Article Text

Abstract
Objective Stress testing is commonly performed in emergency department (ED) patients with suspected acute coronary syndrome (ACS). We hypothesised that changes in N-terminal pro-B type natriuretic peptide (NT-proBNP) concentrations from baseline to post-stress testing (stress-delta values) differentiate patients with ischaemic stress tests from controls.
Methods We prospectively enrolled 320 adult patients with suspected ACS in an ED-based observation unit who were undergoing exercise stress echocardiography. We measured plasma NT-proBNP concentrations at baseline and at 2 and 4 hours post-stress and compared stress-delta NT-proBNP between patients with abnormal stress tests versus controls using non-parametric statistics (Wilcoxon test) due to skew. We calculated the diagnostic test characteristics of stress-delta NT-proBNP for myocardial ischaemia on imaging.
Results Among 320 participants, the median age was 51 (IQR 44–59) years, 147 (45.9%) were men, and 122 (38.1%) were African–American. Twenty-six (8.1%) had myocardial ischaemia. Static and stress-deltas NT-proBNP differed at all time points between groups. The median stress-deltas at 2 hours were 10.4 (IQR 6.0–51.7) ng/L vs 1.7 (IQR −0.4 to 8.7) ng/L, and at 4 hours were 14.8 (IQR 5.0–22.3) ng/L vs 1.0 (−2.0 to 10.3) ng/L for patients with ischaemia versus those without. Areas under the receiver operating curves were 0.716 and 0.719 for 2-hour and 4-hour stress-deltas, respectively. After adjusting for baseline NT-proBNP levels, the 4-hour stress-delta NT-proBNP remained significantly different between the groups (p=0.009).
Conclusion Among patients with ischaemic stress tests, static and 4-hour stress-delta NT-proBNP values were significantly higher. Further study is needed to determine if stress-delta NT-proBNP is a useful adjunct to stress testing.
- echocardiography
- emergency medicine
- coronary artery disease
- acute coronary syndrome
- myocardial ischaemia and infarction (IHD)
- biomarkers
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
- echocardiography
- emergency medicine
- coronary artery disease
- acute coronary syndrome
- myocardial ischaemia and infarction (IHD)
- biomarkers
Key questions
What is already known about this subject?
Patients in the emergency department with potential acute coronary syndrome are often admitted to the hospital to receive provocative cardiac stress testing.
In the case of exercise echocardiography testing, imaging is used to identify abnormal wall motion abnormalities after stress.
It is known that N-terminal pro-B type natriuretic peptide (NT-proBNP) is also released with acute ventricular wall stress.
What does this study add?
We examined whether NT-proBNP elevates acutely when patients have an abnormal exercise echocardiography test by comparing the change in plasma levels of NT-proBNP in patients with abnormal stress tests with patients with non-ischaemic stress test results.
We found that stress-delta NT-proBNP had modest areas under the receiver operating curves for predicting ischaemia on stress test imaging.
How might this impact on clinical practice?
If further validated, our work suggests a potential role for stress-delta NT-proBNP for identifying inducible myocardial ischaemia in patients presenting with acute coronary syndrome symptoms.
Introduction
Background
Accurate diagnosis and management of patients with suspected acute coronary syndromes (ACS) has been a vexing problem for decades.1–5 Patients can be rapidly assessed for myocardial infarction (MI) by cardiac troponin assays.6–9 However, even in the era of high-sensitivity troponin assays, patients frequently require inpatient admission or observation for further risk stratification, including stress testing.10–14 However, stress tests require specialty expertise and equipment15 16 that are not routinely available in the emergency department (ED). Multiple factors, including medicolegal risk aversion17 18 and supply-induced demand,19 20 have led to widespread, low-yield use of stress testing.21 A new paradigm is needed for risk stratification of patients with suspected ACS in whom MI has been excluded.
Importance
Prior research suggests that myocardial ischaemia induced by stress testing is associated with dynamic increases (stress-deltas) in N-terminal pro-B type natriuretic peptide (NT-proBNP) concentrations.22–29 These studies only included outpatients with symptoms of stable angina. In this investigation, we test a novel means for assessing ED patients with potential ACS: a biomarker-based stress test. A stress test that uses biomarkers (as opposed to imaging) to assess ischaemia could have several possible benefits for ED patients with ACS symptoms and could improve the current paradigm.
Goals of this investigation
We hypothesised that ED patients undergoing stress testing with myocardial ischaemia would demonstrate higher increases in NT-proBNP (stress-delta NT-proBNP) than patients without myocardial ischaemia. We calculated the diagnostic test characteristics for the index test of stress-delta NT-proBNP compared with a reference standard of standard stress test imaging. For exploratory analyses, we evaluated whether patients who subsequently suffered adverse cardiac events, such as MI, urgent percutaneous coronary intervention (PCI) or coronary artery bypass grafting, would similarly demonstrate significantly higher stress-delta NT-proBNP.
Methods
Study design and setting
We conducted an a priori planned observational cohort substudy of a prospectively collected biorepository compiled at an urban academic medical centre ED with an approximate yearly census of 75 000 visits. All patients provided informed consent prior to participating. We have previously described the methods for this biorepository,30 but we briefly review it here and follow previously suggested reporting guidelines.31
Selection of participants
From November 2012 to September 2014, we recruited patients from our ED-based observation unit daily on weekdays and intermittently on weekends when staffing was available. During this time, we saw an estimated 5000 patients with undifferentiated chest pain per year in our ED and patients are placed in the ED-based observation unit based on treating physician gestalt with some exclusion criteria as previously described.3 32 33 In short, patients cannot be placed in the observation unit (and were therefore excluded from our study) if they have significant arrhythmias, unstable vital signs, aortic aneurysm or dissection, active myocarditis or pericarditis, acute or decompensated heart failure, or severe aortic stenosis. Likewise, patients had to have non-diagnostic results from serial ECGs and three cardiac troponin assays (Roche Elecsys fourth-generation troponin T) over 8 hours below our institutional cut-off (<0.1 ng/mL, 10% coefficient of variation (CV) level ≤0.03 ng/mL). Advanced practice providers provided care in our observation unit, but final decisions about eligibility for the unit rested with the attending emergency physician caring for the patient in the ED. Approximately 65% of patients in our observation unit for ACS have stress echocardiograms as part of their work-up as opposed to other modalities (myocardial perfusion imaging or cardiac MRI).
Eligible patients for the biorepository had the following characteristics: (1) over the age of 30 years, (2) placed in our observation unit for symptoms suggestive of ACS and (3) scheduled to have exercise stress echocardiography as part of usual care.
Interventions
As part of usual care, patients underwent stress echocardiogram that included symptom-limited treadmill exercise using the Bruce Protocol followed by standard echocardiogram. Stress echocardiograms were interpreted by board-certified cardiologists who were blinded to the results of study-specific NT-proBNP results and overall study hypothesis. The reports generated by these usual-care studies were used for our outcome. Two reviewers (including ATL) further reviewed these reports to confirm abnormal studies and to adjudicate indeterminate results. A third reviewer (LKN), a board-certified cardiologist, adjudicated the remaining indeterminate reports. All reviews were conducted blinded to NT-proBNP results.
We obtained serum samples from a peripheral vein before stress testing and 2 hours after stress testing using existing intravenous catheters when possible. Whenever possible, we obtained a 4-hour post-stress blood sample but did not exclude patients if this sample could not be obtained.
We centrifuged blood within 1 hour of collection for plasma, which was aliquoted into 0.4 mL samples and frozen at −80°C within 8 hours of collection. A core laboratory at the University of Maryland determined plasma concentrations of NT-proBNP using an assay from Roche Diagnostics (Indianapolis, Indiana). The limit of detection for this assay is 5.0 ng/L, the 97.5th percentile cut-off has been established as 115 ng/L, and the manufacturer-recommended cut-off for clinical use is 125 ng/L. At a level of 125 ng/L, the CV for the system is 2.7%. We blinded the core laboratory to all clinical data, including the outcomes of stress testing and subsequent cardiac events. Likewise, all clinical staff caring for patients were blinded to the research NT-proBNP results.
Measurements
In our repository, we collected demographics, patient history including cardiac risk factors and comorbidities, and usual care laboratory and radiography testing results. Clinical data were collected from patients via standardised data collection form and confirmed with medical providers. We prospectively contacted participants at 90 days from enrolment to ascertain the occurrence of any adverse events. We also recorded the results of any relevant tests and other events occurring during the patient’s index visit and for 1 year afterwards via medical records review. We specifically recorded the occurrence of any subsequent MI (International Classification of Diseases-9 code or medical record evidence), abnormal stress testing, significant coronary disease by angiography (lesions >50% in a major epicardial coronary artery), PCI or coronary artery bypass graft surgery (CABG), or death (cardiovascular and all-cause) within 90 days and 1 year from enrolment. At enrolment, we obtained consent to review outside hospital records to confirm any events that occurred outside of our health system. Any discrepancies or ambiguity of follow-up outcome were adjudicated by the lead author. We entered study data into a REDCap (Research Electronic Data Capture)34 data repository hosted at Duke University.
Outcomes
For this a priori planned substudy of the parent biorepository, we compared stress-delta NT-proBNP concentrations between patients with inducible myocardial ischaemia (wall motion abnormality in at least one segment with stress that was not present at rest) on their stress tests versus those without. We calculated the diagnostic test characteristics—sensitivity, specificity and area under the receiver operating curve (AUC)—for the index test of 2-hour and 4-hour stress-delta NT-proBNP values compared with a reference standard of stress echocardiography imaging results.
In an exploratory analysis, we also compared stress-delta NT-proBNP results between patients who had a composite adverse cardiac event outcome at 90 days from index visit and those who did not. We included any patient who had any revascularisation procedure (PCI or CABG), MI or death within 90 days of the index visit. We also extended the follow-up period to 1 year.
To assess the sensitivity of stress-delta NT-proBNP for myocardial ischaemia on stress testing, our targeted sample size of 333 patients would provide a 95% CI range of approximately ±15%, assuming a true sensitivity of 85%.35 For 85% power to detect a difference between groups with alpha <0.05, we needed 25 patients with myocardial ischaemia. Based on prior studies in this observation unit, we anticipated being able to find at least an 8% prevalence of ischaemia on stress tests being performed in our unit.32
Analysis
Absolute and relative intraindividual changes in NT-proBNP concentrations across time points (stress-delta values) were calculated for each patient. In order to calculate these values, we used a value of 0 ng/L for any NT-proBNP assay that was below the limit of detection for this assay (5 ng/L). We used the Wilcoxon rank-sum test to compare the distribution of individual stress-delta values between patients with ischaemia on stress testing versus those without. Additionally, 2-hour and 4-hour stress-delta NT-proBNP values were analysed using analysis of variance models to adjust for differences in baseline values between groups; in these models, all NT-proBNP values were log-transformed due to skew. The receiver operating characteristic (ROC) curves were plotted and the AUC calculated, with calculation of optimal cut-off for maximal sensitivity and specificity. We did not adjust for multiple comparisons. A two-sided p value of <0.05 was considered statistically significant. All analyses were conducted using SAS V.9.4 statistical software.
Results
Characteristics of study subjects
We approached 413 eligible patients and ultimately enrolled 320 patients. Patients who were approached but did not enrol fell into one of the following non-exclusive categories: 30 patients declined or otherwise could not provide informed consent, 43 patients were unable to provide adequate blood samples or accurate lab assays, and 35 patients had their stress test changed to a non-exercise modality after consent. Four-hour post-stress samples were available for 173 patients.
Table 1 shows the demographic and clinical characteristics of enrolled patients. The prevalence of known coronary artery disease and of coronary artery disease risk factors was low.
Patient demographics and clinical characteristics
For the primary comparison, we further excluded two patients who had indeterminate stress test results in the opinion of our three reviewers’ adjudication. Our review of stress test reports resulted in only one disagreement between two reviewers out of 292 stress test reports reviewed—a case initially reported as ischaemia that the second reviewer found to be artefact. In total, 26 patients had myocardial ischaemia on stress echocardiographic testing. In follow-up, we were able to contact 241 (75.3%) by phone at 90 days and conduct medical record review on all patients at 1 year. Within 1 year, 48 patients had had some form of coronary artery imaging, with 16 patients demonstrating at least one artery with >50% stenosis. Ultimately, nine patients had any composite outcome within 90 days and 11 patients had any within 1 year. Each individual patient’s downstream outcomes are shown in online supplementary table 1.
Supplemental material
Main results
Table 2 shows the median (25th and 75th percentiles) NT-proBNP concentrations at each time point, along with the median patient-level absolute and relative changes in NT-proBNP concentrations (stress-delta). The median absolute stress-deltas at 2 hours were 10.4 (IQR 6.0–51.7) vs 1.7 (IQR −0.4 to 8.7) ng/L and at 4 hours were 14.8 (IQR 5.0–22.3) ng/L vs 1.0 (−2.0 to 10.3) ng/L for patients with ischaemia on stress testing versus those without. Patients with abnormal stress tests had significantly higher NT-proBNP concentrations at baseline and at all subsequent time points (all p<0.05). Figures 1 and 2 show spaghetti plots with boxplots of NT-proBNP concentrations at baseline and at 2-hour and 4-hour post-stress comparing patients who had ischaemia on stress testing versus those without.
Patients with ischaemic cardiac stress tests had higher NT-proBNP levels at all time points, as well as higher absolute and relative stress-delta values
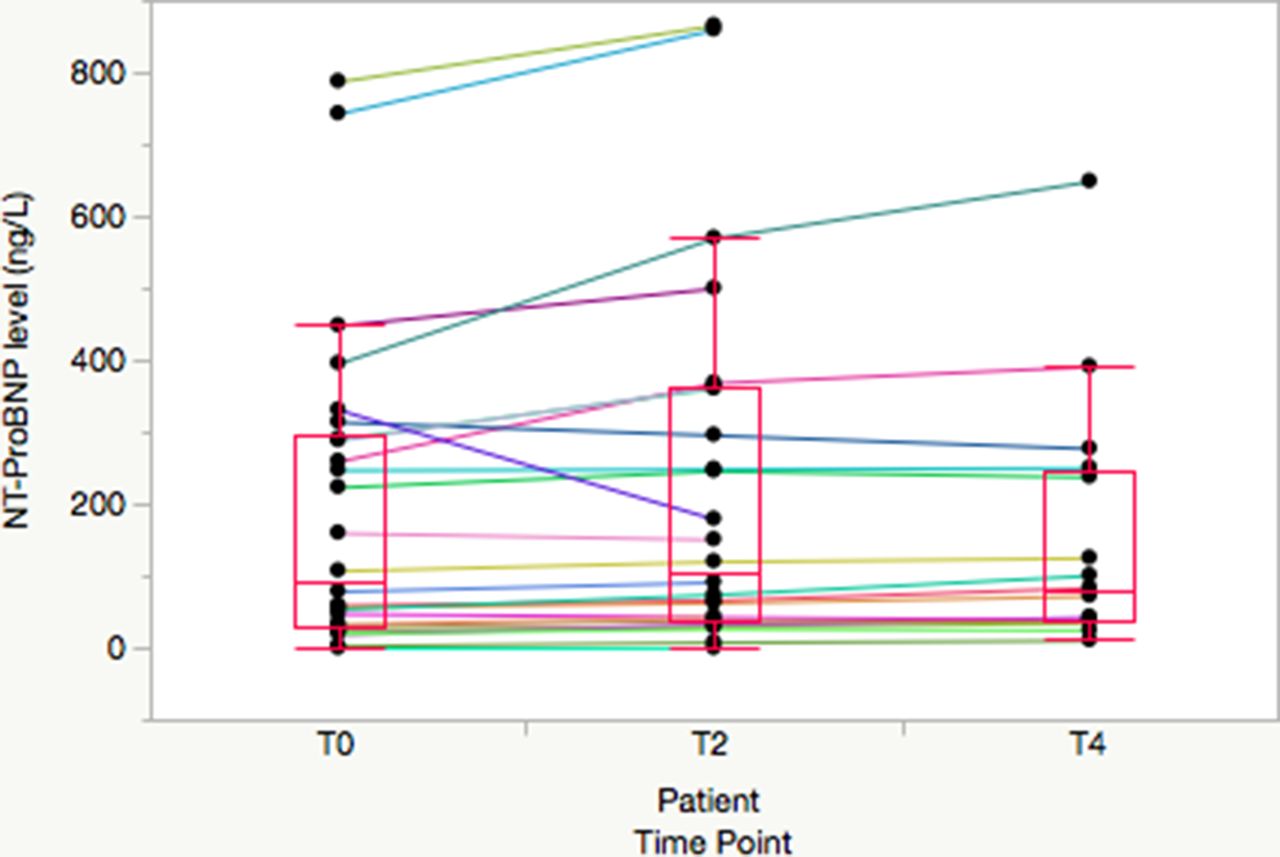
Spaghetti plot of individual patient N-terminal pro-B type natriuretic peptide (NT-proBNP) concentrations for patients with ischaemic stress test results. Median, 25th and 75th percentiles are noted by boxes and whiskers extend to 1.5x interquartile range..

Spaghetti plot of individual patient N-terminal pro-B type natriuretic peptide (NT-proBNP) concentrations for patients with normal or indeterminate stress test results. Median, 25th and 75th percentiles are noted by boxes and whiskers extend to 1.5x interquartile range. . Scale is truncated in order to match figure 1 and due to two extreme outlier patients who are excluded from the graph but not from our analysis.
In unadjusted analyses, relative and absolute stress-delta NT-proBNP significantly differed according to the presence or absence of ischaemia on stress testing at both 2-hour and 4-hour time points. After log transformation of NT-proBNP values and adjusting for baseline concentrations, 2-hour stress-delta NT-proBNP concentrations were not significantly different between patients with ischaemic versus normal stress tests (p=0.07), but the 4-hour stress-delta NT-proBNP concentrations were significantly different (p=0.0085).
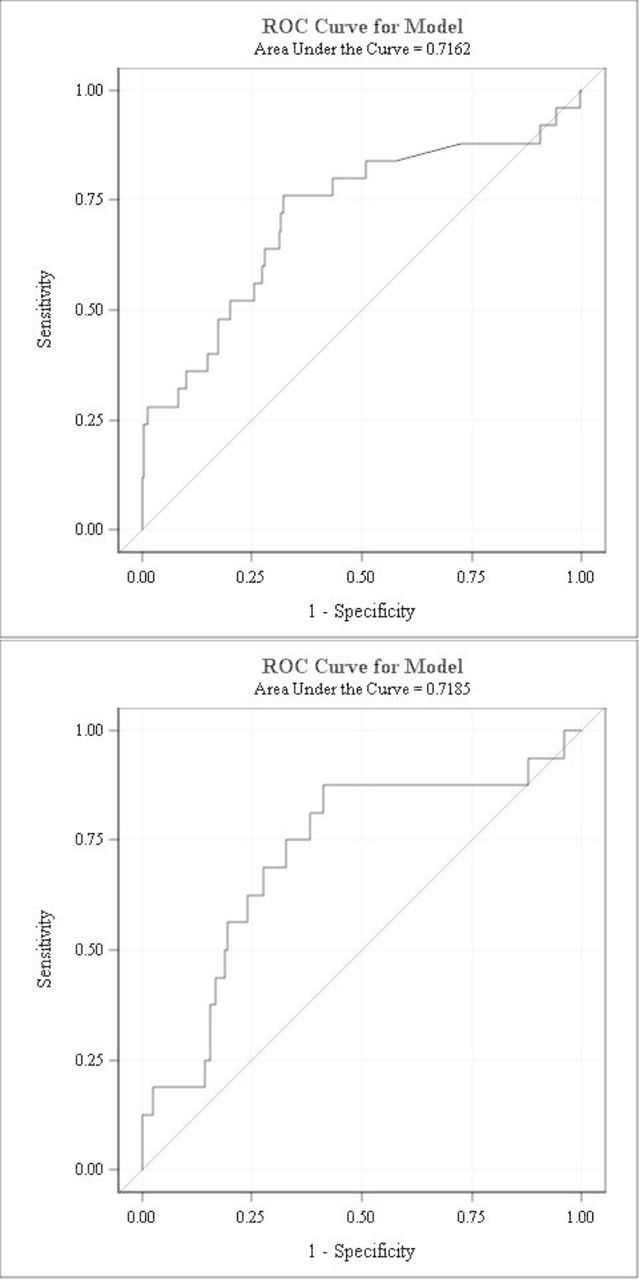
Figure 3 shows the ROC curves of 2-hour and 4-hour stress-delta NT-proBNP for predicting myocardial ischaemia on stress testing. It demonstrates that 2-hour and 4-hour stress-delta NT-proBNP had modest predictive value of ischaemia with an AUC of 0.716 and 0.719, respectively. The diagnostic test characteristics of 2-hour and 4-hour stress-delta NT-proBNP for predicting myocardial ischaemia on stress test imaging are shown in table 3. Stress-delta NT-proBNP has modest sensitivity and specificity, high negative predictive value but poor positive predictive value.
Diagnostic test characteristics of stress-delta NT-proBNP for myocardial ischaemia on stress echocardiogram imaging

{kind=link}
{kind=link}
{kind=link}
ROC curve of 2-hour (A) and 4-hour (B) stress-delta NT-proBNP. Two-hour stress-delta NT-proBNP shows modest predictive ability of ischaemia on stress test imaging with an AUC of 0.7162. Four-hour stress-delta shows an AUC of 0.7185. AUC, area under the curve; NT-proBNP, N-terminal pro-B type natriuretic peptide; ROC, receiver operating characteristic.
In exploratory analyses we found nine patients with a 90-day composite outcome, and the median NT-proBNP values were non-significantly higher at all static time points, and only the absolute 2-hour stress-delta comparison was significantly different (online supplementary table 2). Similarly, none of the NT-proBNP concentrations were significantly different for the 11 patients with a 1-year composite outcome compared with those without such outcome (online supplementary table 3).
Supplemental material
Supplemental material
Discussion
The optimal assessment of suspected ACS remains controversial despite decades of research. The current standard of care uses stress testing,8 36–38 in which the patient who has ruled out for MI undergoes a protocolised stressor and is assessed via imaging modalities such as echocardiography. The current paradigm remains inefficient, and many question the utility of routine stress testing in ED patients with symptoms of ACS.21 39–42 Based on the event rate in the reported literature (eg, <1% in Sandhu et al 42), it appears that stress testing is currently overused. However, there remains concern for adverse cardiac outcomes following serial cardiac troponin testing, even with high-sensitivity assays.7 30
In this context, we sought to determine whether a biomarker-based stress test could improve the current paradigm. Currently, biomarkers are only serially measured in resting patients as a test for MI, heart failure or as a predictor of cardiac complications following major non-cardiac surgery.43 44 Measuring dynamic changes in biomarker levels during stress testing is a novel application of cardiac biomarkers in ED patients. If a biomarker-based stress test could be developed, it would have several advantages. Since laboratory testing is routinely available 24 hours a day to ED patients, a biomarker stress test could serve as a triage test in the ED to determine which patients need further work-up. If it could provide equivalent predictive value, it might represent a cost-effective and time-effective alternative to standard stress testing that does not require special equipment nor specialists to obtain or interpret the images. Based on prior literature,45 46 it would appear that using two serial NT-proBNP tests compared with an echocardiogram would be approximately 30% the cost of using echocardiography with stress testing. However, for biomarkers to replace the use of stress echocardiography, considerably higher sensitivities than our current results would likely be needed. Alternatively, it could be used as an adjunct to aid in disposition of patients with indeterminate results on standard stress tests.
In this study, we assessed the feasibility of a biomarker-based stress test using NT-proBNP. We found that NT-proBNP concentrations differed significantly according to patients’ stress test imaging results. Our study is one of the largest to examine this biomarker-based stress test concept with NT-proBNP. Prior authors found that patients with ischaemia had a differential stress-delta response,22 25–29 while others did not.23 24 Our patient sample of recently symptomatic ED patients makes our study unique. Obtaining a baseline measurement of NT-proBNP just prior to stress testing limits any potential impact that the patients’ recent symptoms may have had on results.
NT-proBNP is the prohormone of BNP released first in the bloodstream and has a shorter half-life, which could potentially lead to differences in results between these two markers. However, others have studied BNP in this paradigm and found a similar range of response in patients with inducible ischaemia.47–54
Prior studies used the stress test imaging component as their gold standard for outcome. We built on these by considering a broader range of downstream outcomes, although these occurred infrequently in our population. Our study did not find significantly different stress-delta results in this comparison, a finding that we attribute to underpowered analyses.
We also found that baseline NT-proBNP levels were significantly higher among patients who ultimately had myocardial ischaemia. This was not our primary intent in this study so these findings should be considered preliminary. However, NT-proBNP has long been noted to have high independent prognostic capability as a traditional ACS biomarker.55–57 Although professional society guidelines acknowledge their potential use for ED risk stratification of ACS,58 they have not entered into common use for this purpose. These findings suggest a potential role for NT-proBNP in ED ACS risk stratification that should be further explored.
Study limitations
Our study has some important limitations. It was performed at a single institution and in a population that had been selected for relatively low risk for ACS. During this time, our unit did not have objective criteria for entry in the ACS pathway. However, it has been shown that clinician gestalt can effectively risk-stratify patients to lower risk groups,59 and our unit’s prevalence of ischaemia is similar to that described in other settings.60 Furthermore, during the time of this study, high-sensitivity troponin assays were not available in our setting. The introduction of these assays will likely alter the prevalence of disease in the population being referred for observation unit care in the future. Although we attempted to approach consecutive patients, we did not have the ability to reach all patients on weekends.
This was an observational study that is subject to ascertainment bias of downstream outcomes, although all patients had the reference standard test as an inclusion criterion. Furthermore, a small sample size with a low event rate led to underpowered analyses of downstream composite outcomes. We did not control for multiple other baseline risk factors other than NT-proBNP to avoid overfitting our small number of patients with ischaemia. We did use an admittedly surrogate outcome for patient-oriented adverse events; however, we felt that for this low-risk cohort, the stress test result is the key data point that determines further testing and thus a valid outcome. In the future, cardiac MRI or angiography could be considered as diagnostic standard, but this would require significant resources to conduct in a study and has less practical relevance for most ED practices. Nonetheless, our findings warrant further study in larger samples with higher risk of ACS. Although we conducted multiple comparisons between groups, the consistency of results at multiple time points and between static and stress-delta comparisons is compelling.
We were not able to obtain 4-hour post-stress samples on all patients in our biorepository. In almost all cases, this was because the patient had been discharged from the ED within 4 hours of completion of their stress test. Despite the smaller sample size for this comparison, we still noted results that were directionally the same as our 2-hour analyses and that were statistically significant in our adjusted analyses. It remains to be seen whether our proposed paradigm of biomarker-based stress testing would be clinically acceptable to clinicians and patients. Furthermore, a complete financial analysis of a biomarker-based stress test strategy is beyond the scope of this paper.
In conclusion, patients with ischaemia on stress testing demonstrated higher concentrations of NT-proBNP at baseline and all subsequent post-stress time points.
Relative and absolute stress-delta NT-proBNP differed significantly based on stress test imaging results at the 2-hour and 4-hour time points, although when adjusted for baseline NT-proBNP only the 4-hour time point remained significant. These findings warrant further study of this biomarker stress test paradigm in a larger number of patients.
Acknowledgments
We would like to acknowledge Ms Ashley Morgan for proof-reading the manuscript. We would like to acknowledge Roche Diagnostics International for their financial support of this project via an investigator-initiated grant.
References
Footnotes
Twitter alimkakeng
Contributors ATL conceived the study. ATL, LKN and YL designed the analysis. ATL and LKN obtained funding for the project. ATL, EJ, JCL and MG oversaw enrolment, data collection, blood specimen collection and storage. RC oversaw the analysis of blood samples and provided expertise on laboratory-related content. ATL, EJ, YL and JCL managed the data. YL provided the statistical analysis plan and analysed the data. ATL drafted the manuscript, and all authors contributed substantially to its revision. ATL takes responsibility as guarantor for the content of the paper as a whole.
Funding Financial support was not dependent on the results of the study. Roche Diagnostics International provided salary support for investigators and materials for testing samples. The investigators retained control of the data throughout the study and the decision of whether to publish the results. The Duke Office of Clinical Research’s support of this project was made possible by Grant Number 1 UL1 RR024128-01 from the National Center for Research Resources (NCRR), a component of the National Institutes of Health (NIH) and the NIH Roadmap for Medical Research. Its content is solely the responsibility of the authors and does not necessarily represent the official view of the NCRR or the NIH.
Competing interests ATL would like to disclose that he has received research support from Roche Diagnostics, Siemens Healthcare Diagnostics and Abbott Laboratories, all of which are manufacturers of troponin and B-type natriuretic peptide assays. RHC has served as a consultant and member of scientific advisory groups for Roche Diagnostics, Quidel Diagnostics, Beckman Coulter Diagnostics, and Siemens Healthcare Diagnostics. LKN reports receiving consulting honoraria from Roche Diagnostics and Philips Healthcare, which produce products related to the current research, and from AstraZeneca HCF, Metanomics and Medscape. She has received research grants from Bristol-Myers Squibb, GlaxoSmithKline, Google Life Sciences (Verily), NHLBI and the MURDOCK Study.
Patient consent Not required.
Ethics approval The Duke University Medical Center Institutional Review Board approved this protocol.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.