Article Text

Abstract
Introduction Myocardial injury markers such as high-sensitive cardiac troponin T (hs-cTnT) and creatine kinase MB (CK-MB) reflects the amount of myocardial injury with ablation. The aim of the study was to identify the value of myocardial injury markers to predict outcomes after pulmonary vein isolation (PVI) using three different ablation technologies.
Methods Consecutive patients undergoing PVI using a standard 3.5 mm irrigated-tip radiofrequency catheter (RF-group), an irrigated multielectrode radiofrequency catheter (IMEA-group) and a second-generation cryoballoon (CB-group) were analysed. Blood samples to measure injury markers were taken before and 18–24 hours after the ablation. Procedural complications were collected and standardised follow-up was performed. Logistic regression was used to identify predictors of recurrence and complications.
Results 96 patients (RF group: n=40, IMEA-group: n=17, CB-group: n=39) undergoing PVI only were analysed (82% male, age 59±10 years). After a follow-up of 12 months, atrial fibrillation (AF) recurred in 45% in the RF-group, 29% in the IMEA-group and 36% in the CB-group (p=0.492). Symptomatic pericarditis was observed in 20% of patients in the RF-group, 15% in the IMEA-group and 5% in the CB-group (p=0.131). None of the injury markers was predictive of AF recurrence or PV reconnection after a single procedure. However, hs-cTnT was identified as a predictor of symptomatic pericarditis (OR: 1.003 [1.001 to 1.005], p=0.015).
Conclusion Hs-cTnT and CK-MB were significantly elevated after PVI, irrespective of the ablation technology used. None of the myocardial injury markers were predictive for AF recurrence or PV reconnection, but hs-cTnT release predicts the occurrence of symptomatic pericarditis after PVI.
- radiofrequency
- cryoballoon
- nmarq
- ablation
- atrial fibrillation
- pulmonary vein isolation
- high-sensitive-troponin T
- creatine kinase-mb
- creatine kinase
- recurrence
- complications
- pericarditis
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- radiofrequency
- cryoballoon
- nmarq
- ablation
- atrial fibrillation
- pulmonary vein isolation
- high-sensitive-troponin T
- creatine kinase-mb
- creatine kinase
- recurrence
- complications
- pericarditis
Key questions
What is already known about this subject?
High-sensitive cardiac troponin T (hs-cTnT) release after ablation reflects the amount of myocardial injury.
What does this study add?
This is the first study to investigate the value of hs-cTnT measurements both to predict pulmonary vein isolation (PVI) efficacy and safety after an index PVI procedure using different technologies (focal and multielectrode radiofrequency [RF] ablation and second-generation cryoballoon).
A total of 96 patients undergoing PVI only using three different ablation technologies (focal RF, multielectrode RF and second-generation-cryoballoon) were analysed (82% male, 59±10 years, 58% paroxysmal atrial fibrillation [AF]).
High-sensitive-troponin-T was significantly elevated after PVI irrespective of the technology used.
How might this impact on clinical practice?
High-sensitive-troponin-T levels were not predictive for AF recurrence, but were predictive for symptomatic pericarditis.
Key message
This is the first study to investigate the value of myocardial injury markers (hs-cTn, CK, CK-MB) measurements both to predict pulmonary vein isolation (PVI) efficacy (freedom from AF recurrence and persistence of PVI) and safety after a first PVI procedure using RF catheters (focal and multielectrode) or the second-generation cryoballoon. The main findings of this study are:
High-sensitive cardiac troponin T (hs-cTnT) release after PVI was significant but was not different between the patient groups undergoing PVI with three different ablation technologies, but creatine kinase (CK) and CK-MB release was significantly different between the groups.
None of the myocardial injury markers was identified as a significant predictor of AF recurrence
nor as a predictor of PV reconnection in patients undergoing a redo procedure.
Hs-cTnT release was predictive of post-procedural symptomatic pericarditis.
Introduction
Pulmonary vein isolation (PVI) to disconnect the atrial fibrillation (AF) triggers within the pulmonary veins (PV) from the left atrium (LA) is a well-established therapeutic option for patients with AF.1 2 Various types of technologies for PVI are currently available with comparable success rates, and new ones, especially balloon-based multi-electrode catheters, are being used and developed.1–4 However, even in patients without symptomatic AF recurrence, PV reconnection is observed in roughly 60% of patients.5 6 Consequently, the goal of the current technological development is to increase the PVI success rate by improving the durability of the lesions. One option to quantify the acute effect of the ablation is to measure myocardial injury markers such as creatine kinase-MB (CK-MB) or high-sensitive cardiac troponin T (hs-cTnT) release as a marker of myocardial damage.7–9 The release of hs-cTnT with ablation has been studied with different ablation modalities.8 While controversial results exist on the efficacy of hs-cTnT release as a predictor of the long-term outcome after PVI, research focusing on the value of the hs-cTnT on procedural safety is lacking.8–10 Although currently performed on a routine basis, PVI is associated with a non-negligible complication rate of up to 16% with significant discrepancies in incidence and type depending on the technology used.1 11
The aim of the current study was to investigate the value of hs-cTnT release in prediction of the efficacy and safety of PVI in patients with AF using focal, multielectrode radiofrequency (RF) and cryoballoon (CB) technology.
Methods
We analysed consecutive patients with paroxysmal or persistent AF referred for ablation enrolled in our prospective BEAT-AF-PVI ablation registry. The hospital’s Ethics Committee approved the study and the study was conducted in accordance with the Declaration of Helsinki. Patients, in whom linear or other lesions for substrate modification in addition to PVI were performed, were excluded from the analysis. Transthoracic and transoesophageal echocardiogram to rule out left atrial thrombus and to assess left atrial (LA) diameter in the parasternal long axis and left ventricular ejection fraction (LVEF) were performed before the procedure.
Ablation procedure
Focal irrigated-tip RF catheter (RF-group) in combination with a 3D electroanatomical mapping system (Carto3, Biosense Webster, Diamond Bar, California, USA) was used to perform PVI as described in detail elsewhere.2 10 A 20-pole variable circular mapping catheter (Lasso 2515, Biosense Webster) and a 3.5 mm open irrigated-tip catheter (Thermocool, Biosense Webster, Diamond Bar, California, USA) were used. RF energy was delivered with 25W at the posterior wall and 30W at the anterior wall for a duration of 20–30 s. Multielectrode irrigated RF catheter (IMEA-group) (nMARQ, Biosense Webster) was also used to perform PVI, mostly in patients with persistent AF, as described before.4 The procedural endpoint of both RF based technologies was the documentation of PV entrance block using a 20-pole variable circular diagnostic catheter (Lasso 2515, Biosense Webster). No additional lesions were performed. The length of the ablation lesion for RF based technologies was measured along the ablation tags on the electroanatomical map taken during ablation. Cumulative RF time for the focal RF catheter and the sum of RF duration delivered by each electrode in the IMEA-group was calculated. Cryoballoon PVI was performed (CB-group) using the second generation CB (Arctic Front Advance, Medtronic, Minnesota, USA) as previously described.2 Using a single-freeze approach, the standard freezing duration was 180 s, but could be prolonged to 240 s at the physician’s discretion. No additional touch-up ablation was done after CB ablation. The procedural endpoint was documentation of PV entrance block using the inner-lumen circular catheter (Achieve, Medtronic). Energy transfer time for CB-PVI was calculated as the sum of the duration of all freezes. Lesion length for the CB-PVI was calculated by measuring the ostial circumference of the PV on the reconstructed pre-procedural cardiac magnetic resonance image.
Outcome and follow-up
Outcomes were measured based on the acute success of PVI, the recurrence of AF during follow-up and the reconnection of the PVs assessed in the subgroup of patients with repeat procedures due to AF recurrence. Episodes of AF or left atrial tachycardia lasting >30 s were considered a recurrence. Follow-up was performed at 3, 6 and 12 months after the procedure and included physical examination, 12-lead ECG and 7 day Holter-ECG monitoring. Repeat procedures in patients suffering from AF recurrence were performed using focal RF ablation in conjunction with an electroanatomical mapping system. Persistence of PVI was assessed using a 20-pole variable circular diagnostic catheter (Lasso 2515, Biosense Webster). PV reconnection was assessed with regard to the location and type of gap. A gap was defined as focal if it could be closed by a maximum of two RF lesions or as a segmental if more than two ablation points were needed to reisolate the PV. To investigate the relationship between hs-cTnT release and duration of energy application, the data of the duration of energy transfer and hs-cTnT release were included in the dataset of first procedures only.
Laboratory analysis
Blood samples were collected in fasting state on the morning before the procedure and 18–24 hours after the procedure. A hs-cTnT assay (Roche Elecsys 2010 high-sensitivity troponin T, Roche Diagnostics) with a 99th percentile concentration of 14 ng/L with a corresponding coefficient of variation of 10% at 13 ng/L was used. Ablation-induced hs-cTnT release was defined as the difference between the two hs-cTnT measurements. Standardised hs-cTnT release was calculated by dividing the hs-cTnT release by the duration of energy transfer (seconds) and by the length of the lesion (millimetres). In addition, CK and CK-MB isoenzyme values were assessed using enzyme test (Roche/Hitachi Cobas C System, Roche Diagnostics GmbH, Mannheim, Germany) and electrochemiluminescence immunoassay (Roche Cobas E System, Roche Diagnostics GmbH, Mannheim, Germany). The laboratory sets the normal value for CK between 38–157 U/L and for CK-MB at <5.0 µg/L and/or CK-MB/MB ratio >0.06 speaks in favour of myocardial damage. Ablation-induced CK and CK-MB release were defined as the difference between the measurements before and after the ablation.
Ablation safety assessment
Safety of the procedure was assessed based on acute complications and complications occurring within 3 months after ablation. We assessed the incidence of stroke or transient ischaemic attack (TIA), pericardial effusion/tamponade, pericarditis and periprocedural myocardial infarction. Transthoracic echocardiography was performed before ablation and within 2 hours after catheter ablation to rule out pericardial effusion or tamponade. Standard 12-lead ECG was acquired before ablation and the morning after the ablation. If patients experienced chest pain or if neurological symptoms were observed, standardised diagnostic work-up and therapy were provided. Postprocedural pericarditis was diagnosed if typical symptoms occurred within 36 hours after the procedure and required the administration of non-steroidal anti-inflammatory drugs.
Statistical analysis
Continuous variables are presented as mean±SD or as median and IQR. For continuous variables, comparisons were made using Student’s T-test, or Mann-Whitney U test, as appropriate. Discrete variables were compared using Fisher’s exact test. Association between hs-cTnT release and other parameters was tested using Spearman’s correlation and linear regression analysis without intercept. Univariable and multivariable logistic regression models using a stepwise forward procedure were constructed to assess the associations between the cTnT release with PVI outcome and safety, respectively. The multivariable models were adjusted for age, sex, hypertension, diabetes and coronary artery disease. P<0.05 was prespecified to indicate statistical significance. Statistical analysis was performed using SPSS V.22 (IBM SPSS Statistics, USA).
Results
Baseline data
We analysed 96 patients with a mean age of 59±10 years, and 82% were male. Median follow-up was 360 (151–423) days. To perform PVI, irrigated-tip RF catheter, irrigated multielectrode RF catheter and CB were used in 39 patients (40%), 17 patients (18%) and 40 patients (42%), respectively. There were significant differences between the groups in baseline characteristics: there were more patients with persistent AF in the IMEA-group, and these subjects differed significantly with regard to LVEF and left atrial size in comparison with two other groups (p<0.001). Baseline characteristics of the study groups are given in table 1.
Baseline characteristics of the study groups
Laboratory analysis
Hs-cTnT release after PVI was 806±413 ng/L, 864±262 ng/L and 840±331 ng/L, in the RF-group, IMEA-group and CB-group, respectively (p=0.809). A significant hs-cTnT increase occurred in all patients, independent of the ablation modality used. Correlation between the hs-cTnT release and the duration of energy application was identified in all study groups: RF-group (Spearman rho=0.584, p<0.0001), IMEA group (Spearman rho=0.529, p=0.024) and CB-group (Spearman rho=0.408, p=0.007). Lesion length did not correlate with hs-cTnT release (Spearman rho=0.053, p=0.641). A linear relationship between the duration of energy transfer and the hs-cTnT release was observed (R2=0.664) for the entire dataset. Further per-group analysis showed a strong linear relationship for the RF-group (R2=0.844, beta=0.398 [0.351–0.444]), the IMEA-group (R2=0.863, beta=0.162 [0.129–0.195] and the CB-group (R2=0.783; beta=0.463 [0.386–0.539]) (figure 1).
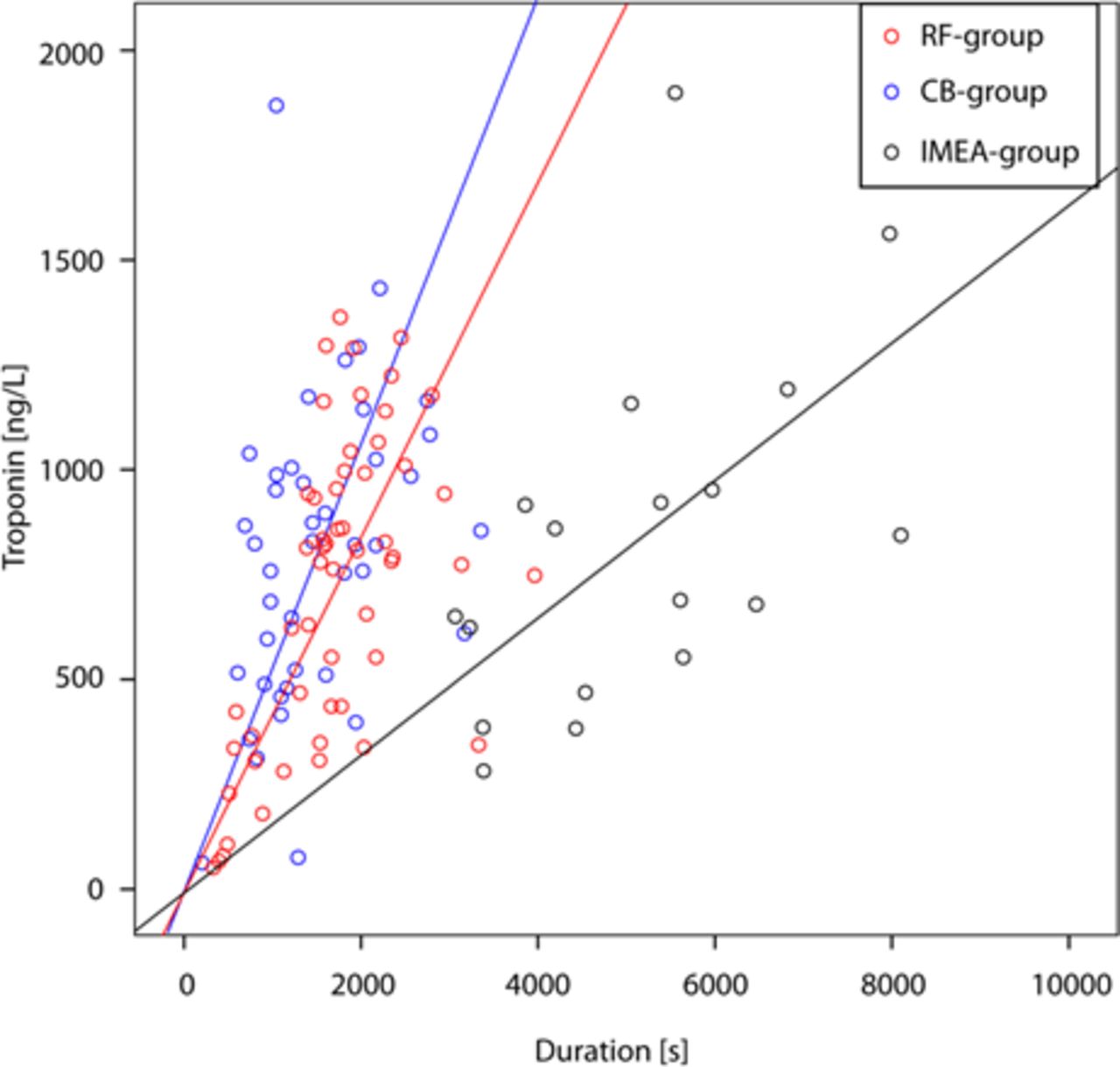
High-sensitive cardiac troponin T release and energy delivery duration for the RF-group, the IMEA-group and the CB-group. CB, second-generation cryoballoon ablation; IMEA, irrigated multi-electrode radiofrequency catheter ablation; RF – focal radiofrequency catheter ablation.
In addition, CK release was not significant and even negative in RF-group and IMEA-group, but was significantly higher in CB-group compared with the RF technologies (−2 vs −8 vs 116 U/L, p<0.001). Similar results were obtained for CK-MB release (table 1).
Hs-cTnT release and AF recurrence
Acute procedural success of PVI was achieved in all patients. After a follow-up of 12 months following the index procedure, AF recurrence was observed in 18 patients (45%) of the RF-group, in 5 patients (29%) of the IMEA-group and 14 patients (36%) of the CB-group, respectively (p=0.492). There were no significant differences between the patients with and without AF recurrence, except for the size of the LA (table 2).
Long-term follow-up data
Repeat PVI was performed in 26 of the 37 patients with AF recurrence. Reconnection of PVs was found in 23 out of the 26 patients with AF recurrence that underwent a repeat procedure. One, 2, 3 and 4 PVs were reconnected in 7, 12, 3 and 1 patient, respectively. For reisolation of these veins, a focal lesion was sufficient in 7 of 26 patients (27%). Patients with isolated PVs (n=3) or only one focally reconnected PVs (n=4) were not different from patients with segmentally reconnected veins in any of the investigated parameters (online supplementary table 1). In multivariable logistic regression, none of the analysed parameters could be identified as a predictor of AF recurrence after an index PVI procedure or of PV reconnection in the patients undergoing a repeat procedure (online supplementary table 2).
Supplemental material
Hs-cTnT release and ablation safety
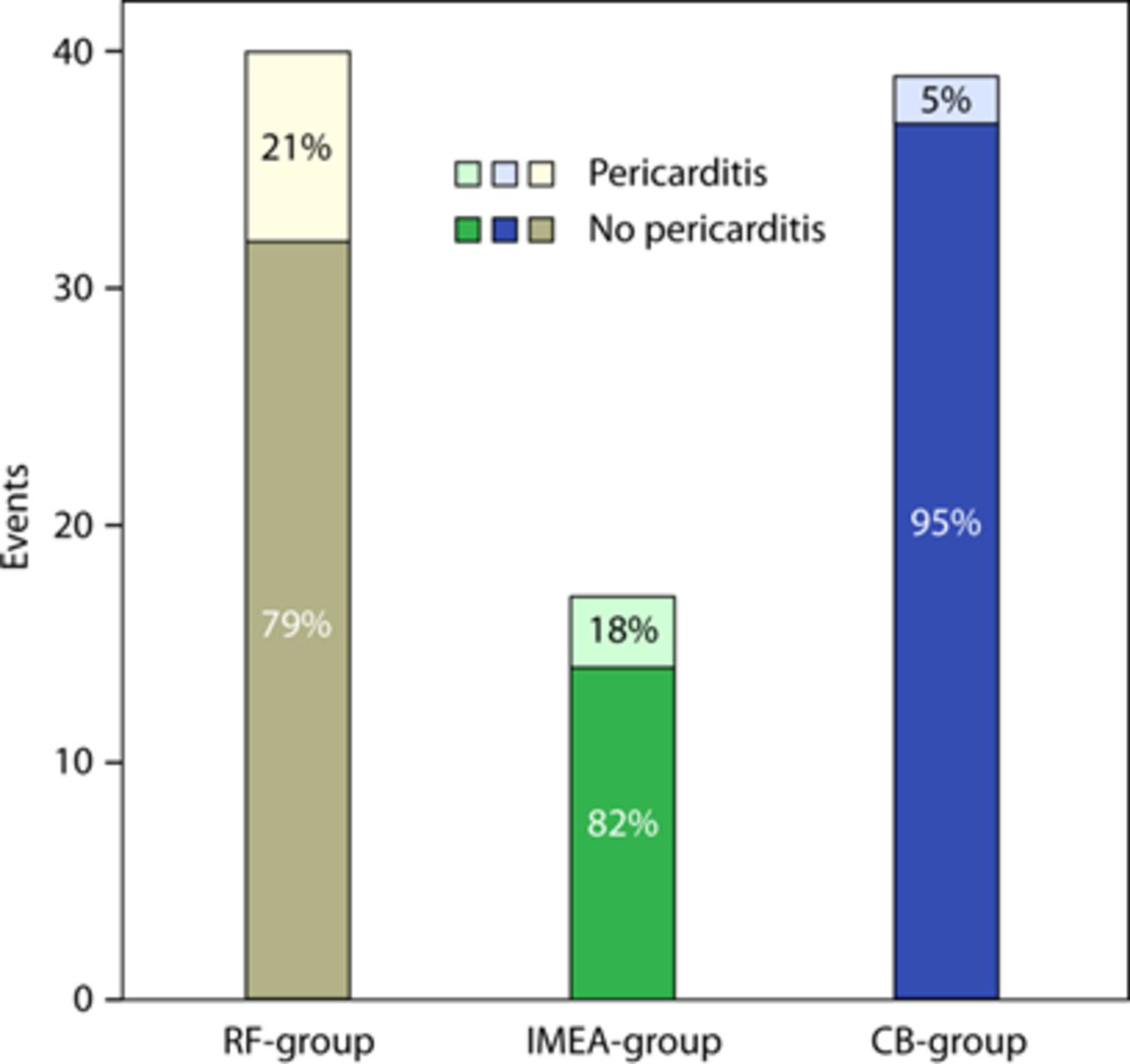
No patient had a procedure-related stroke/TIA or pericardial effusion/tamponade. Symptomatic pericarditis during the hospitalisation requiring the administration of non-steroidal anti-inflammatory drugs (ibuprofen) was diagnosed in 13 patients overall (13.5%): 8 patients of the RF-group (20.5%), 3 patients of the IMEA-group (17.6%) and 2 patients of the CB-group (5.1%) (p=0.113) (figure 2). With every hs-cTnT increase of 10 ng/L, the risk of a symptomatic pericarditis increased by 3%. The likelihood to develop symptomatic pericarditis after RF ablation PVI (RF-group and IMEA-group combined) was higher compared with CB ablation (19.6% vs 5.1%, p=0.046). CK and CK-MB release were not predictive for symptomatic pericarditis in study groups (p=0.447) (table 3). All cases of symptomatic pericarditis were successfully treated with the administration of non-steroidal anti-inflammatory drugs (Ibuprofen). Colchicine was not used for treatment in any of the cases. No recurrence or chronic pericarditis was noted during the follow-up period. Multivariable logistic regression (corrected for sex, age, BMI and hypertension) revealed that hs-cTnT release (ng/L) was the only independent predictor of symptomatic pericarditis (OR: 1.003 [1.001 to 1.005], p=0.015) after PVI. Lesion length and energy delivery duration were not predictive of symptomatic pericarditis (table 3).

{kind=link}
{kind=link}
Absolute and relative incidence of symptomatic pericarditis for the analysed ablation technologies. CB, second-generation cryoballoon ablation; IMEA, irrigated multielectrode radiofrequency catheter ablation; RF, focal radiofrequency catheter ablation.
Univariable and multivariable logistic regression analysis to predict pericarditis after PVI
Discussion
This is the first study to investigate the value of hs-cTnT measurements both to predict PVI efficacy (freedom from AF recurrence and persistence of PV isolation) and safety after a first PVI procedure using RF catheters (focal and multielectrode) and the second-generation CB. The main findings of this study are: (1) Hs-cTnT release after PVI was significant but was not different between the patient groups undergoing PVI with three different ablation technologies. (2) CK-MB release after PVI was significantly higher when using CB in comparison to RF technologies. (3) Hs-cTnT was neither identified as a significant predictor of AF recurrence (4) nor as a predictor of PV reconnection in patients undergoing a redo procedure. (5) Hs-cTnT release was predictive of postprocedural symptomatic pericarditis; however, CK-MB release was not.
Hs-cTnT release with ablation
Despite all technological improvements, a direct feedback or measure of the efficacy and the durability of an individual lesion or an entire lesion set are scarce.2 10–12 Hs-cTnT release has proven to be a reliable marker of myocardial cell damage and has been investigated for PVI performed using different technologies.8–10 In this study, acute success of PVI was achieved regardless of the technology used and a significant hs-cTnT release with PVI was observed in all cases. We could confirm the relationship between the total energy delivery duration and hs-cTnT release for investigated ablation technologies, as reported previously.13 14 However, no significant difference in hs-cTnT release after the PVI was observed between the technologies. On the contrary, CK-MB release was significantly higher after CB PVI, which is in accordance with previous results.15 16 Although most previous studies reported longer CB ablation time, the cumulative energy delivery time was longest for the IMEA-group.8 15–19 However, this was not reflected by the hs-cTnT release. The reason for this is unclear, but it could be hypothesised that this could occur especially with multielectrode ablation due to lack of contact of one or several electrodes with the tissue during the ablation. Contrary to our results, several previous studies showed higher myocardial injury assessed by troponin release after CB ablation when compared with RF ablation.8 10 15–17 We used high-sensitive troponin T release in our study, which could explain the mentioned differences at least to some extent. Namely, differences between troponin I and troponin T, as well as differences between the high-sensitive and the regular assays were proven.20–23 Our data are supported by the work by Herrera Siklody et al who also showed that there is no difference between hs-cTnT release after CB and RF ablation.24 This suggests that different biomarkers and different assays may not be 100% comparable in determining the myocardial damage in general, and especially in terms of AF ablation. In addition, our procedural data are different when compared with most other studies since we assessed only second generation CB ablation in a combined paroxysmal and persistent AF patient population and did not use additional focal RF or CB ablation for ‘touch-up’ isolation.8 15–19 Also, our data suggest rather short CB ablation time (1392 s); however, a relevant slowing of myocardial ice formation is typically reached within 3 min, which means that freezing cycle prolongation does not necessarily result in a larger lesion or more myocardial damage.2 15 25–28
Hs-cTnT release and AF recurrence
Documentation of myocardial injury by measuring hs-cTnT release is an unspecific quantitative marker of ablation and probably more so of the efficacy or durability of lesions applied during PVI. Despite the proven capability of hs-cTnT release to quantify myocardial injury with catheter ablation, controversial results have been reported to predict AF recurrence.8–10 13 14 The work by Lim et al showed that the cTnT levels after ablation, among other biomarkers including high-sensitive C-reactive protein, fibrinogen and D-dimers, were associated with early AF recurrence within the first 3 days, but not at 3 or 6 months.29 Wynn et al constructed the ‘Ablation Effectiveness Quotient’, the ratio between the hs-cTnT increase and the duration of RF ablation, which was a reliable predictor of long-term AF recurrence.14 On the contrary, several studies failed to identify cTnT as a predictor of long-term AF recurrence regardless of the ablation modality (RF, CB or Laser-balloon) in patients with paroxysmal and persistent AF13 14 30 which is in line with our results in patients with both paroxysmal and persistent AF. It is not surprising, especially for the RF-group, that the hs-cTnT release, as a non-qualitative measure of cumulative myocardial injury, does not predict the continuity of lesions of more than 10 cm around the ipsilateral veins. One single gap between the roughly 20 lesions around the veins may not be identified by troponin release, but results in electrical conduction with the potential to initiate a recurrence of AF. However, initially elevated values of hs-cTnT (>14 pg/mL) before the ablation were recognised as predictor of long-term AF recurrence, most probably as a sensitive marker of left ventricular and atrial remodelling and consequent elevated risk of AF recurrence.31 Moreover, we could not identify predictors of PV reconnection characteristics assessed during a redo procedure, among all analysed parameters including hs-cTnT and CK-MB.
Hs-cTnT release and ablation safety
Our data indicate low PVI procedural complication rates, regardless of the technology used, with the exception of pericarditis. As stated by the HRS/EHRA/ECAS consensus paper, pericarditis is a rarely reported, but almost certainly an underdiagnosed consequence of PVI ablation.1 11 32 The reported incidence of pericarditis after PVI in earlier studies was in the range of 0.1%–5% and clearly lower than the herein observed incidence (14%), especially when looking at the group of patients undergoing PVI using RF ablation (21%).1 11 32–34 However, the exact definition of pericarditis is often not specified in detail and the incidence of pericarditis is usually not systematically analysed. The diagnosis of pericarditis can be made based on symptoms, electrocardiographic changes and physical examination,32 and we did not assess inflammatory markers (white blood count, C reactive protein and so on) for additional confirmation or prediction of pericarditis. We used a symptom-driven definition and this might potentially explain this difference.
We observed that the hs-cTnT release was significantly associated with symptomatic pericarditis with an increase of 10 ng/mL elevating the risk by 3%. On the other hand, CK and CK-MB were not predictive for pericarditis, although CK-MB significantly differs between the study groups. Patients undergoing PVI using RF ablation (RF-group and IMEA-group combined) had higher likelihood to develop pericarditis in comparison to the CB-group. Ablation lesions during PVI are often large, transmural and lead to irritation and inflammation of the myocardium and pericardium.1 8–12 This may be related to the development of pericarditis. CB ablation resulted in a lower incidence of pericarditis despite comparable hs-cTnT release with the RF ablation and higher CK-MB release. One reason for this could be the spherical lesion formation with RF energy: to obtain a continuous transmural line with focal catheters with an interlesion distance of <6 mm, the heating is often deeper than the LA wall thickness. In addition, CB ablation creates sharper, more defined lesion demarcation than RF ablation. Also, there is a possibility that pericardial tissue reacts differently to heating and freezing. Ultimately, the different rate of symptomatic pericarditis could be due to more homogeneous energy transfer or to the larger contact area and consequently lower energy ‘density’ of the CB compared with RF technology. However, the exact reason remains speculative.1 2 8–11 31–34
Limitations
The results of the present study should be interpreted in the light of several limitations. First, this was a single-centre experience performed in a small group of patients. Second, baseline data between the three groups were significantly different in sex, AF type, and with regard to LVEF and LA size, mainly because the patients in the IMEA-group were more likely to have persistent AF and larger LA. Third, the nMARQ ablation catheter used for multielectrode ablation is currently not available on the market, but other multielectrode RF catheters are. Also, new balloon based multielectrode RF ablation catheters are currently being developed where similar types of procedural concerns might arise. Fourth, the definition of pericarditis was symptom driven, but stricter criteria for diagnosis probably would have underestimated the incidence of symptomatic pericarditis after PVI.
Conclusion
Hs-cTnT release after the PVI was significant but not different between focal RF ablation, multielectrode RF ablation and the second-generation CB. CK and CK-MB release were significantly higher after CB procedure in comparison to RF technologies PVI. Hs-cTnT release could neither be identified as a predictor of AF recurrence nor of persistent PV isolation. However, hs-cTnT was identified as a significant independent predictor of symptomatic pericarditis after PVI.
References
Footnotes
IZ and SK are joint first authors.
Contributors IZ, SK, NP: concept/design, data analysis/interpretation, drafting article, critical revision of article, approval of article. SK: concept/design, data analysis/interpretation, drafting article, critical revision of article, approval of article, statistics. NP: concept/design, data analysis/interpretation, drafting article, critical revision of article, approval of article, data collection. UC: data collection, data analysis/interpretation, drafting article, approval of article. FS, SB, DM, LP, TR, BAS, SO, CS, MK: data analysis/interpretation, critical revision of article, approval of article.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon request.