Article Text

Abstract
Aim Angina pectoris in the absence of obstructive coronary artery disease (CAD) is common and is associated with poor quality of life (QOL). Coronary microvascular endothelial dysfunction is associated with myocardial ischaemia and is a common cause of angina. We hypothesise that evaluation of coronary endothelial function, its diagnosis and treatment will favourably impact QOL in patients with angina symptoms and non-obstructive CAD.
Methods and results Follow-up was done on 457 patients with chest pain and non-obstructive coronary arteries who had undergone coronary vascular reactivity evaluation by administration of intracoronary acetylcholine at the time of diagnostic study. After a mean follow-up of 8.4±4.7 years, QOL was assessed by administration of the SF-36 QOL survey. Patients diagnosed and treated for microvascular endothelial dysfunction had a higher (better) overall mental composite score (44.8 vs 40.9, p=0.036) and mental health score (44.2 vs 40.7, p=0.047), and a trend towards higher vitality scores (39.1 vs 35.9, p=0.053) and role emotional scores (43.6 vs 40.4, p=0.073), compared with patients with normal endothelial function.
Conclusion Among patients with chest pain and normal coronaries, diagnosis and treatment of coronary microvascular endothelial dysfunction in those with angina pectoris and non-obstructive CAD are associated with better QOL compared with patients with normal endothelial function.
- microvascular endothelial function
- quality of life
- angina
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known about this subject?
Very little is known on the subject of quality of life (QOL) and coronary endothelial function.
No studies to our knowledge have specifically addressed the effects of diagnosis and treatment of coronary endothelial dysfunction on long-term QOL.
What does this study add?
In this manuscript we report the results of the impact of diagnosis and treatment of patients with coronary microvascular endothelial dysfunction and non-obstructive coronary artery disease (CAD) on long-term QOL.
These results demonstrate that among patients with chest pain and normal coronaries, the diagnosis and treatment of coronary microvascular endothelial dysfunction in those with angina pectoris and non-obstructive CAD are associated with better QOL compared with patients with normal endothelial function.
How might this impact on clinical practice?
The findings bring novel information to support the use of coronary endothelial function testing by skilled operators in the diagnosis of microvascular disease in patients with atypical chest pain that is not due to obstructive disease.
The results of the study suggest that the diagnosis and subsequent treatment of patients found to have microvascular disease may lead to an improvement in QOL.
Introduction
Angina pectoris with normal coronaries is a common phenomenon occurring in over 60% of patients undergoing coronary angiography in the USA.1 Patients with persistent chest pain and normal or non-obstructive coronary angiograms have poor quality of life (QOL) and consume large amounts of healthcare resources due to repeat evaluations for diagnostic and therapeutic uncertainty.2 3 Coronary microvascular endothelial dysfunction is associated with myocardial ischaemia4 and cardiovascular events,5–7 and can be an important mechanism for persistent chest pain in these patients.8
The identification and treatment of coronary microvascular endothelial dysfunction as a cause of angina in these patients may potentially modify their disease. Furthermore, recent studies have shown that reversal of endothelial dysfunction is associated with an improvement in cardiovascular prognosis.9 10 The effect of diagnosis and treatment of microvascular endothelial dysfunction on long-term QOL in patients with angina and normal angiograms has however not been studied.
Therefore, the aim of this study was to evaluate the impact of diagnosis and treatment of patients with coronary microvascular endothelial dysfunction and non-obstructive coronary artery disease (CAD) on long-term QOL.
Methods
Study design
This study is a prospective cohort study in a single centre.
Study population
The study group consisted of 457 patients with chest pain who were referred to the cardiac catheterisation laboratory for evaluation of CAD, found to have non-obstructive disease, and had comprehensive coronary physiology study including assessment of endothelial function and non-endothelium-independent coronary flow reserve.11–14
Exclusion criteria included significant coronary artery stenosis (>40%), ejection fraction <45%, unstable angina, previous myocardial infarction, use of radiographic contrast agents within 12 hours, significant systemic disease and pregnancy. Patients who did not return a follow-up questionnaire were excluded.
Study protocol
Medications that may affect cardiovascular haemodynamics were discontinued for at least 48 hours before the study. At baseline, diagnostic coronary angiography and determination of endothelium-dependent changes in Coronary Blood Flow (CBF) and endothelium-independent coronary flow reserve were performed as previously described.4 15 A Doppler guidewire (0.014-inch diameter, FloWire, Volcano) within a 2.2 F coronary infusion catheter (Ultrafuse, SciMed Life System) was advanced and positioned in the middle portion of the left anterior descending coronary artery (LAD). Intracoronary bolus injections of incremental doses (18–72 µg) of adenosine (Fujisawa), an endothelium-independent vasodilator (primarily of the microcirculation),16 were administered into the guiding catheter until maximal hyperaemia was achieved.
Assessment of the endothelium-dependent changes in CBF was performed by selective infusion of acetylcholine (ACh) into the LAD. ACh (Iolab Pharmaceuticals) 10−6, 10−5 and 10−4 mol/L were infused at 1 mL/min for 3 min.4 17 Haemodynamic data (heart rate and mean arterial pressure), Doppler measurements and coronary angiography were obtained after each infusion. Endothelium-independent epicardial vasodilation was assessed with an intracoronary bolus injection of nitroglycerin (200 µg, Abbott Laboratories).18
Microvascular endothelial function
Doppler flow velocity spectra were analysed online to determine the time-averaged peak velocity. Volumetric CBF was determined from the following relation: CBF=cross-sectional area × average peak velocity × 0.5.19 Endothelium-dependent microvascular function was calculated as % ∆ CBF in response to ACh as previously described.20 As previously reported microvascular endothelial dysfunction was defined as ≤50% increase in CBF in response to the maximal dose of ACh compared with baseline CBF.6 Patients were divided into two groups based on the presence of microvascular endothelial dysfunction.
Epicardial vascular function testing
Coronary artery diameter was analysed by quantitative coronary angiograms from digital images using a modified, previously described technique from this institution.4 13 The LAD was divided into proximal, middle and distal segments. For each segment, the measurements were performed in the region where the greatest change had occurred during the ACh infusion. An angiographically smooth segment of the proximal, middle and distal LAD, free of any overlapping branch vessels, was identified in each patient and served as the reference diameter for the calculation of diameter stenosis. End-diastolic cine frames that best showed the segment were selected and calibration of the video and cine images was done, identifying the diameter of the guide catheter. Quantitative measurements of the coronary arteries were obtained using a computer-based image analysis system. Segment diameters were determined at baseline and after both ACh and nitroglycerin administration. The proximal segment was not exposed to ACh and thus served a control segment.
Epicardial coronary endothelial dysfunction was defined as a decrease or no increase in coronary artery diameter in response to the maximal dose of ACh compared with baseline.21
Follow-up
After a mean follow-up of 8.4±4.7 years, QOL was assessed by administration of Short Form (36) Health (SF-36) survey.22 Patients were contacted by mail and the SF-36 survey sent to them.
Survey instrument
The SF-36 survey is a well-validated, multipurpose, short-form health survey with 36 questions. It is an 8-scale profile of functional health, well-being and mental health that forms a generic measure of participants’ perception of their health status and their mental and physical well-being (figure 1).22–25
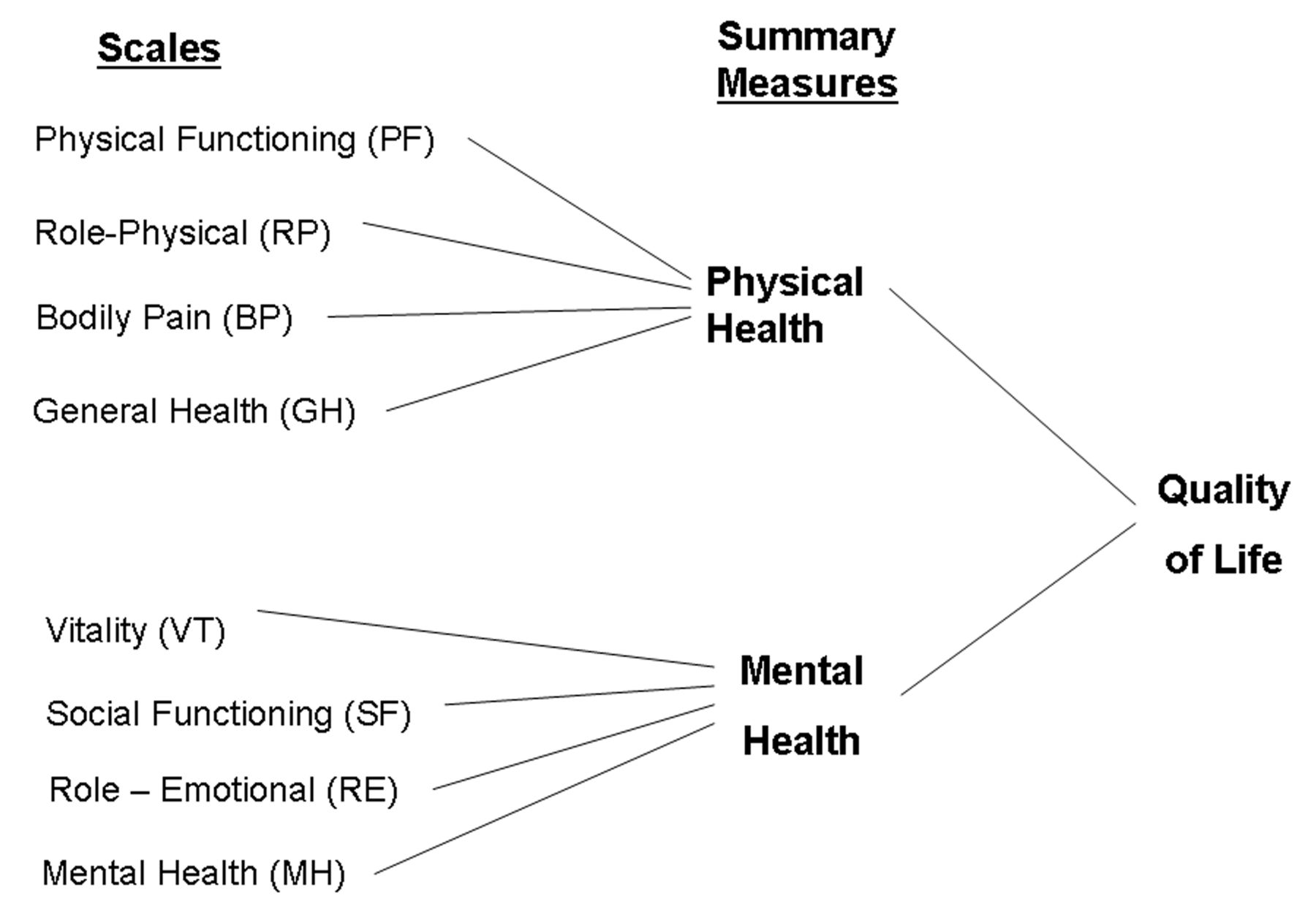
Summary of the measures and scales of the quality of life SF-36 survey.
Statistical analysis
Data are displayed as mean±SD or count and percentage as appropriate. Variables with heavily skewed distribution are reported as medians with first and third quartiles in parenthesis. Analysis to compare different demographic and baseline clinical data between the groups was performed using analysis of variance for continuous data and the Pearson’s χ2 test for categorical data. Baseline data for the CBF, CFR and coronary artery diameter were compared using a rank-sum test. Statistical analyses were performed using JMP V.14 (SAS Institute, Cary, NC, 1989–2018).
Quality of life
The responses to the SF-36 items for the 8-scale SF-36 scale were scored using the publisher’s normative methods, which in turn generated the summary physical and mental components scores. All of these scores are standardised such that in a normal age-matched and sex-matched reference population the mean score is equal to 50 and the SD of the scores is equal to 10. Patients who have SF-36 scores greater than 50 report better health-related QOL than the normal population, and scores less than 50 indicate poorer QOL. Differences between the groups in the QOL analysis were compared using Student’s t-test. Multiple linear regression was used to estimate the difference in QOL adjusted for other covariates. The model was adjusted for covariates which included the baseline characteristics (reported in table 1) as well as the medication use at baseline (reported in table 2). All statistical tests were two-sided, and a p<0.05 was considered to be statistically significant.
Baseline patient characteristics, by microvascular function
Medication use, by microvascular function
Results
Therefore 457 patients were included in the study, of whom 258 (56%) had microvascular endothelial dysfunction. There were 313 women (68%), and the mean age of the study population was 52 years (range, 17–78 years). Most patients (92%) had >1 risk factor for CAD. The mean duration of follow-up was 8.4±4.7 years.
Baseline characteristics
Patients with microvascular dysfunction were slightly older compared with patients with normal endothelial function (mean age 54 vs 51, p=0.028) and had a lower smoking rate. The groups were otherwise well matched at baseline with regard to gender, race, other cardiovascular risk factors and inflammatory marker (table 1).
Medications at baseline
Patients with microvascular dysfunction had a higher rate of lipid-lowering drugs use (43% vs 33%, p=0.032) and a lower rate of aspirin use (43% vs 52%, p=0.06) (did not reach statistical significance) compared with patients with normal microvascular function. The two groups matched well on the frequency of use of other cardiac medications including beta-blockers, ACE inhibitors use and calcium channel blockers (table 2).
Microvascular and epicardial endothelial function
Patients in the microvascular coronary dysfunction group had a lower mean per cent change in CAD after maximal dose of ACh from baseline (greater vasoconstriction) compared with patients with normal microvascular endothelial function (−25.7% vs −3.8%, p<0.001). There was also a higher percentage of patients with epicardial endothelial dysfunction (58% vs 16%, p<0.001) in the microvascular coronary dysfunction group compared with the group with normal microvascular endothelial function.
Quality of life
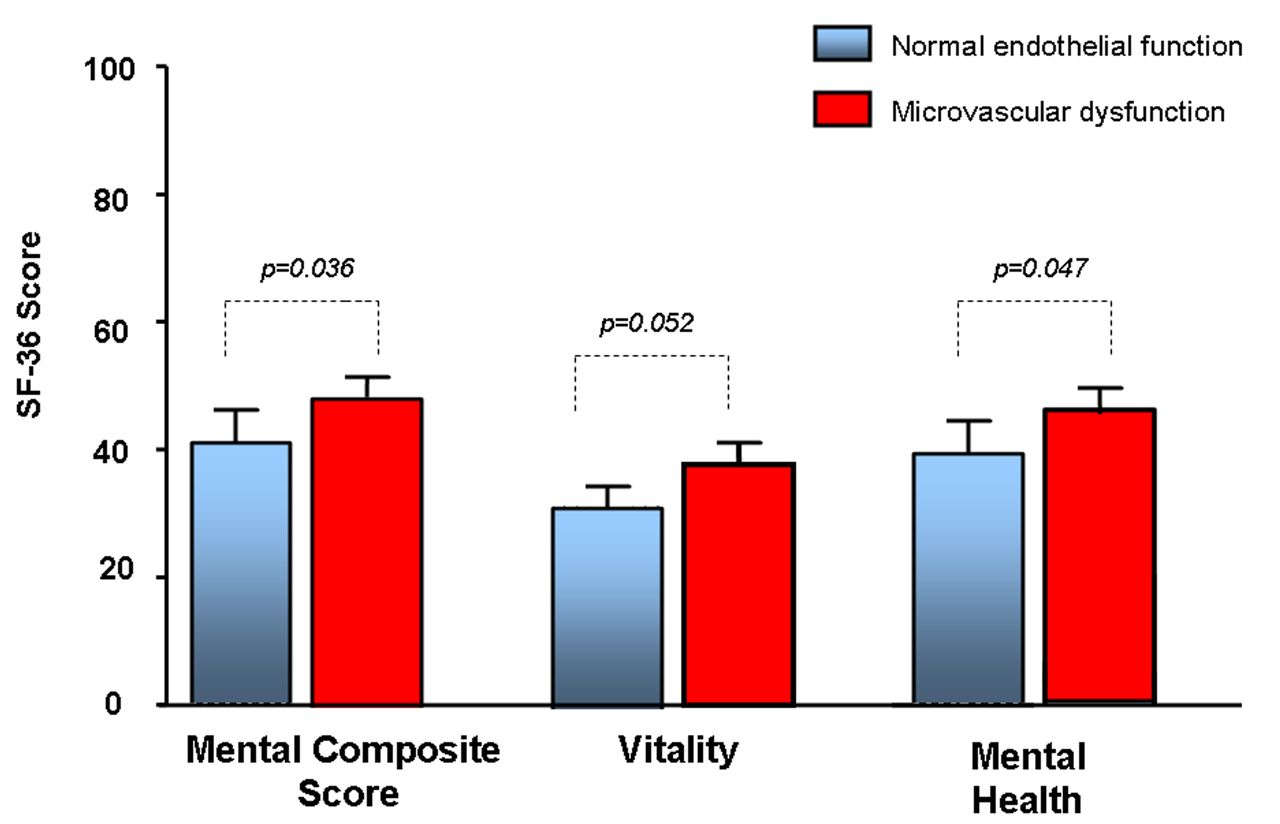
At the time they were surveyed, patients who were diagnosed and treated for microvascular endothelial dysfunction experienced higher overall mental composite score (44.8 vs 40.9, p=0.036) and mental health (44.2 vs 40.7, p=0.047), and a trend towards higher vitality (39.1 vs 35.9, p=0.053) and role emotional (43.6 vs 40.4, p=0.073), compared with patients with normal endothelial function (table 3 and figure 2).

Short Form (36) Health (SF-36) survey mental composite score, vitality and mental health in patients with microvascular endothelial dysfunction compared with patients with normal microvascular functions.
Endothelial function and Short Form (36) Health (SF-36) survey results, by microvascular function
Subgroup analysis of women
On subgroup analysis, women with microvascular endothelial dysfunction had similar baseline characteristics, frequency of cardiovascular risk factors, inflammatory markers and use of cardiovascular medication compared with women with normal microvascular endothelial function.
On QOL analysis women diagnosed and treated for microvascular endothelial dysfunction had a higher physical function (44.5 vs 40.4, p=0.039), general health (43.4 vs 38.7, p=0.016) and vitality (42.1 vs 37.3, p=0.008), and a trend towards higher overall mental composite score (46.8 vs 43.4, p=0.08), overall physical composite score (41.1 vs 37.3, p=0.05), role emotional (46.5 vs 43.2, p=0.09), social function (44.8 vs 41.4, p=0.08) and role physical (42.1 vs 38.9, p=0.09), compared with women with normal endothelial function (table 4 and figure 3).

{kind=link}
{kind=link}
{kind=link}
SF-36 physical functioning, vitality and general health in women with microvascular endothelial dysfunction compared with women with normal microvascular functions.
Women and SF-36 results by microvascular function
Discussion
The current study demonstrated that among patients with chest pain and non-obstructive CAD, QOL with respect to measures of mental well-being during long-term follow-up is better in those patients who were assessed, diagnosed and received treatment for microvascular endothelial dysfunction compared with those who are found to have normal endothelial function. The current study suggests that assessment and treatment of microvascular angina may improve their QOL.
Patients with chest pain and non-obstructive CAD have been shown to have high morbidity and mortality than previously thought.26 27 These patients constitute a large percentage (up to 50%) of patients who undergo coronary angiography studies for suspected myocardial ischaemia.28 These patients face diagnostic uncertainty and are high users of healthcare resources,26 29 30 due to the perceived need for frequent hospitalisation and multiple angiograms.31 They also have poor QOL, functional disability and limitations in activities of daily living.26 32 33
The aetiologies for chronic chest pain encompass a wide array of potential diagnoses, including cardiac and non-cardiac causes. Recent evidence suggests ischaemia due to coronary microvascular or macrovascular endothelial dysfunction34–37 may play a role, especially in women.28 37–40 Furthermore, the presence of microvascular dysfunction is associated with adverse cardiovascular events and its treatment may lead to improved prognosis.4 The need for proper diagnosis of chest pain in these patients is underscored by the recent guidelines and endorsement by the European Society of Cardiology. To our knowledge there are no studies in patients with chest pain showing the effect of diagnosis and treatment of microvascular endothelial dysfunction on QOL.
Our finding of higher QOL scores in patients with microvascular endothelial dysfunction who were on treatment compared with patients with normal endothelial function may seem paradoxical. Previous studies have however found similar results. In one study women with chest pain and myocardial ischaemia had a higher QOL compared with women without.41 There are several potential mechanisms for this observation. First, lack of diagnosis for chest pain is a source of frustration for both the physician and the patient. Conversely, establishment of a diagnosis may alleviate anxiety for the patients, which would lead to improvement in the measures within the mental domains of QOL. Similar observations have also been made in patients admitted to hospitals for evaluation of suspected myocardial infarction. Patients in whom acute myocardial infarction was not confirmed reported more cardiovascular symptoms of chest pain, dyspnoea and palpitations, as well as more psychosomatic and psychological parameters, at 1 year compared with patients diagnosed with acute myocardial infarctions.42 Furthermore patients with unstable angina pectoris are likely to experience poorer QOL following an acute hospitalisation than patients with other types of acute coronary syndrome.43 Second, the treatment of microvascular dysfunction may relieve their symptoms, which may improve QOL. Previous studies have shown that treatment of angina is associated with improvement in physical, mental and social domains of QOL.44 Third, the paradoxical finding of better QOL in women with ischaemia compared with those without ischaemia41 45 may also in part explain our finding. Patients able to exercise to a sufficient workload to elicit an ischaemic response may have better QOL because they are less functionally impaired.41 The mechanism is thought to be due to less functional impairment in women with myocardial ischaemia compared with women without myocardial ischaemia. We have previously shown that microvascular coronary disease is associated with myocardial ischaemia in patients with non-obstructive coronary disease.4 Although we did not specifically measure the exercise tolerance of our patients, it may be speculated that a similar mechanism may play a role in patients with chest pain and impaired microvascular function.
Persistent chest pain in the absence of coronary disease is more prevalent in women.46 47 Indeed, we found in our study a higher percentage of women having microvascular endothelial dysfunction compared with men. In a subgroup analysis, the differences in QOL were more marked among women. We speculate that microvascular disease is thus more prevalent women, and its diagnosis and treatment may have greater benefit compared with men. The current study further supports the notion that coronary microvascular dysfunction is one of the main mechanisms of chest pain in women.
Limitations
There are several limitations to be mentioned. No baseline QOL scores were obtained. Although the characteristics of the two groups were similar at baseline, including cardiovascular risk factors and medication use, we do not have baseline QOL data for comparison. This precludes stronger inference about the cause and effect of any findings. In addition there was no standardised treatment protocol for patients with microvascular disease, and the attending clinician determined the treatment based on the patient’s risk factors. We thus cannot draw definite conclusion on the effect of a specific treatment on QOL. In addition, we were unable to ascertain the medication use at follow-up and verify it with medical records because many of the patients did not follow up in our institution.
Our study was not designed to measure healthcare utilisation and functional status or to do cost analysis of potential healthcare saving of diagnosis and treatment of microvascular disease in patients with chest pain. This would have provided more outcome benefits, which could potentially be linked to improved QOL.
Conclusions
Among patients with chest pain and non-obstructive CAD or normal coronary arteries, it is suggested that the diagnosis and subsequent treatment of patients found to have microvascular disease may lead to an improvement in QOL. These results support the use of coronary endothelial function testing by skilled operators in the diagnosis of microvascular disease in patients with atypical chest pain that is not due to obstructive CAD.
References
Footnotes
Contributors The authors of the paper take full responsibility.
Funding The study was supported by grants from the NIH (NIH K24 HL-69840, NIH R01 HL-63911, HL-77131, HL 92954, HL 085307, DK 73608) and the Mayo Foundation.
Competing interests None declared.
Patient consent for publication Obtained.
Ethics approval The Mayo Clinic Institutional Review Board approved the study.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.