hospitals in the West Götaland Region yielded 251 adult patients with HOCM (128 male, 123 female). Case notes were reviewed for clinical data and ECG and ultrasound findings. Beta-blockers were used in 71.3% of patients from diagnosis (median metoprolol-equivalent dose of 125 mg/day), and at latest follow-up in 86.1%; 121 patients had medical therapy alone, 88 short atrioventricular delay pacing and 42 surgical myectomy. Mean follow-up was 14.4±8.9 (mean±SD) years. Primary endpoint was disease-related death, and secondary endpoint heart failure deaths.
Results There were 65 primary endpoint events. Independent risk factors for disease-related death on multivariate Cox hazard regression were: female sex (p=0.005), age at diagnosis (p<0.001), outflow gradient ≥50 mm Hg at diagnosis (p=0.036) and at follow-up (p=0.001). Heart failure caused 62% of deaths, and sudden cardiac death 17%. Late independent predictors of heart failure death were: female sex (p=0.003), outflow gradient ≥50 mm Hg at latest follow-up (p=0.032), verapamil/diltiazem therapy (p=0.012) and coexisting hypertension (p=0.031), but not other comorbidities. Neither myectomy nor pacing modified survival, but early and maintained beta-blocker therapy was associated with dose-dependent reduction in disease-related mortality in the multivariate model (p=0.028), and final dose was also associated with reduced heart failure mortality (p=0.008). Kaplan-Meier survival curves analysed in initial dose bands of 0–74, 75–149 and ≥150 mg metoprolol/day showed 10-year freedom from disease-related deaths of 83.1%, 90.7% and 97.0%, respectively (ptrend=0.00008). Even after successful relief of outflow obstruction by intervention, there was survival benefit of metoprolol doses ≥100 mg/day (p=0.01).
Conclusions In population-based HOCM cohorts heart failure is a dominant cause of death and on multivariate analysis beta-blocker therapy was associated with a dose-dependent cardioprotective effect on total, disease-related as well as heart failure-related mortality.
- hypertrophic obstructive cardiomyopathy
- risk factors
- mortality
- heart failure
- beta-blockers
- metoprolol
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known about this subject?
Much research on patients with hypertrophic cardiomyopathy (HCM) has come from tertiary centre populations with possible referral bias for patients with a malignant family history. In those populations sudden cardiac death (SCD) has been an important proportion of disease-related mortality. Major risk factors for SCD include extreme cardiac hypertrophy, cardiac syncope and a malignant family history. Left ventricular outflow tract obstruction is considered a minor risk factor.
What does this study add?
This study on a complete geographical cohort of patients with obstructive HCM, and long and 100% complete follow-up, shows that heart failure caused a majority (62%) of disease-related deaths, and that SCD only constituted 17% of deaths. Furthermore, this study is the first to demonstrate on multivariate analysis the independent risk factors specifically for heart failure death: female sex, verapamil/diltiazem therapy, coexisting systemic hypertension and outflow gradient ≥50 mm Hg. Thus, risk factors for heart failure death are different from those for SCD. This study also suggests that pharmacotherapy with beta-blockers in doses similar to target doses for dilated cardiomyopathy is associated with reduced risk of heart failure death in a dose-dependent fashion.
Key questions
How might this impact on clinical practice?
American Heart Association guidelines suggest that symptom-free left ventricular outflow tract obstruction need not be treated, but our results indicate that in obstructive HCM there is survival benefit from pharmacotherapy with beta-blockers, even in those patients where interventional treatment has reduced gradient to <30 mm Hg. Furthermore, our results suggest that other risk factors like systemic hypertension need optimal control, and that perhaps calcium channel blockers should be avoided in this patient group.
Introduction
Hypertrophic cardiomyopathy (HCM) is often associated with a dynamic muscular outflow tract obstruction, and tertiary centres report that outflow tract obstruction is a risk factor for both more rapid symptomatic deterioration and death.1 Nevertheless, the American Heart Association (AHA) guidelines for treatment of HCM suggest that left ventricular outflow tract obstruction (LVOTO) without symptoms does not necessarily need treatment.2 Whereas LVOTO is not considered a major risk factor in the AHA 2011 guidelines,2 it is included in the latest European Society of Cardiology algorithm for assessing risk of sudden cardiac death (SCD).3 Most studies on risk factors have emanated from specialised tertiary centres subject to possible referral bias. Therefore, we studied the long-term outcome of patients with hypertrophic obstructive cardiomyopathy (HOCM) in an unselected complete geographical cohort in order to assess risk factors for adverse outcome. No long-term prospective randomised trials of the effect of currently used therapy on survival have been performed so far, thus we included possible effect on survival of drug therapy, myectomy and pacing in the analysis.
Materials and methods
Patient population
Adult cardiac care for the 1.6 million inhabitants of West Götaland Region is provided by 10 hospitals (listed in the Acknowledgements section). We searched all hospital diagnostic databases for adult inpatients and outpatients attending hospital from January 2002 to December 2013 with diagnostic codes relating to a diagnosis of HCM, and reviewed the case notes on site to identify those with HCM and outflow tract obstruction (HOCM). Diagnosis of HCM was based on standard clinical criteria as defined previously.4 Patients were categorised as HOCM if they had a verified LVOT pressure gradient of ≥30 mm Hg at rest.3 During the study period, 1142 patients had a verified diagnosis of primary HCM, and from that group 251 patients (128 male, 123 female) fulfilled the HOCM criteria.
Therapy modalities employed
Patients were initially treated medically, and 121 patients remained on medical therapy only, but 130 required interventions, 88 with short atrioventricular delay pacing and 42 with myectomy (flow chart in online supplementary figure S1). Detailed comparisons of haemodynamic and symptomatic outcomes, and of survival, between myectomy and pacing in this cohort have been published and showed equivalent efficacy.5 Consequently, in this study we examined the risk factors for disease-related death in the total HOCM group. Type and dose of beta-blocker and calcium-blocker therapy were recorded. For statistical comparison, all beta-blocker doses were converted to equivalent doses of metoprolol (the beta-blocker most commonly employed: 48.6% metoprolol, 22.7% bisoprolol, 7.5% propranolol and 6.7% atenolol). The conversion used was metoprolol 100 mg=propranolol 80 mg6=bisoprolol 5 mg=atenolol 50 mg.
Supplemental material
Clinical measures collected
Clinical features (including proposed risk factors and comorbidities), ECG and echocardiographic measurements, implantable cardioverter-defibrillator (ICD) therapies and type of medical therapy and dose used were documented at diagnosis, and at latest follow-up visit.
Cause of death
Vital status was censored on 28 February 2015. The Swedish unique personal identification number allowed us to establish causes of death by death certificates from the National Board of Health and Welfare, in addition to case note review. No patient was lost to follow-up. The primary endpoint was a composite of total cardiac mortality, heart transplantation and fatal embolic stroke of presumed cardiac origin together referred to as ‘disease-related death’.
Statistics
Analysis was carried out by SPSS statistical software, V.22.0 (IBM). The majority of the variables studied did not show a normal distribution, and accordingly those data are presented by median (IQR). Statistical comparisons of paired continuous variables were made by Wilcoxon signed-rank test, and for paired binary data with McNemar test. Survival was analysed by Kaplan-Meier curves and the log-rank test, and comparative analysis of risk factors for the endpoint was carried out by univariate and multivariate Cox proportional hazards method. Variables were selected for multivariate analysis if univariate p values were ≤0.20. The number of variables was restricted to six at a time in our multivariate models in order to have adequate statistical power, and were analysed with backward selection. All tests were two sided, and p values <0.05 were considered statistically significant; variables with p<0.10 on multivariate analysis were kept in multivariate models. Correlations were analysed with Pearson’s correlation coefficient for continuous variables and Spearman’s rho for categorical data. For intergroup comparisons in online supplementary tables, Mann-Whitney U test was used for continuous variables, and two-tailed Fisher’s exact test and χ2 test for categorical variables as appropriate.
Results
Characterisation of the cohort
Mean follow-up was 14.4±8.8 years (mean±SD) and median follow-up 13.2 (IQR=12.4) years. Findings at the time of diagnosis and at latest follow-up are shown in table 1. The sex distribution was even, but females were generally older. Initial medical therapy consisted of beta-blocker in 69.7%, verapamil/diltiazem in 10.8% and in 1.6% beta-blocker and calcium-blocker were combined; 17.9% of patients did not receive any initial pharmacotherapy. During follow-up there was improvement in New York Heart Association (NYHA) class with therapy, and reduction in resting LVOT gradient at rest to a median of 16 mm Hg. However, 21% had resting gradients remaining ≥50 mm Hg, and 33% ≥30 mm Hg at latest assessment. Atrial size and incidence of atrial fibrillation had increased at latest follow-up.
Characterisation of total cohort at diagnosis and at latest follow-up (n=251), shown as median (IQR) when not otherwise specified
Primary endpoint
There were 65 primary endpoint events (53 cardiac deaths, 4 heart transplants, 8 embolic deaths) during follow-up consisting of a total of 3614 patient-years. Only 11 deaths (17%) were attributed to SCD, with an annual rate of 0.37% during the first 10 years of follow-up. The majority of deaths were due to heart failure (62%), with myocardial infarct (8%) and embolic strokes (12%) being less common. There were 25 non-cardiac deaths in the cohort.
ICD implantations
Sixteen patients (6.4%) had received ICD implantation (4 secondary, 12 primary prevention). There was one appropriate discharge in 149 patient-years, that is an appropriate annual discharge rate of 0.67%.
Medical therapy employed
Beta-blocker use increased from 71.3% at diagnosis to 86.1% at latest follow-up, with no significant differences between intervention and non-intervention groups (online supplementary table S1). The beta-blocker dose prescribed initially had no significant correlations to NYHA class, chest pain, syncope, outflow gradient or severity of cardiac hypertrophy (correlation coefficients between −0.053 and 0.144 for all). Hence, patients with the most advanced disease did not receive lower doses. The median initial dose prescribed was 125 mg metoprolol/day, and at latest follow-up was 150 mg/day for patients given beta-blockers. Verapamil/diltiazem therapy was given in median doses of 240 (IQR=80) mg/day, and altered only from 12.4% of patients to 12.7% at latest follow-up. For other medication, see online supplementary table S1.
Cox hazard analysis of risk factors
Risk factors at presentation for subsequent disease-related death
Among risk factors significantly associated with outcomes on univariate analysis were age at diagnosis, female sex, coronary artery disease and a resting LVOT gradient ≥50 mm Hg. In the multivariate analysis of the whole group, those risk factors except coronary artery disease remained as significant independent risk factors. Comorbidities and accepted risk factors for SCD were not significant risk factors for total disease-related deaths (table 2).
Risk factors/protective factors at diagnosis for disease-related and heart failure death on Cox hazard regression
Risk factors that were significantly associated with disease-related mortality were also significantly associated with all-cause mortality (online supplementary table S2).
For heartfailure deaths female sex and age were independent risk factors on multivariate analysis (table 2; univariate risk factors, see online supplementary table S3).
Influence of therapy choice on survival
Neither pacing nor myectomy reduced disease-related deaths significantly, whereas use of beta-blocker therapy started at diagnosis was associated with reduced risk on univariate Cox hazard analysis (p=0.004). The association with outcome appeared to be dose dependent with reduced risk with increased daily dose (p=0.001) and dose dependency remained significant in the multivariate analysis (p=0.028; table 2), also for heart failure deaths specifically (table 2; online supplementary table S3). The HR between early beta-blocker use and non-use was 0.49 (95% CI 0.30 to 0.81), p=0.006. Freedom from disease-related deaths for patients given ≥100 mg/day was significantly better than for those given 0–99 mg/day (log-rank: p=0.00004; figure 1A), as was all-cause survival, p=0.00005 (online supplementary figure S2). There were no significant differences in comorbidities between patients in 0–99 mg/day and ≥100 mg/day groups (online supplementary table S4). The survival curves of patients given no beta-blocker (n=74) were overlapping the curves of patients given 25–74 mg/day (n=36; p=0.67; online supplementary figure S3) and these patients were combined in a 0–74 mg/day group. Survival curves depicting three dose ranges: 0–74 mg/day, 75–149 mg/day and ≥150 mg/day of metoprolol equivalents, the middle band encompassing the median dose, show the benefit of larger doses of beta-blocker most clearly. There was a significant log-rank for trend in reduced risk of disease-related deaths with increased dose (p=0.00008; figure 1B). The 10-year freedom from disease-related deaths for the three dose bands, 0–74, 75–149, ≥150 mg/day, was 83.1%, 90.7% and 97.0%, respectively. The 20-year proportions were 65%, 74% and 86%, respectively. The 10-year freedom from disease-related deaths of patients without beta-blocker therapy was 81.7%. Analysis of total mortality confirmed a similar pattern (log-rank ptrend=0.00009), with 10-year all-cause survival of 78.7%, 88.8% and 91.1% in respective dose bands.

(A) Kaplan-Meier survival curve illustrating freedom from disease-related death in patients with initial beta-blocker dose 0–99 mg/kg, that is, less than the total cohort median dose of 100 mg metoprolol equivalents/day (blue curve), or equal to or greater than 100 mg/day (black curve), who on log-rank testing have significantly superior survival (p=0.00004). (B) Kaplan-Meier survival curves showing freedom from disease-related death in patients receiving 0–74 mg/day (blue curve), 75–149 mg/day (black curve) or ≥150 mg/day (red curve) in metoprolol equivalents, with increasing daily dose showing significant trend of improvement (p=0.00008). The numbers below the curves indicate the number of patients remaining in the survival curves.
Verapamil therapy, on the other hand, was associated with increased risk on univariate analysis (p=0.014; table 2).
Predictors of disease-related death at latest follow-up
On univariate Cox hazard analysis, female sex, age, NYHA class ≥III, a gradient remaining ≥50 mm Hg and a smaller left ventricle end-diastolic diameter were associated with a significantly increased risk. Progression to dilated end stage was observed in only 4%. Larger beta-blocker dose was associated with lower risk of disease-related death also at latest follow-up (p=0.018). Verapamil/diltiazem was a risk factor on univariate, but not multivariate analysis. Neither use of amiodarone, disopyramide, ACE inhibitor nor spironolactone showed any significant influence on survival. Also at latest follow-up a higher beta-blocker dose remained an independent predictor associated with reduced risk of disease-related death in multivariate analysis (p=0.021). Comorbidities were not independent predictors in the multivariate model (table 3).
Predictor factors/protective factors for disease-related and heart failure death on Cox hazard regression as recorded at latest follow-up
For heartfailure deaths specifically, female sex, verapamil/diltiazem therapy, coexisting systemic hypertension and outflow gradient ≥50 mm Hg remained independent risk predictors, whereas beta-blocker dose reduced risk (p=0.008) in the multivariate model (table 3; for univariate results see online supplementary table S5).
Multivariate analysis of risk factors, therapies and comorbidities in relation to total all-cause mortality is shown in online supplementary table S6. The risk predictors for total all-cause mortality were similar as for disease-related deaths: female sex, age, LVOT gradient ≥50 mm Hg and maximal wall thickness. Higher daily dosage of beta-blockers was associated with better survival also on multivariate analysis for total mortality (p=0.008).
Beta-blocker and postintervention gradient
Patients not receiving early beta-blockers had significantly higher proportion of disease-related deaths, if post-treatment gradient was ≥30 mm Hg (10-year proportion 39.1%) than with gradients <30 mm Hg (10-year proportion 7.4%; p=0.002). Accordingly, we analysed whether the apparent protective effect of beta-blockers was present only in patients with a residual gradient of ≥30 mm Hg after initial therapy. This appeared not to be the case as shown in figure 2A,B.
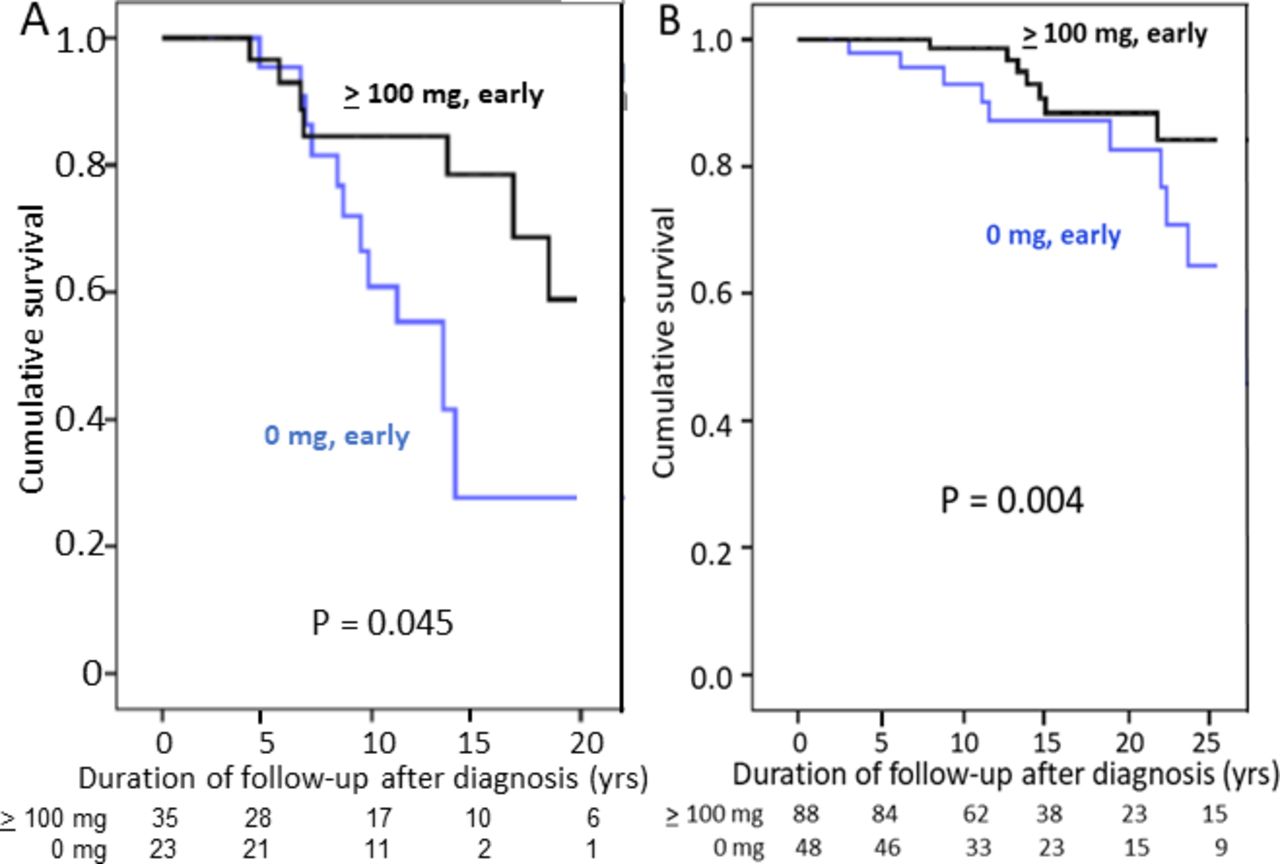
(A) Kaplan-Meier survival curve comparing freedom from disease-related death in patients with residual gradient on treatment ≥30 mm Hg in patients with a median initial dose of ≥100 mg/day of metoprolol equivalents (black curve) to patients not receiving any beta-blocker (blue curve). There are few patients with gradients ≥30 mm Hg, but the difference is nevertheless significant (p=0.045). (B) Kaplan-Meier survival curve comparing freedom from disease-related death in patients with residual gradient on treatment <30 mm Hg in patients with a median initial dose of ≥100 mg/day of metoprolol equivalents (black curve) which also have significantly better survival (p=0.004) to patients not receiving any beta-blocker (blue curve). The numbers below the curves indicate the number of patients remaining in the survival curves.
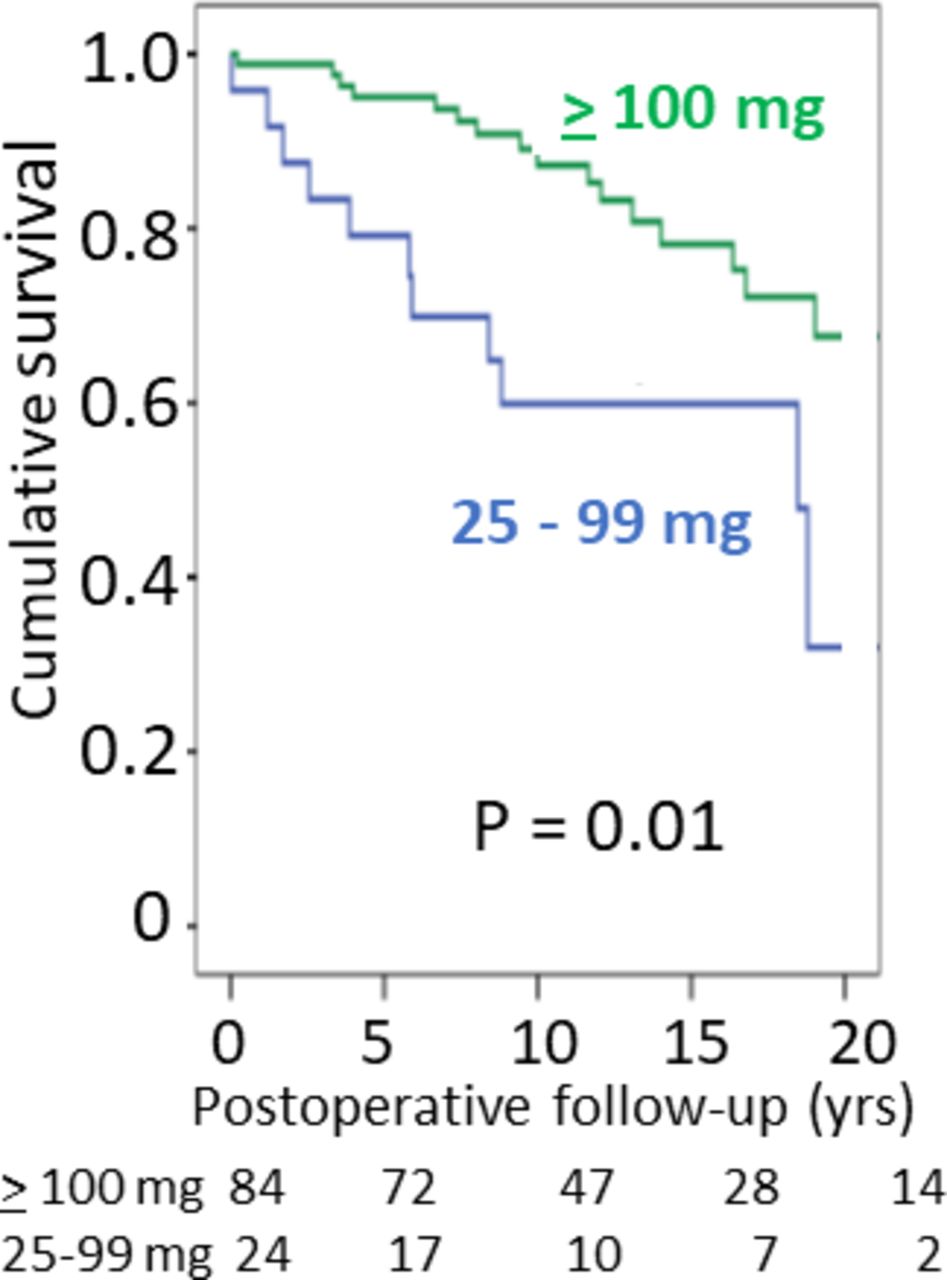
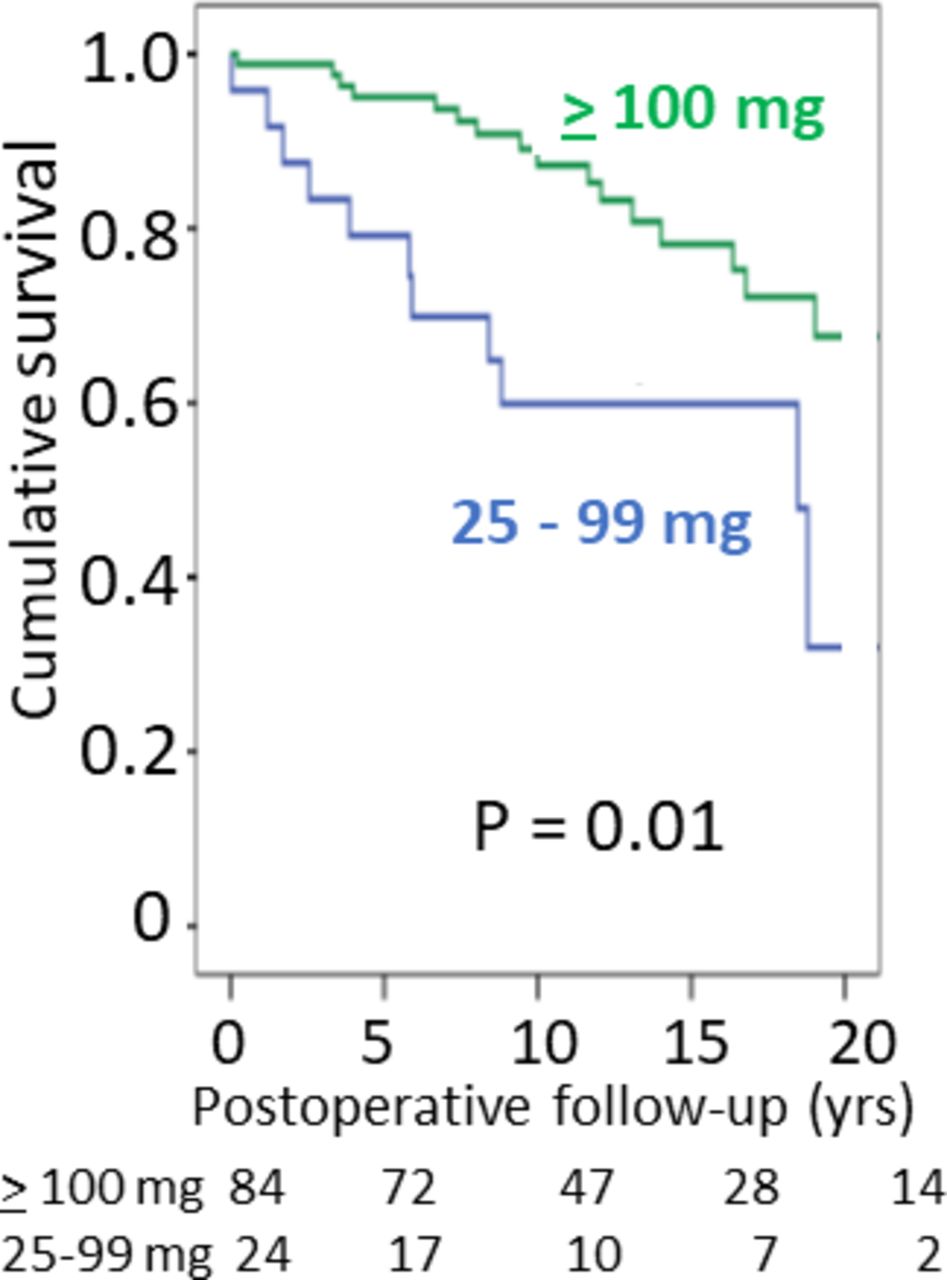
Some patients with good relief of outflow tract obstruction after interventional procedures had beta-blocker therapy reduced after intervention. We therefore explored whether postintervention beta-blocker dose influenced survival, and found that a beta-blocker dose ≥100 mg metoprolol equivalent/day was associated with significantly better outcome than low dose (25–99 mg) (figure 3).
{kind=link}
{kind=link}
{kind=link}
Kaplan-Meier survival curves illustrating postintervention freedom from disease-related death in patients who have received interventional treatment with either short atrioventricular (AV) delay pacing or myectomy related to postintervention dose of beta-blocker therapy. The green curve illustrates survival with postintervention dose of ≥100 mg/day of metoprolol equivalents, and the blue curve the inferior survival with metoprolol-equivalent doses of 25–99 mg/day (p=0.010).
Effect of comorbidities
There was no significant skewing of proportion of patients with comorbidity between patient groups in figure 3 (online supplementary table S7). Furthermore, there was no excess comorbidity in patients who had died a disease-related death (online supplementary table S8).
Discussion
Risk factors for long-term mortality
Age, female sex and an unrelieved LVOT gradient were significant risk factors for disease-related mortality in this study of a geographical cohort of patients with HOCM. These have previously been reported by others.1 7–10 It is noteworthy that in our geographical cohort of patients with HOCM, SCD caused a small proportion of disease-related deaths, in spite of a low rate of ICD implantations (6.4%), in contrast to reports from tertiary centres. For example, in a multicentre study of patients with similar age profile as ours, SCD comprised 39% of deaths in the HOCM group, with annual SCD mortality of 0.75%–1.26% in various groups,11 compared with an annual SCD mortality of 0.37% in our study. This may explain why risk factors thought to be important for SCD, such as family history of SCD and maximal wall thickness ≥3 cm, failed to show significant impact on total disease-related mortality in our cohort, in contrast to an LVOT gradient ≥50 mm Hg. A recent study identified unmet clinical needs in population-based patients with HCM including a 4.3 times excess of heart failure, and that heart failure was more common than SCD and ventricular arrhythmias combined,12 as in our study. This underlines the importance of evaluating therapies that may reduce non-sudden and heart failure-related mortality in HOCM, like a good control of significant risk factors for heart failure death on multivariate analysis in this study such as systemic hypertension and LVOTO.
Effect of therapy on risk of death
Surgical septal myectomy has long been considered the gold standard treatment for therapy-resistant patients with HOCM,2 13 14 and suggested to give superior survival compared with conservative treatment.15 However, the conservatively treated group was on average 10 years older, and a reduction in cardiovascular mortality in the intervention group could not be substantiated.15 We have earlier reported that in a geographical cohort of patients with HOCM, neither myectomy nor pacing was significantly associated with improved survival compared with conservative medical therapy, although both treatments improved NYHA class.5 In the present study, neither univariate nor multivariate Cox hazard analysis could detect that myectomy or pacing was associated with a survival benefit that was independent of other risk factors such as age (tables 2 and 3). Thus, the only therapy associated with significant improvement of survival on multivariate analysis in our cohort was beta-blocker therapy. The observed excess mortality in heart failure in patients with HOCM receiving verapamil/diltiazem is concerning but should be interpreted with caution due to the small numbers receiving calcium-blockers. This merits further study in HCM populations with higher use of calcium channel blockers than ours.
Benefit of beta-blocker therapy
Beta-blocker therapy reduces LVOT gradient in HOCM, both at rest and during exercise, and improves symptoms, diastolic function and exercise capacity.16–21 In childhood HCM, it is also associated with improved survival22 in a dose-related manner,23 24 and reduces risk of SCD.25 It has been claimed that beta-blocker therapy does not affect survival in adult HCM,26 although Frank et al27 reported particularly low SCD mortality (0.3%) in patients treated with relatively high doses of propranolol, aiming for ≥320 mg/day. In another study on 163 consecutive patients, average follow-up of 5.3 years, of whom 40% received beta-blockers, beta-blocker was significantly associated with improved outcome, HR 0.25 (95% CI 0.08 to 0.77), p=0.0120.9 In a larger recent study that focused on sex differences in survival (3673 patients), beta-blocker therapy (dose unspecified) was associated with a lower all-cause mortality (they were unable to separate cardiac mortality).28 These observations support our finding that beta-blocker therapy emerges as a significantly protective factor for disease-related deaths even on multivariate analysis (tables 2 and 3, and figure 1A,B), confirmed in an all-cause mortality analysis. Previous studies have included both non-obstructive and obstructive HCM, and the effect we observed might be due to gradient reduction or to the doses employed. Findings illustrated in figure 2B make the former mechanism unlikely. Among patients receiving beta-blockers the early median metoprolol dose for survivors was 162.5 mg metoprolol/day, and median latest follow-up dose was 175 mg/day. Thus, the survivor doses are within the range of doses used in the prospective randomised trials on heart failure that have demonstrated metoprolol significantly reduces cardiac mortality.29 A dose effect would tally with studies that show heart rate lowering efficacy of beta-blocker dose correlates to reduction in mortality in patients with heart failure.30
However, our significant results are quite likely also a question of statistical power. Melacini et al’s negative study from 200726 lacked statistical power to detect a protective effect of beta-blockers: out of 293 patients only 26% were treated with beta-blockers, giving at most 456 patient-years, whereas our study has 2613 patient-years on beta-blocker therapy. With our study there are now three studies from patient cohorts of very different ethnic origin that report statistically significant protection from beta-blocker use. The HR for patients with beta-blocker use from diagnosis was 0.49 (95% CI 0.30 to 0.81) in our cohort. Furthermore, the association was dose dependent (figure 1A,B), suggesting a pharmacological effect and not a chance association.
Therapy with mild or latent obstruction
The finding of an apparent survival benefit of continued adequate beta-blocker therapy even in patients where interventions have reduced gradients to below 30 mm Hg might indicate that this therapy could be protective also in the absence of LVOT obstruction. A prospective randomised trial in non-obstructive HCM has not been performed. The observation that it takes around 5 years for survival curves to diverge significantly (figure 1A) indicates that the effect may be particularly on myocardial preservation perhaps affecting progress of fibrosis, rather than reducing SCD mortality as reported with higher paediatric dosages.25 Lacking controlled trials, it would be desirable that large international registries for HCM should collect and publish data on mortality related to pharmacotherapy, both type and dose.
Incomplete relief of LVOTO
Our results confirm earlier studies that patients in whom therapeutic interventions have failed to reduce the resting gradient below 30 mm Hg have a worse prognosis1 3; the risk is incremental and the prognosis is particularly poor with gradients ≥50 mm Hg. This underlines the importance of intensifying treatment even in asymptomatic patients if a sizeable resting gradient remains.
Strengths and limitations
The strengths of this study are the long follow-up and 100% complete cause of death information. Retrospective studies on complete unselected geographical cohorts are the method of choice in identifying risk factors for adverse outcomes, but it is not the method of choice for evaluating the effects of drug therapy, where prospective randomised trials would be preferable. The fact that there is no published prospective randomised drug trial using mortality as endpoint in patients with HCM, not even from supraspecialised centres, testifies to the difficulties in organising such studies. Particular handicap is studying drugs such as beta-blockers that are out of patent so that pharmaceutical companies have no incentive for financial support.
Conclusions
In this unselected geographical cohort we found that heart failure was a dominant cause of death in HOCM, and showed that female sex, age and persisting LVOT obstruction were important independent risk factors for disease-related, and specifically heart failure-related deaths. The data indicate that beta-blocker therapy would be beneficial even in asymptomatic LVOT obstruction, aiming for doses of at least 150 mg/day metoprolol equivalents. We hope these results will stimulate international collaborative prospective randomised studies of adequate duration of the effect of pharmacotherapy on survival in HCM.
Acknowledgments
We are most grateful for the helpful assistance of medical and clerical staff at the Sahlgrenska, Östra, Mölndal, Uddevalla, Trollhättan, Skövde, Lidköping, Alingsås, Borås and Kungälv Hospitals in the West Götaland Region, Sweden.
References
Footnotes
Contributors The design of the study was agreed between DJ, IÖ-S, BA and MS. DJ, N-JA and IÖ-S have collected the patient information. The statistical analyses have been carried out by DJ and IÖ-S. All authors have contributed to the writing and the revisions of the manuscript. The authors are not reusing any figures or tables previously published.
Funding The study was supported by grants from the Swedish Heart and Lung Foundation (Hjärt-Lungfonden; 20080510), and by a Swedish state ALF agreement (Gothenburg University) project grant (ALFgbg-544981).
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The study complies with the Helsinki convention and was approved by the University of Gothenburg Ethics Committee (approval number ÖS1012-12).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request. All data relevant to the study are included in the article or uploaded as supplementary information.