Article Text

Abstract
Background Oral anticoagulation (OAC) therapy guidelines recommend using CHA2DS2-VASc to determine OAC need in atrial fibrillation (AF). A usable tool, CHA2DS2-VASc is challenged by its predictive ability. Applying components of the complete blood count and basic metabolic profile, the Intermountain Mortality Risk Score (IMRS) has been extensively validated. This study evaluated whether use of IMRS with CHA2DS2-VASc in patients with AF improves prediction.
Methods Patients with AF undergoing cardiac catheterisation (N=10 077) were followed for non-fatal stroke and mortality (mean 5.8±4.1 years, maximum 19 years). CHA2DS2-VASc and IMRS were calculated at baseline. IMRS categories were defined based on previously defined criteria. Cox regression was adjusted for demographic, clinical and treatment variables not included in IMRS or CHA2DS2-VASc.
Results In women (n=4122, mean age 71±12 years), the composite of non-fatal stroke/mortality was stratified (all p-trend <0.001) by CHA2DS2-VASc (1: 12.6%, 2: 22.8%, >2: 48.1%) and IMRS (low: 17.8%, moderate: 40.9%, high risk: 64.5%), as it was for men (n=5955, mean age 68±12 years) by CHA2DS2-VASc (<2: 15.7%, 2: 30.3%, >2: 51.8%) and IMRS (low: 19.0%, moderate: 42.0%, high risk: 65.9%). IMRS stratified stroke/mortality (all p-trend <0.001) in each CHA2DS2-VASc category.
Conclusions Using IMRS jointly with CHA2DS2-VASc in patients with AF improved the prediction of stroke and mortality. For example, in patients at the OAC treatment threshold (CHA2DS2 -VASc = 2), IMRS provided ≈4-fold separation between low and high risk. IMRS provides an enhancing marker for risk in patients with AF that reflects the underlying systemic nature of this disease that may be considered in combination with the CHA2DS2-VASc score.
- atrial fibrillation
- stroke
- risk factors
- mortality
- gender
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0
Statistics from Altmetric.com
Key questions
What is already known about the subject?
The CHADS2 and CHA2DS2-VASc scores are the most widely used models for risk-guided provision of OAC to AF patients.
A meta-analysis evaluated the CHADS2 and CHA2DS2-VASc scores and reported some of the best c-statistics for these scores at 0.685 and 0.675, respectively; values that suggest limited predictive ability for stroke.
As such new tools are need to work with these prior scores or independently that can dynamically assess stroke risk.
What does this study add?
The sex-specific IMRS derived from commonly ordered physiologic tests and the CHA2DS2-VASc score were significant independent risk predictors of a composite of stroke or mortality among AF patients.
IMRS adds to the CHA2DS2-VASc across all risk profiles and has the promise to add dynamic understanding of risk assessment to baseline risk factors.
How might this impact on clinical practice?
This study serves as a foundation for better modeling of risk in AF patients with a combination of both the CHA2DS2-VASc risk score and IMRS.
Dynamic markers of risk can assist in understanding of severity of individual risk factors, response to therapeutic changes or lifestyle modifications, and can augment or lower risk over time to better identify patients at need for long-term anticoagulation.
Atrial fibrillation (AF) is a complex, systemic disease that is marked by structural and electrophysiological remodelling of atrial tissue.1 AF results in various clinical manifestations with differing symptoms, yet all patients with AF are at a higher risk of thromboembolism spanning across multiple comorbid states.2 Strokes among patients with AF are associated with greater levels of other morbidities and earlier mortality.3 Oral anticoagulation (OAC) is a mainstay of antithrombotic therapy, and based on current guidelines, OAC should be provided to patients according to a risk-optimised approach.
The CHADS2 and CHA2DS2-VASc scores are the most widely used models for risk-guided provision of OAC to patients with AF.1 In recognition of a potential higher-than-expected risk with lower CHA2DS2-VASc scores and a more favourable benefit/risk profile with direct oral anticoagulants (DOACs), the most recent European Society of Cardiology guidelines recommend use in patients with a CHA2DS2-VASc score of 1 or higher.4 A meta-analysis evaluating the CHADS2 and CHA2DS2-VASc scores reported some of the best c-statistics for these scores at 0.685 and 0.675, respectively, although these values suggest limited predictive ability for stroke.5 Despite their limitations, these scores are simple to memorise and calculate in one’s head and thus are widely used, but by design they sacrifice their predictive ability to be feasible for use in clinical practice.6 Additionally, these scores are composed of static, dichotomous baseline variables and as a consequence predict higher risk once risk factors become present regardless of whether the patient’s health improves.
A risk prediction tool for clinical decision-making that incorporates pertinent risk information not included by CHADS2 and CHA2DS2-VASc and is feasible to use in clinical practice could improve the precise identification of patients with AF who do, and those who do not, need OAC. The Intermountain Mortality Risk Scores (IMRSs) are potentially such clinical decision tools that have been extensively validated to stratify risk of morbidity and mortality in a wide variety of cardiovascular and non-cardiac patient populations.7–9 IMRS models are adaptive and dynamic because they use risk factors that vary over time due to changes (including improvements) in physiological status, pharmacological therapies and lifestyles. This study evaluated whether the combination of CHA2DS2-VASc and IMRS can improve risk stratification in the AF population.
Methods
Study population
The study population consisted of adult patients (ages ≥18) with AF who were evaluated by cardiac catheterisation at the Intermountain Heart Institute from October 1993 through December 2015 and who also had both complete blood count (CBC) and basic metabolic profile (BMP) values measured. This was a retrospective analysis of prospectively collected observational data from the Intermountain Healthcare electronic data warehouse that consists of an electronically mirrored copy of clinical health records for administrative and research use. CHA2DS2-VASc was calculated based on previously established criteria10 and IMRS was computed based on previously derived sex-specific weightings of age and the components of the CBC and BMP laboratory panels.7–9 11
Laboratory analysis and risk calculation
IMRS values were generated using subject age, sex, and CBC and BMP laboratory measurements at the time of inclusion into the study.12 IMRS was derived in 2009 as a sex-specific linear combination of weighted regression coefficients for the following risk predictors: haematocrit, mean corpuscular volume, red cell distribution width, mean corpuscular haemoglobin concentration, platelet count, mean platelet volume, white blood cell count, sodium, potassium, bicarbonate, creatinine, glucose, calcium and age. CBC panels were analysed on Coulter haematology analysers (Beckman Coulter, Hialeah, Florida, USA) until 2012 or on Sysmex haematology analysers (Sysmex America, Lincolnshire, Illinois, USA) beginning in mid-2012, and reported values were normalised to ensure concordance in the population. BMP panels were tested using a Vitros clinical chemistry system (Ortho Clinical Diagnostics, Raritan, New Jersey, USA).
IMRS scores were calculated for all patients and divided into groups of low, moderate and high risk based on thresholds reported in prior publications.9 12 The risk categories for IMRS among men were <11, 11–16 and ≥17, respectively, using the 1-year mortality IMRS formula. For women, IMRS categories of low, moderate and high risk were scores of <9, 9–14 and ≥15, respectively, for 1-year IMRS calculations.
Study endpoints
Due to an inability to obtain cause of death information on approximately one-third of patients and because of the relatively low frequency of non-fatal stroke, the primary outcome in this study was all-cause mortality or non-fatal stroke within pre-specified groups of IMRS and CHA2DS2-VASc. Death outcomes were determined from a combination of Intermountain Healthcare electronic records, Social Security Administration death master file and State of Utah death certificates. Stroke outcomes were obtained electronically from Intermountain records based on International Classification of Diseases codes, with both ischaemic and haemorrhagic stroke included in the outcomes under the assumption that any event not predicted by the risk scores in this study would be randomly distributed across risk categories. Those outcomes labelled as stroke were all admissions to a medical facility with a non-fatal stroke. The study cohort was also evaluated for non-fatal stroke and for mortality separately.
Statistical considerations
Survival analyses were performed to evaluate the association of CHA2DS2-VASc and of IMRS with study outcomes for up to 19 years of follow-up. Survival curves were generated using the Kaplan-Meier method. Cox proportional-hazards models were constructed separately for men and women to evaluate CHA2DS2-VASc and IMRS in univariable analysis and together in bivariable modelling. Cox regression was evaluated for IMRS within strata defined by CHA2DS2-VASc, categorised by previously derived thresholds of low, medium or high risk for mortality.9 12 Cox regression was also used to evaluate multivariable adjusted associations of the risk scores with outcomes for 20 variables that were not included in the risk scores (hyperlipidemia, family history of coronary disease, history of or current smoking, presentation (unstable angina or acute myocardial infarction), history of renal failure, chronic obstructive pulmonary disease, depression, number of diseased coronary arteries (70% or greater stenosis), treatment with ablation, treatment with percutaneous coronary intervention or coronary bypass surgery, and discharge prescription of an anticoagulant, aspirin, antiplatelet, statin, beta-blocker, calcium channel blocker, diabetes medication, diuretic, ACE inhibitor or angiotensin receptor blocker).
Stratified analyses were performed in which IMRS associations with study outcomes were evaluated in CHA2DS2-VASc categories defined by scores ≤1, 2 and ≥3. Kaplan-Meier survival curves were created for IMRS risk groupings within each of those CHA2DS2-VASc strata. Cox regressions for the association of IMRS with outcomes were performed as described above but within CHA2DS2-VASc categories and for the association of joint CHA2DS2-VASc/IMRS categories instead of with CHA2DS2-VASc included in the modelling. The receiver operator characteristic curve was evaluated to determine c-statistics describing the predictive ability of risk scores for study outcomes. Predictive values were calculated for positive predictive value (PPV), negative predictive value (NPV), sensitivity, specificity and accuracy. Two-sided statistical tests were evaluated using SPSS V.23 (IBM SPSS Statistics) with a p value of ≤0.05 designated as statistically significant.
Results
Baseline characteristics of women (n=4122) and men (n=5955) are shown in table 1. The composite of non-fatal stroke or mortality was predicted among women by CHA2DS2-VASc categories (1: 12.6%, 2: 22.8%, >2: 48.1%; p-trend <0.001) and by IMRS (low-risk: 17.8%, moderate-risk: 40.9%, high-risk: 64.5%; p-trend <0.001). This was also the case for men, with both CHA2DS2-VASc (<2: 15.7%, 2: 30.3%, >2: 51.8%; p-trend <0.001) and IMRS (low risk: 19.0%, moderate risk: 42.0%, high risk: 65.9%) predicting the primary outcome. Kaplan-Meier survival curves displaying these outcomes are shown in figure 1. In Cox regression entering both IMRS and CHA2DS2-VASc (table 2), both risk scores remained significant among both women and men, although the association of CHA2DS2-VASc with stroke or mortality was reduced compared with univariable analysis (beta-coefficients for CHA2DS2-VASc of 2 and >2 in women and men were reduced by 30%–37% in bivariable analyses). Changes to the association of IMRS with outcomes were impacted less (beta-coefficients for IMRS in Cox regression were 16%–27% lower for moderate and high-risk groups in women and men). Results were similar to this after further multivariable adjustment in Cox regression.
Baseline characteristics
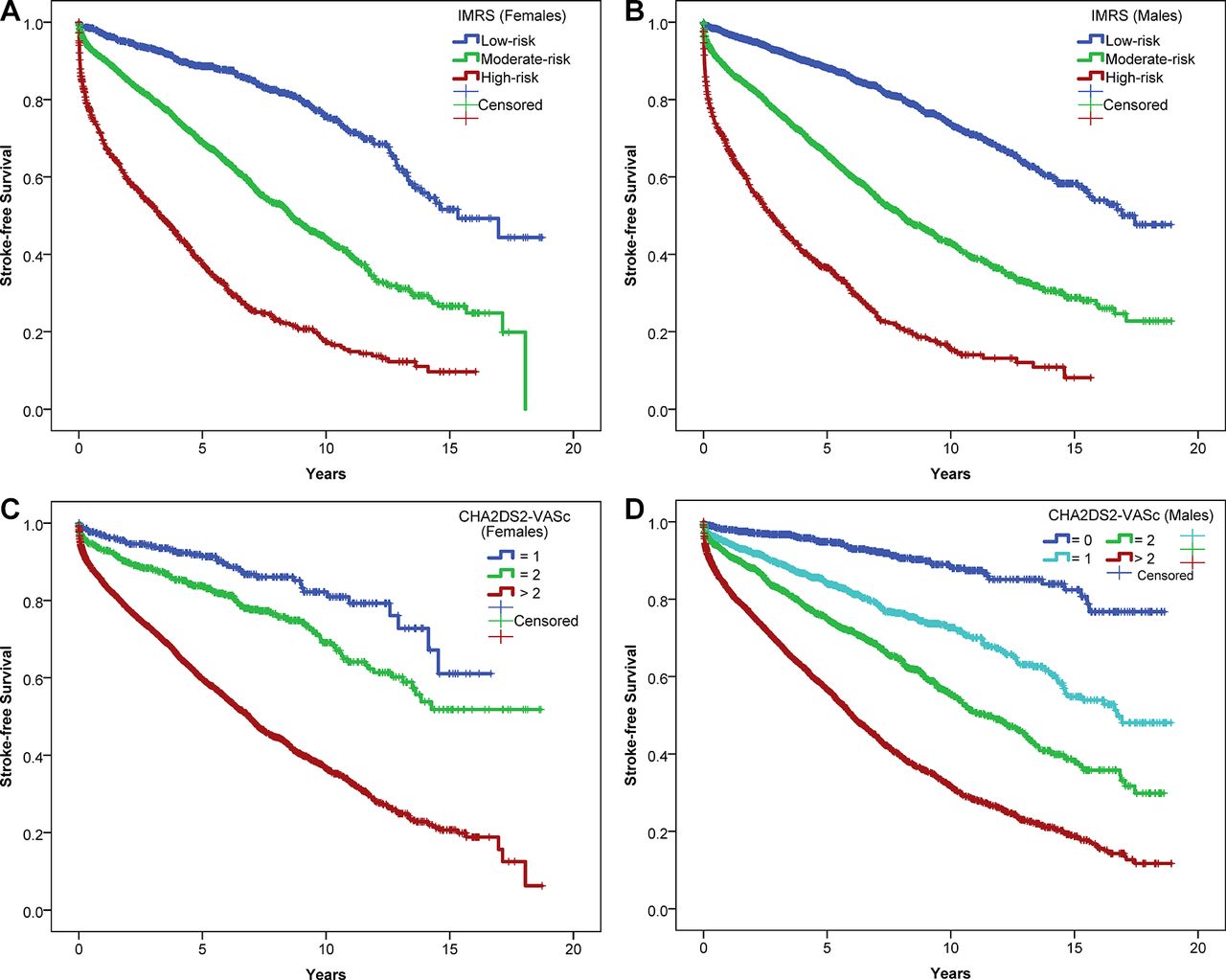
Kaplan-Meier survival curves for non-fatal stroke or mortality based on IMRS categories among (A) women (p-trend <0.001, low risk: n=996, moderate risk: n=2129, high risk: n=997) and (B) men (p-trend <0.001, low risk: n=2373, moderate risk: n=2791, high risk: n=791), and CHA2DS2-VASc categories among (C) women (p-trend <0.001, 1: n=357, 2: n=648, >2: n=3117) and (D) men (p-trend <0.001, 0: n=659, 1: n=1088, 2: n=1463, >2: n=2745). IMRS, Intermountain Mortality Risk Score.
Cox regression of IMRS and CHA2DS2-VASc associations with non-fatal stroke or mortality and with each endpoint individually
Evaluation of predictive ability for women found c-statistics of c=0.683 for CHA2DS2-VASc and c=0.706 for IMRS for stroke or mortality. For men, c-statistics were c=0.706 for CHA2DS2-VASc and c=0.716 for IMRS. The PPV, NPV, sensitivity, specificity and accuracy for women and men are shown in online supplementary table s1, including for the composite endpoint and for each endpoint individually, demonstrating poor PPV (as is typical for all prognostic scores) and limited other predictive value except for sensitivity when examining the combined intermediate and high-risk groups. Examination of the high-risk groups compared with the low-risk and intermediate-risk groups revealed that both CHA2DS2-VASc and IMRS had strong NPV and specificity but limited PPV and sensitivity.
Supplemental material
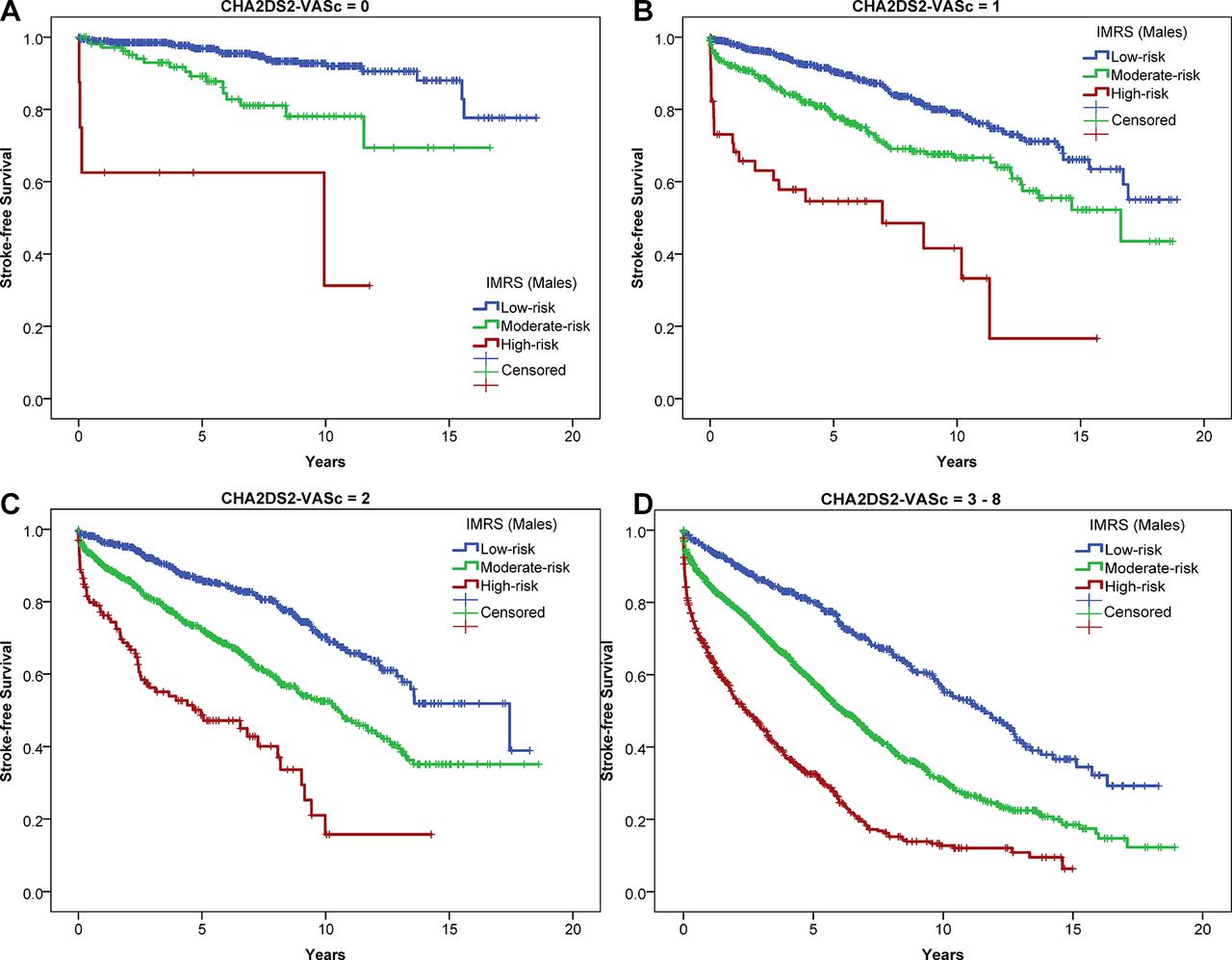
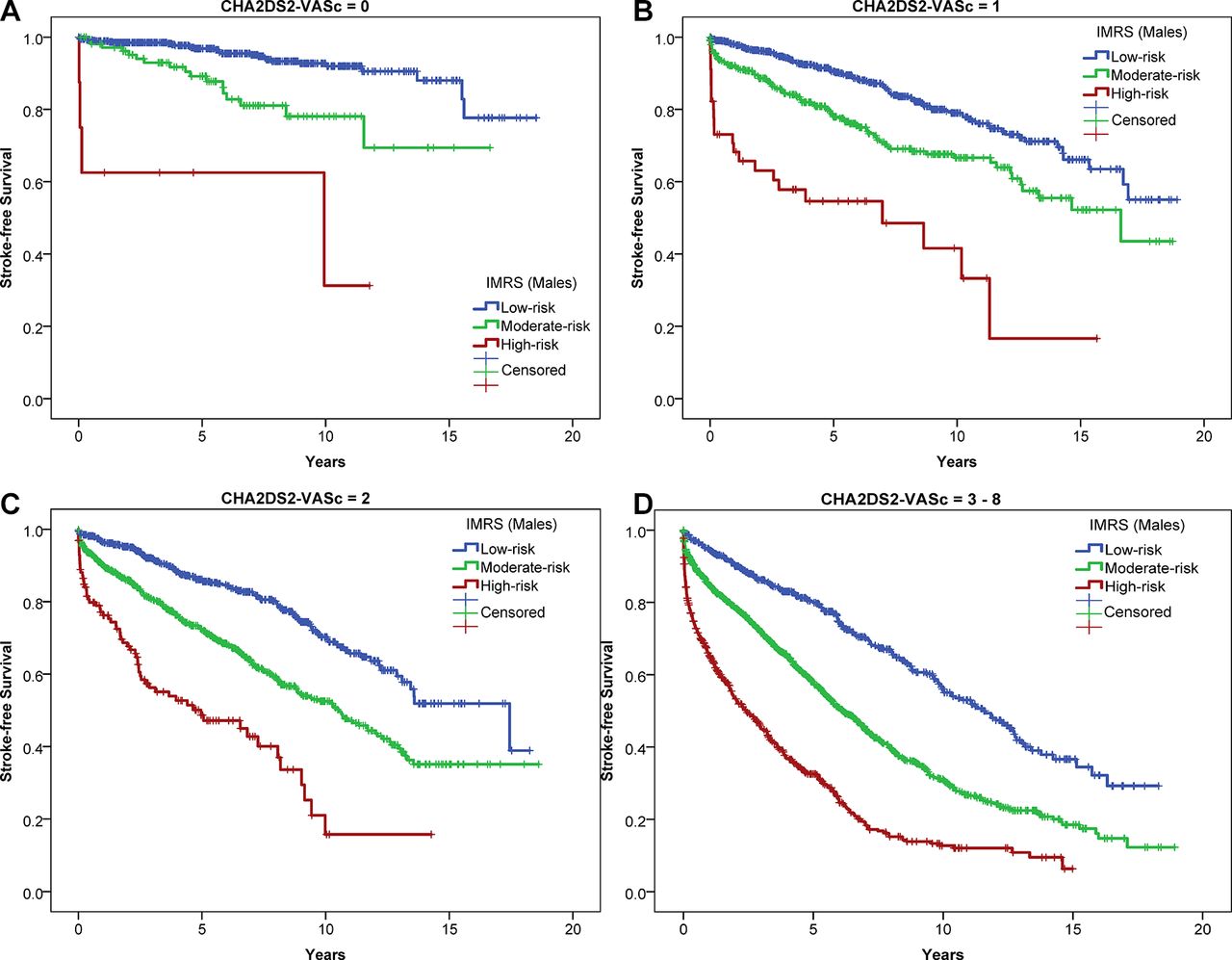
IMRS provided further significant stratification of the risk of stroke/mortality within each CHA2DS2-VASc category, as demonstrated in figure 2 for women and figure 3 for men. This may be especially important in those with CHA2DS2-VASc scores not meeting guidelines for OAC (CHA2DS2-VASc<2) and in those just barely meeting guideline to receive OAC (CHA2DS2-VASc=2). For women with CHA2DS2-VASc=1, IMRS had fully adjusted HR=2.40 (CI 1.21 to 4.79) for moderate risk versus low risk and HR=6.87 (CI 2.03 to 23.21) for high versus low risk, while for those with CHA2DS2-VASc=2 IMRS had HR=1.57 (CI 1.08 to 2.29) for moderate versus low risk and HR=4.03 (CI 2.31 to 7.02) for high versus low risk. In men, those having CHA2DS2-VASc <2 were further risk stratified by IMRS with fully adjusted HR=2.14 (CI 1.65 to 2.77) for moderate versus low risk and HR=6.73 (CI 4.34 to 10.46) for high versus low risk, while among those with CHA2DS2-VASc=2, IMRS had HR=1.87 (CI 1.50 to 2.33) for moderate versus low risk and HR=3.62 (CI 2.65 to 4.96) for high versus low risk. In the CHA2DS2-VASc >2 category, IMRS also provided additional fully adjusted predictive ability among both women (moderate vs low risk: HR 2.00, CI 1.64 to 2.45; high vs low risk: HR 4.28, CI 3.46 to 5.29) and men (moderate vs low risk: HR 1.82, CI 1.56 to 2.14; high vs low-risk: HR 3.60, CI 3.02 to 4.30). For univariable Cox regression using the joint combination of CHA2DS2-VASc and IMRS categories, with all compared with the referent category of <2/low risk, higher HRs in higher risk score categories were found for stroke/mortality, mortality and most analyses for non-fatal stroke (table 3). Small sample sizes, especially in women with CHA2DS2-VASc=1, impacted the non-fatal stroke analyses.

Kaplan-Meier survival curves of the IMRS association with non-fatal stroke/mortality (stroke-free survival) in women with AF, stratified by CHA2DS2-VASc score of (A) 1 (p-trend <0.001, IMRS<9: n=251, 9–14: n=97, ≥15: n=9), (B) 2 (p-trend <0.001, IMRS<9: n=312, 9–14: n=296, ≥15: n=40) and (C) >2 (p-trend <0.001, IMRS<9: n=433, 9–14: n=1736, ≥15: n=948). IMRS, Intermountain Mortality Risk Score.
{kind=link}
{kind=link}
{kind=link}
Kaplan-Meier survival curves of the IMRS association with non-fatal stroke/mortality (stroke-free survival) in men with AF, stratified by CHA2DS2-VASc of (A) 0 (p-trend <0.001, IMRS<11: n=543, 11–16: n=108, ≥17: n=8), (B) 1 (p-trend <0.001, IMRS<11: n=653, 11–16: n=390, ≥17: n=45), (C) 2 (p-trend <0.001, IMRS<11: n=594, 11–16: n=741, ≥17: n=128) and (D) >2 (p-trend <0.001, IMRS<11: n=583, 11–16: n=1553, ≥17: n=609).
HRs and 95% CI (bold/italicised: p<0.05) for the association of joint CHA2DS2-VASc and IMRS categories with non-fatal stroke/mortality, non-fatal stroke and mortality
These stratified findings were replicated within further stratifications defined by whether or not patients were prescribed an OAC at discharge (online supplementary figures s1 and s2). Formal analyses of statistical interactions between OAC and IMRS or CHA2DS2-VASc scores showed no interaction (among women and men, all p-interaction were p>0.10 and up to p=0.86). OACs were associated with stroke/mortality only among women in multivariable models (HR 0.90, CI 0.81 to 0.999, p=0.0496; which arose only from an association with mortality: HR 0.88, CI 0.79 to 0.98, p=0.018), but they were not associated with stroke/mortality or mortality in men and were not associated with non-fatal stroke in either sex.
For non-fatal stroke individually, CHA2DS2-VASc (women—1: 3.9%, 2: 4.6%, >2: 6.6%, p-trend <0.001; men—<2: 3.1%, 2: 3.9%, >2: 5.8%, p-trend <0.001) and IMRS (women—low risk: 6.4%, moderate risk: 6.4%, high risk: 4.9%, p-trend=0.06; men—low risk: 4.1%, moderate risk: 4.6%, high risk: 6.0%, p-trend <0.001) predicted non-fatal stroke. However, for women, the predictive ability was not different from chance (c=0.480), while for IMRS in men (c=0.526) and CHA2DS2-VASc for both sexes (women: c=0.573; men: c=0.596), the predictive ability was minimal. In bivariable Cox regression analyses for non-fatal stroke alone (table 2), CHA2DS2-VASc but not IMRS remained significant among women, while the higher but not intermediate categories of both risk scores were significant predictors among men. Cox regression for joint risk score categories further elucidated the combined associations with non-fatal stroke (table 3).
For mortality alone, CHA2DS2-VASc (women—1: 9.8%, 2: 19.9%, >2: 44.9%, p-trend <0.001; men—<2: 13.5%, 2: 28.2%, >2: 49.9%, p-trend <0.001) and IMRS (women—low risk: 13.7%, moderate risk: 37.8%, high risk: 62.6%, p-trend <0.001; men—low risk: 16.2%, moderate risk: 40.2%, high risk: 64.6%, p-trend <0.001) predicted the outcome. For mortality, table 2 shows that both risk scores were strongly significant predictors in both women and men, with c=0.730 for IMRS and c=0.685 for CHA2DS2-VASc among women and c=0.730 for IMRS and c=0.713 for CHA2DS2-VASc among men. See table 3 for joint risk score associations with mortality.
Discussion
The sex-specific IMRS and the CHA2DS2-VASc score were significant independent risk predictors of a composite of stoke or mortality among patients with AF. The two scores also predicted the individual endpoints, with both predicting non-fatal stroke among men and mortality among men and women. As further evidence of their independent ability to predict risk, IMRS added to risk stratification when examined within substrata defined by CHA2DS2-VASc levels. These findings add patients with AF to the populations for which IMRS is a validated predictor of risk.4 7 8 With respect to the clinical application of IMRS, patients with AF with a CHA2DS2-VASc score at or above 2 had significant additional discrimination of risk across IMRS categories that could be useful in evaluation of which patients with AF require OAC. This included that some patients with a CHA2DS2-VASc score <2 were identified to have a significantly higher risk when IMRS was included in risk stratification (see figures 2A, 3A and B) than clinically is estimated today by use of just CHA2DS2-VASc. Among patients where CHA2DS2-VASc suggests that OAC is indicated, IMRS identified patients with AF who were at a substantially lower risk than the CHA2DS2-VASc estimate indicated, including in those with a CHA2DS2-VASc score of 2.
IMRS is a validated risk prediction tool that has the ability to provide discrete information regarding pathological and metabolic pathways.12 This prediction tool uses components of the CBC and BMP, and has illuminated the broader risk implications that are present within these commonly ordered tests. Originally created to predict mortality in a general population, IMRS reflects underlying pathophysiology that presents itself in patients as a constellation of factors that result in systemic vascular dysfunction. It is suspected that AF is a manifestation of underlying systemic vascular disease.13 One of the strongest drivers of IMRS is the red cell distribution width, which is associated with many diseases and may serve well as a marker for many underlying pathophysiologies.14 The mechanism behind this relationship is not entirely known, but the red cell distribution width may serve as a strong marker of risk regardless of whether we understand the biology at this time. IMRS also uses essentially all other components of the CBC and BMP, which give a broader view of the underlying metabolic and pathological pathways, although the risk weightings vary in strength for the various score components. For example, platelets, platelet receptors and adhesion molecules all play a critical role in coronary artery disease,15 and white blood cell count is also a well-established marker of general inflammation.
The argument for starting a patient with AF on OAC at a specific CHA2DS2-VASc score threshold is based on recommendations of society guidelines. These recommendations are based on studies that suggest the CHA2DS2-VASc more clearly defines risk than the CHADS2 score and redistributed more patients from a low-risk to a high-risk group.10 16 17 This shift from the CHADS2 to CHA2DS2-VASc score is largely based on removing the large intermediate-risk group found with CHADS2, where anticoagulation recommendations were not very clear.17 The result was a large shift of women, particularly older women, to the high-risk group. Unfortunately, while older women have a heightened risk of stroke, they are also at a higher risk for bleeds. It is also suggested that CHA2DS2-VASc was a better discriminator of ‘true low-risk’ patients when compared with CHADS2.16 This is important as the net benefit analyses have shown only patients who truly do not benefit from OAC are those at low risk for stroke, even when taking bleeding risk into account.18 While CHADS2 and CHA2DS2-VASc are the most widely used measures to determine use of OAC in patients with AF, it is readily apparent that they are challenged by their lack of discernment between low-risk, intermediate-risk and high-risk patients, as well as a lack of dynamicity. While a study showed that CHA2DS2-VASc can increase over time,(29) this only occurs when a risk factor that a patient did not already have is diagnosed, while laboratory factors can increase and also decrease and may improve in response to a successful treatment. By current guidelines, patients with a score >1 should receive OAC. In this cohort, that accounts for 91.1% of women and 70.1% of men (88.6% of men when a score of 1 is included in the high-risk group).
IMRS exhibited stronger specificity as well as stronger NPV than CHA2DS2-VASc in this cohort of patients. The augmentation of risk stratification can be useful to clinicians when dealing with an intermediate-risk patient (as defined by CHA2DS2-VASc). A low IMRS when combined with a CHA2DS2-VASc score of 2 showed a near fourfold lower risk compared with a patient with a high IMRS in the same CHA2DS2-VASc strata. Similarly, lower risk was noted for high versus low IMRS in CHA2DS2-VASc score of 1. Discernment of truly low-risk patients in this ‘intermediate-risk’ group represents an opportunity for low-risk patients to put off initiation of OAC until their risk profile increases to a level more commensurate with OAC initiation. A similar approach may be considered for OAC initiation in a patient stratified as low risk by CHA2DS2-VASc but with a high IMRS.
Limitations
This was a retrospective, observational study that used historically collected data entered by physicians from patients who presented for cardiac catheterisation. Hence, this study may include unobserved or uncontrolled confounding that could limit the generalisability of the results. For example, a minority of these patients with AF presented with acute coronary syndromes which may alter laboratory values transiently, although such changes may be prognostic compared with patients with non-acute coronary syndromes. Furthermore, the patients included in this study were higher-risk individuals with a clinical indication for cardiac catheterisation, thus the results reported herein may not be generalisable to the general AF population. Also, the extent to which adding these risk scores improves predictive accuracy in therapeutic decision-making for this patient cohort requires additional study.
Conclusions
Using IMRS jointly with CHA2DS2-VASc in patients with AF improved the prediction of stroke and mortality. For example, in patients at the OAC treatment threshold (CHA2DS2-VASc=2), IMRS provided ≈4-fold separation between low and high risk. IMRS provides an enhancing marker for risk in patients with AF that reflects the underlying systemic nature of this disease that may be considered in combination with the CHA2DS2-VASc score.
References
Footnotes
BDH and TJB contributed equally.
Contributors BDH and TJB designed the study. KGG, HTM, VJ, BDH and TJB planned the execution of the study. BDH and HTM collected and prepared the data. BDH conducted statistical analyses. KGG, HTM, KUK, JBM, VJ, DLL, JLA, BDH and TJB evaluated and interpreted the results. KGG, VJ, BDH and TJB drafted the manuscript. HTM, KUK, JBM, DLL and JLA revised the paper for important intellectual content.
Funding This work was supported by internal institutional funds and the authors had final authority over manuscript content.
Competing interests BDH is an inventor of IMRS and other risk scores that are licensed to CareCentra. BDH is PI of grants funded by Intermountain Healthcare's Foundry innovation program, the Intermountain Research and Medical Foundation, CareCentra, AstraZeneca and GlaxoSmithKline for the development and/or implementation of clinical risk scores. The authors have no other potential conflicts of interest to report.
Patient consent Not required.
Ethics approval This study was approved by the Intermountain Healthcare Institutional Review Board as a minimum-risk study.
Provenance and peer review Not commissioned; internally peer reviewed.
Data sharing statement No additional data are available.