Article Text

Abstract
Background Early experience with transcatheter mitral valve replacement (TMVR) highlighted several investigational challenges related to this novel therapy. Conclusive randomised clinical trials in the field may, therefore, be years ahead. In the interim, contemporary outcomes of isolated surgical bioprosthetic mitral valve replacement (MVR) can be used as a benchmark for the emerging TMVR therapies.
Methods We used the nationwide inpatient sample to examine recent trends and outcomes of surgical bioprosthetic MVR for mitral regurgitation (isolated and combined).
Results 21 007 patients who had bioprosthetic MVR between 2003 and 2014 were included. Of those, 30% had isolated MVR and 70% had concomitant cardiac surgical procedure(s). In patients who underwent isolated bioprothestic MVR, mean age was 68±13, and females were the majority (58.4%). Most of these procedures were performed at teaching institutions (71.3%) and during an elective admission (64%). In-hospital mortality improved during the study period (7.8% in 2003 to 4.7% in 2014, p trend=0.016). Postoperative morbidities were common; permanent pacemaker 11.7%, stroke 2.4%, new dialysis 4.9% and blood transfusion 41.6%. Mean length of stay was 13±12 days, and 27.2% of patients were discharged to an intermediate care of rehabilitation facility. Cost of hospitalisation was $62 443±50 997.
Conclusions Isolated bioprosthetic MVR for mitral regurgitation is performed infrequently but is associated with significant in-hospital morbidity and mortality and cost in contemporary practice. These data are useful as benchmarks for the evolving TMVR therapies.
- mitral regurgitation
- bioprosthetic valve
- surgical mitral valve replacement
- transcatheter mitral valve replacement.
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0
Statistics from Altmetric.com
- mitral regurgitation
- bioprosthetic valve
- surgical mitral valve replacement
- transcatheter mitral valve replacement.
Key questions
What is already known about this subject?
Early experience with transcatheter mitral valve replacement (TMVR) identified certain challenges specific to this field. While conclusive randomised trials in the field are under way, contemporary outcomes of isolated surgical bioprosthetic MVR are lacking and can be used as benchmarks for these emerging TMVR therapies.
What does this study add?
In-hospital mortality of isolated bioprothestic MVR improved overtime (7.8% in 2003 to 4.7% in 2014, p trend=0.016), but surgery remained associated with significant morbidity, lengthy hospitalisations and high cost of care.
How might this impact on clinical practice?
These contemporary outcome data on isolated bioprothestic mitral valve replacement may serve as benchmarks for TMVR.
The steady success of transcatheter aortic valve replacement (TAVR) has inspired an explosion of clinical investigations aiming at a matching success in transcatheter therapies for mitral regurgitation (MR), especially in light of the consistent data showing that MR is undertreated worldwide.1–3 Although surgical treatment of MR has evolved to primarily one of repair, not replacement, early experience with transcatheter mitral repair technologies suggested that a large number of patients might be better suited for transcatheter mitral valve replacement (TMVR) than repair, fueling an increasing interest in TMVR.2 There are currently >30 dedicated TMVR systems in development, but only a handful have reached the early feasibility study (EFS) stages.3
The first reports of TMVR with various transcatheter platforms have raised concerns about the safety of this therapy with an average 30-day mortality rate of 23%.4 Nevertheless, the EFS of TMVR with the Tendyne valve (Abbott, Roseville, Minnesota, USA) has recently reported very promising outcomes with an impressively low 30-day mortality at 3.3%.5 Due to the complexity of mitral valve disease and the wide variability in its management, clinical trials of TMVR are expected to face several challenges.6 In the interim, contemporary data on surgical MVR in patients with MR may serve as a benchmark for further investigations in the expanding TMVR field.3 4 7 We aim to use a nationwide representative sample to assess characteristics and outcomes of patients with MR undergoing isolated bioprosthetic MVR in the USA between 2003 and 2014.
Methods
The Nationwide Inpatient Sample (NIS) was used to derive patient-relevant information between January 2003 and December 2014. The NIS is the largest publicly available all-payer administrative claims-based database and contains information about patient discharges from approximately 1000 non-federal hospitals in 45 states. It contains clinical and resource utilisation information on 5–8 million discharges annually, with safeguards to protect the privacy of individual patients, physicians and hospitals. These data are stratified to represent approximately 20% of US inpatient hospitalisations across different hospital and geographic regions (random sample). National estimates of the entire US hospitalised population were calculated using the Agency for Healthcare Research and Quality sampling and weighting method. The institutional review board approved the study and waived informed consent requirements because the data are derived from a nationwide deidentified database.
We used (International Classification of Diseases-Ninth Revision-Clinical Modification procedure code 35.23) to select patients aged 40 years and older who underwent bioprosthetic MVR during the study period. Patients who underwent redo valve surgery (codes 35.95), those with mitral stenosis (codes 394.0) or infective endocarditis (codes 421, 42.10, 42.11, 42.19, 03642, 09884, 11281, 1154) or had codes for mitral valve repair or mechanical MVR during the same admission were excluded (figure 1). The outcomes of patients who underwent isolated valve replacement were then studied and compared with those of patients submitted for valve replacement combined with other cardiac surgery.

Study flow chart.
The trends of bioprosthetic MVR for MV during the 12-year study period were assessed using weighted numbers (national estimates). Baseline patients’ comorbidities and procedural characteristics were described for both the isolated and combined MVR groups. Trends of in-hospital mortality during the study period for both groups were described. Trend weights accounting for changes in the NIS sampling design are only available for data between 1998 and 2011. For 2012 and 2014, trend weights were not available, and the standard survey weights were used. To estimate the cost of hospitalisation, the NIS data were merged with cost-to-charge ratios available from the Healthcare Cost and Utilization Project. We estimated the cost of each inpatient stay by multiplying the total hospital charge with cost-to-charge ratios. Postoperative morbidities, length of stay (LOS), disposition patterns and cost of care were also evaluated. Patient-relevant descriptive statistics are presented as frequencies with percentages for categorical variables and as means with SD for continuous variables. Baseline characteristics were compared between the groups using a Pearson χ2 test for categorical variables and an independent-samples t-test for continuous variables. Trends over time were examined using a Mann-Kendall test for trend (a non-parametric test to determine the presence and direction of a trend over time). All statistical analyses were performed using SPSS V.24 (IBM).
We also sought to identify independent predictors of in-hospital mortality in our study cohort. Hence, we entered 22 clinical, procedural and hospital characteristics into univariate and multivariate logistic regression models to assess their possible predictive value of in-hospital mortality after valve surgery (online supplementary e-table 1,2).
Supplemental material
Results
Between 2003 and 2014, 21 007 patients who underwent bioprosthetic MVR for MR (representing a national estimate of 103 709 patients), were included in our study. Of those, 14 727 (70.1%) underwent a concomitant cardiac surgical procedure. Utilisation of MVR for MR did not change significantly during the study period (figure 2). Patients who underwent a combined cardiac surgery were older (71±10 vs 68±13 years, p<0.001), had higher incidences of diabetes, atrial fibrillation, coronary and peripheral vascular disease, and chronic renal disease than those who underwent isolated MVR. However, history of sternotomy was more common in the isolated MVR group (table 1). Among patients who underwent combined MVR, coronary artery bypass grafting was the most common concomitant procedure (51.3%) followed by aortic valve replacement (31.5%) and Cox-Maze ablation (26.4%). There was a temporal trend towards treating sicker patients overtime evident by the increasing prevalence of key morbidities in both groups during the study period (online supplementary e-tables 1,2).

Utilisation trends of bioprosthetic mitral valve replacement (MVR) for mitral regurgitation in the USA between 2003 and 2014.
Characteristics of patients undergoing surgical bioprosthetic mitral valve replacement (MVR) for mitral regurgitation between 2003 and 2014
Outcomes of isolated MVR
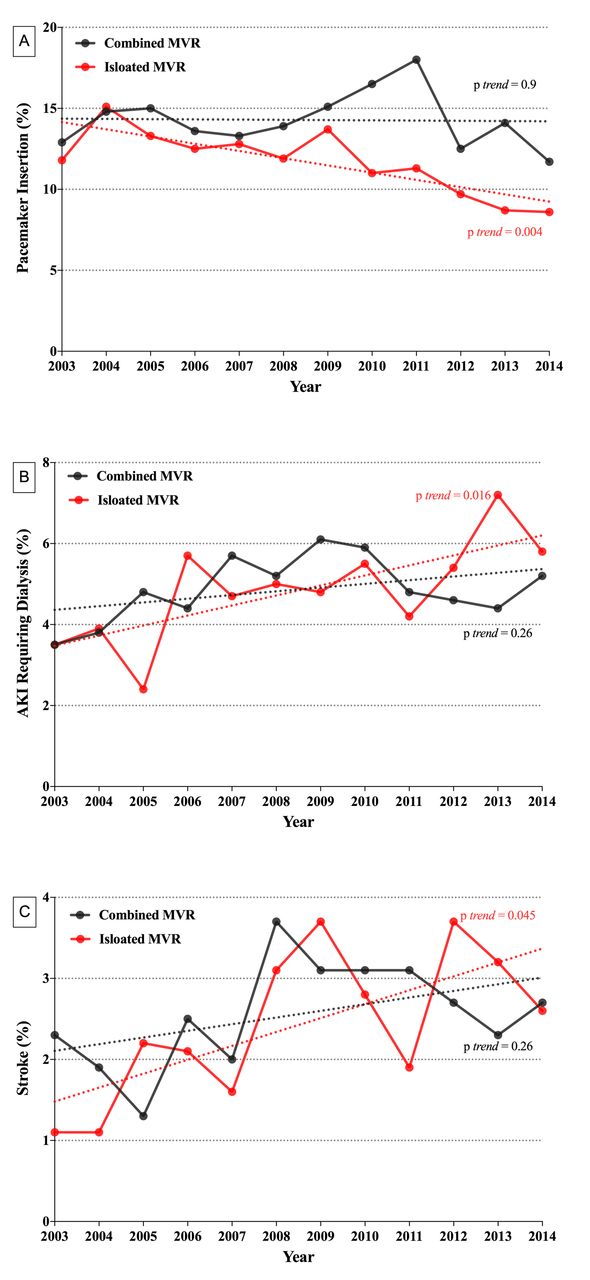
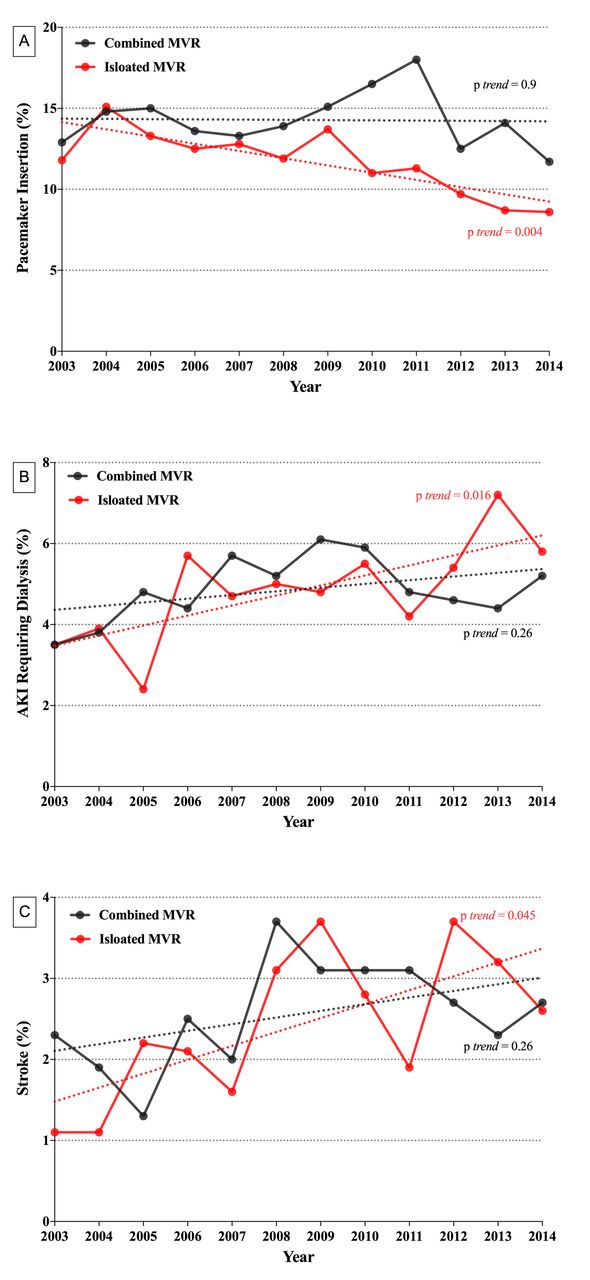
Among patients who underwent isolated MVR, in-hospital mortality was 6.1%, but improved significantly during the study period from 7.8% in 2003 to 4.7% in 2014 (ptrend=0.016) (figure 3). Stroke occurred in 2.4%, vascular complications requiring surgical repair in 1.9% and new dialysis was required in 4.9% (table 2). Also, 11.7% had a permanent pacemaker implantation postoperatively and 41.6% had blood transfusion. There was a temporal trend towards lower incidence of permanent pacemaker implantation, but higher incidences of dialysis-requiring acute kidney injury and stroke during the study period (figure 4). Hospital LOS was >5 days in 84.9% of patients with mean LOS of 13±12 days. Most patients were discharged home versus to intermediate care facility (66.1% vs 27.7%, p<0.001). Mean cost of hospitalisation was $62 443±50 997.

Trend of mortality for patients′ bioprosthetic mitral valve replacement (MVR) for mitral regurgitation between 2003 and 2014.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Trend of complications for patients undergoing bioprosthetic mitral valve replacement (MVR) for mitral regurgitation between 2003 and 2014. (A) Trend of pacemaker implantation isolated versus combined. (B) Trend of acute kidney injury requiring dialysis isolated versus combined. (C) Trend of stroke isolated versus combined.
Clinical outcomes of patients undergoing surgical bioprosthetic mitral valve replacement (MVR) for mitral regurgitation between 2003 and 2014
Outcomes of combined MVR
Among patients who underwent MVR concomitant with other cardiac surgery, in-hospital mortality was 9.4% overall, but also improved during the study period (13.4% in 2003 to 8.3% in 2014, p trend=0.013) (figure 3). In these patients, stroke occurred in 2.6%, vascular complications requiring surgical repair in 2.3% and new dialysis was initiated in 4.9%. Permanent pacemakers were implanted in 14.3% postoperatively. There was no statistically significant change in the rates of major postoperative morbidities in this cohort (figure 4). Approximately 90% of patients stayed in the hospital over 5 days, with a mean LOS of 15±14 days. Intermediate care facilities were used in 35.4%. Mean cost of hospitalisation was $75 469±57 052.
Predictors of in-hospital mortality
Multivariate logistic regression analyses were performed to identify predictors of in-hospital mortality in both groups. Variables included in the regression model included demographic and clinical characteristics, hospital attributes and insurance status. Among patients who underwent isolated MVR, the strongest predictors of in-hospital mortality were the need for ventricular assist device (OR 6.05, 95% CI 4.66 to 7.84), chronic renal failure (OR 2.42, 95% CI 1.88 to 3.12), liver disease (OR 2.27, 95% CI 1.15 to 4.47) and female gender (OR 1.65, 95% CI 1.31 to 2.08). Other predictors are shown in online supplementary e-table 1. Among patients who underwent MVR concomitant with other cardiac surgery, the strongest predictors of in-hospital mortality were the need for ventricular assist device (OR 5.31, 95% CI 4.62 to 6.09), liver disease (OR 3.02, 95% CI 2.14 to 4.25), concomitant tricuspid valve replacement (OR 2.01, 95% CI 1.39 to 2.92) and chronic renal failure (OR 1.83, 95% CI 1.58 to 2.13). Other significant predictors are shown in online supplementary e-tables 3,4.
The impact of gender on in-hospital outcomes
Females constituted the majority of patients undergoing MVR in this study, especially in the isolated MVR group. Compared with males, females who underwent MVR were less likely to be of white race and less likely to have chronic renal disease, coronary artery disease and prior sternotomy, but had higher prevalence of chronic obstructive lung disease and anaemia (online supplementary e-table 5. In-hospital mortality was higher in females than in males following isolated and combined MVR (6.9% vs 5.0%, p=0.001, and 9.9% vs 8.8%, p=0.022, respectively). Females had higher incidences of acute kidney injury and blood transfusion, but similar rates of postoperative strokes and permanent pacemaker implantation (online supplementary e-table 6). Females also experienced longer length of stay, were more likely to be discharged to an intermediate care facility and accrued higher cost of the hospitalisation. In a multivariate logistical regression analysis adjusting for 22 demographic, clinical and hospital characteristics, female gender remained a significant independent predictor of in-hospital mortality (OR 1.65, 95% CI 1.31 to 2.08 for isolated MVR, and OR 1.31, 95% CI 1.15 to 1.48 for combined MVR) (online supplementary e-tables 1,2).
Discussion
The main findings of the present study are (1) MVR for MR remains uncommon and is performed in conjunction with other cardiac surgery procedure in the majority of cases. (2) Patients who undergo MVR for MR have high prevalence of significant clinical morbidities, and this prevalence increased overtime (3) In-hospital mortality following MVR for MR is high but has improved between 2003–2014. However, major post-operative morbidities remained frequent and did not significantly change overtime in the combined MVR group, while the rates of stroke and acute kidney injury increased overtime in the isolated MVR group. (4) MVR for MR is associated with long hospitalizations, frequent intermediate care facility utilisation and significant cost. (5) In this large cohort of patients undergoing MVR, certain patient’s, hospital and procedural characteristics were predictive of in-hospital mortality.
Surgical treatment of MR remains underused due to the surgical risk in many of MR patients and the lack of solid clinical data supporting mitral valve surgery for certain indications (eg, secondary MR).8 9 Over the past decade, transcatheter mitral valve therapies have emerged as promising alternatives to surgery in selected patients and is hoped to expand treatment options in this undertreated population. The MitraClip device demonstrated safety and efficacy in treating severe MR in strictly selected patients with suitable anatomy, but also highlighted the need for further devices to treat wider ranges of MR pathologies.1 This has further fuelled the interest in TMVR with several systems currently in EFS phases. However, investigational challenges in the TMVR field arose due to the complexity and the variability of MV disease and its treatment options.3 For example, it is unclear whether future randomised trials of TMVR would randomise patients against medical therapy or surgical MVR. Also, enrolling patients who are suitable for MitraClip or surgical repair might be challenging. Therefore, conclusive randomised evidence on TMVR could be several years ahead. Current outcomes of isolated bioprosthetic MVR in patients with MR may therefore serve as a benchmark for future investigations. Nevertheless, the existing literature on MVR includes heterogeneous groups of patients with mechanical MVR, infective endocarditis, mitral stenosis and those who are undergoing redo mitral valve operations.7 10–13 In this study, we attempted to identify a group of patients who are similar to those that may be eligible for TMVR (those who are undergoing isolated bioprosthetic MVR for MR).
Several intriguing observations can be made by analysing the patient’s and procedural characteristics in our study: (1) there was a very modest non-significant increase in the number of bioprosthetic MVRs for MR during the study period, contrary to the sharp increase in surgical treatment of other valvular diseases during the same period. (2) Patients who undergo MVR in the current era have high-risk features including a significant prevalence of comorbid conditions (hypertension, diabetes, anaemia, atrial fibrillation, prior sternotomy, coronary artery disease, coagulopathy and chronic renal insufficiency), and the prevalence of these comorbidities increased overtime, suggesting an increasing trend to treated sicker patients. (3) The majority of patients with MR undergo MVR concomitant with other cardiac surgical procedures, with coronary artery bypass grafting being the most common one. Interestingly, concomitant tricuspid valve repair/replacement was undertaken in <10% of patients although moderate/severe tricuspid regurgitation exists in 25% of patients with MR of any aetiology and >50% of patients with secondary MR.3 14 15
In-hospital death occurred in 6.1% and 9.4% of MR patients undergoing isolated and combined MVR, respectively. Although this study included patients across a wide spectrum of risk profiles, it does suggest that even in ‘all-comers’ MVR for MR is associated with significant in-hospital mortality. This highlights the importance of the evolving TMVR field in addressing the critical need to find less morbid alternatives for MR patients. It also emphasises the contrast between aortic and mitral valve diseases. In a contemporary nationwide analysis of surgical aortic valve replacement, average in-hospital mortality rate in all-comers was 2.5%.16 Rates of postoperative morbidities were also high:~5% of patients had a dialysis requiring acute kidney injury,>10% required permanent pacemaker implantation and >40% had blood transfusion. There was also no temporal improvement in the incidence of acute kidney injury and stroke in the combined MVR group, while the occurrence of these complications increased in the isolated MVR overtime (online supplementary efigure-2). These data might be useful when interpreting the emerging literature of the very early experience with TMVR.
Cost and resource utilisation are becoming increasingly important in the era of healthcare reform. Being the first widely adopted transcatheter valve therapy, TAVR was under special scrutiny due to its added incremental costs, but has been found cost-effective in high-risk and inoperable patients.17–19 Emerging TMVR systems have to be cost-effective to survive an increasingly value-driven healthcare delivery system. Our data suggest that MVR is associated with long hospitalisations, significant cost and high rates of intermediate care facility utilisation. Indeed, cost of MVR in our study was over twofold higher than cost of aortic valve replacement in a contemporary national cost analysis.20 These data suggest that future TMVR system can be very competitive from a cost stand of point. In the largest published EFS on TMVR to date, LOS was 9.7±5.9 days even though the trial enrolled patients who are at high or prohibitive risk for MVR.5
Limitations
Our study has several limitations. The NIS is derived from hospital claims data without access to individual medical records and subject to the shortcomings of administrative datasets. However, the Healthcare Cost and Utilization Project (HCUP) quality control measures should minimise these possibilities. Aetiology of MR (primary vs secondary), Society of Thoracic Surgeons (STS) risk score, left ventricular ejection fraction, type of bioprosthetic valve used, baseline and postoperative echocardiographic data are not captured in NIS. Also, details on specific long-term outcomes beyond hospital discharge are also not available in NIS. Finally, this study included patients who were likely deemed acceptable surgical candidates, which may underestimate the actual morbidity and mortality of the higher-risk patients who are currently being denied MVR. Nevertheless, this study provides the largest ‘real-world’ outcome data on bioprosthetic MVR for MR, offering important insights into a cohort of patients that will be the focus of multiple investigations in the field of TMVR.
Conclusions
Despite temporal improvement in operative mortality, isolated bioprosthetic MVR for mitral regurgitation remains associated with high morbidity and mortality and cost in contemporary practice. These data are useful as benchmarks for the emerging TMVR therapies.
References
Footnotes
Contributors CB and FA designed the study, and played a lead role in synthesising the data and editing the manuscript. ZC and SA wrote the first draft and made the illustrations. VB assisted in manuscript drafting and in making critical revisions of the content. FA performed the statistical analyses. MA is responsible for the overall content and the integrity of the data as guarantor.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Not required.
Ethics approval Institutional board approved the study.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement The data will be available for researcher wanting to reproduce the study's result and can be obtained by contacting the corresponding author.