Article Text

Abstract
Objective Mortality amongst patients hospitalised for heart failure (HHF) in Western and Asian countries may differ, but this has not been investigated using individual patient-level data (IPLD). We sought to remedy this through rigorous statistical analysis of HHF registries and variable selection from a systematic literature review.
Methods and results IPLD from registries of HHF in Japan (n=3781) and the UK (n=894) were obtained. A systematic literature review identified 23 models for predicting outcome of HHF. Five variables appearing in 10 or more reports were strongly related to prognosis (systolic blood pressure, serum sodium concentration, age, blood urea nitrogen and creatinine). To compare mortality in the UK and Japan, variables were imputed in a propensity model using inverse probability of treatment weighting (IPTW) and IPTW with logistic regression (doubly robust IPTW). Overall, patients in the UK were sicker and in-patient and post-discharge mortalities were greater, suggesting that the threshold for hospital admission was higher. Covariate-adjusted in-hospital mortality was similar in the UK and Japan (IPTW OR: 1.14, 95% CI 0.70 to 1.86), but 180-day postdischarge mortality was substantially higher in the UK (doubly robust IPTW OR: 2.33, 95% CI 1.58 to 3.43).
Conclusions Despite robust methods to adjust for differences in patient characteristics and disease severity, HHF patients in the UK have roughly twice the mortality at 180 days compared with those in Japan. Similar analyses should be done using other data sets and in other countries to determine the consistency of these findings and identify factors that might inform healthcare policy and improve outcomes.
- acute heart failure
- hospitalised
- nortality prediction
- outcome
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key questions
What is already known about this subject?
The outcome of patients hospitalised for heart failure (HHF) is reported to differ markedly among different countries/healthcare systems, despite similarity in international guidelines on management.
However, this has not been investigated using individual patient-level data with rigorous statistical analyses.
What does this study add?
We directly compared patient characteristics and outcomes in the UK and Japan.
HHF patients in the UK have roughly twice the mortality at 180 days compared with those in Japan even after adjustment by inverse probability of treatment weighting (IPTW) and IPTW with logistic regression (doubly robust IPTW) using covariates strongly associated with mortality identified by a systematic literature review of mortality prediction models.
How might this impact on clinical practice?
In HHF patients, explaining the differences in outcome among countries, cultures and health services independent from disease severity might provide insights that could improve care and outcome and inform healthcare policy decisions.
Introduction
Annually, heart failure (HF) accounts for >80 000 admissions in the UK,1 >200 000 in Japan2 3 and >1 million in the USA. Among patients hospitalised for heart failure (HHF), in-hospital mortality is reported to vary from 2.0% to 12.0%1 3–10 and mortality at 1-year postdischarge from 13.3% to 30.5%.1 6 8 11
Differences in mortality estimates for HHF might be due to variations in patient characteristics, severity of HF, comorbidities or medical care. Substantial international differences in health service provision may also exist, including criteria for admission, length of stay, care in the community after discharge and treatment. There will also be cultural differences in both the art of medicine and patient attitudes to medical advice, especially between Western and Asian countries. To date, outcomes for HHF in different healthcare systems have been investigated only using aggregate rather than individual patient-level data (IPLD). Comparing the characteristics and outcomes of HHF managed in different cultures might identify differences in practice that could improve care.
Accordingly, we investigated in-hospital and post-discharge mortality using IPLD from registries of HHF in the UK and Japan, adjusting for differences in key prognostic variables identified from a systematic review of published mortality prediction models (MPMs) and using inverse probability of treatment weighting (IPTW) techniques.
Methods
Overall study design
Our main objective was to compare the mortality of HHF patients in the UK and Japan after adjusting for differences in baseline covariates. This involved three steps: (1) first, a systematic review of published MPMs for HHF, identifying the variables predicting mortality and estimating their respective predictive weights; (2) subsequently, the predictors identified by the review were imputed in a propensity model using IPTW to identify patients with similar attributes in the UK and Japan; and (3) finally, outcomes of interest between the weighted groups, including in-hospital, 30-day, 90-day and 180-day post-discharge mortality, were evaluated.
Systematic review
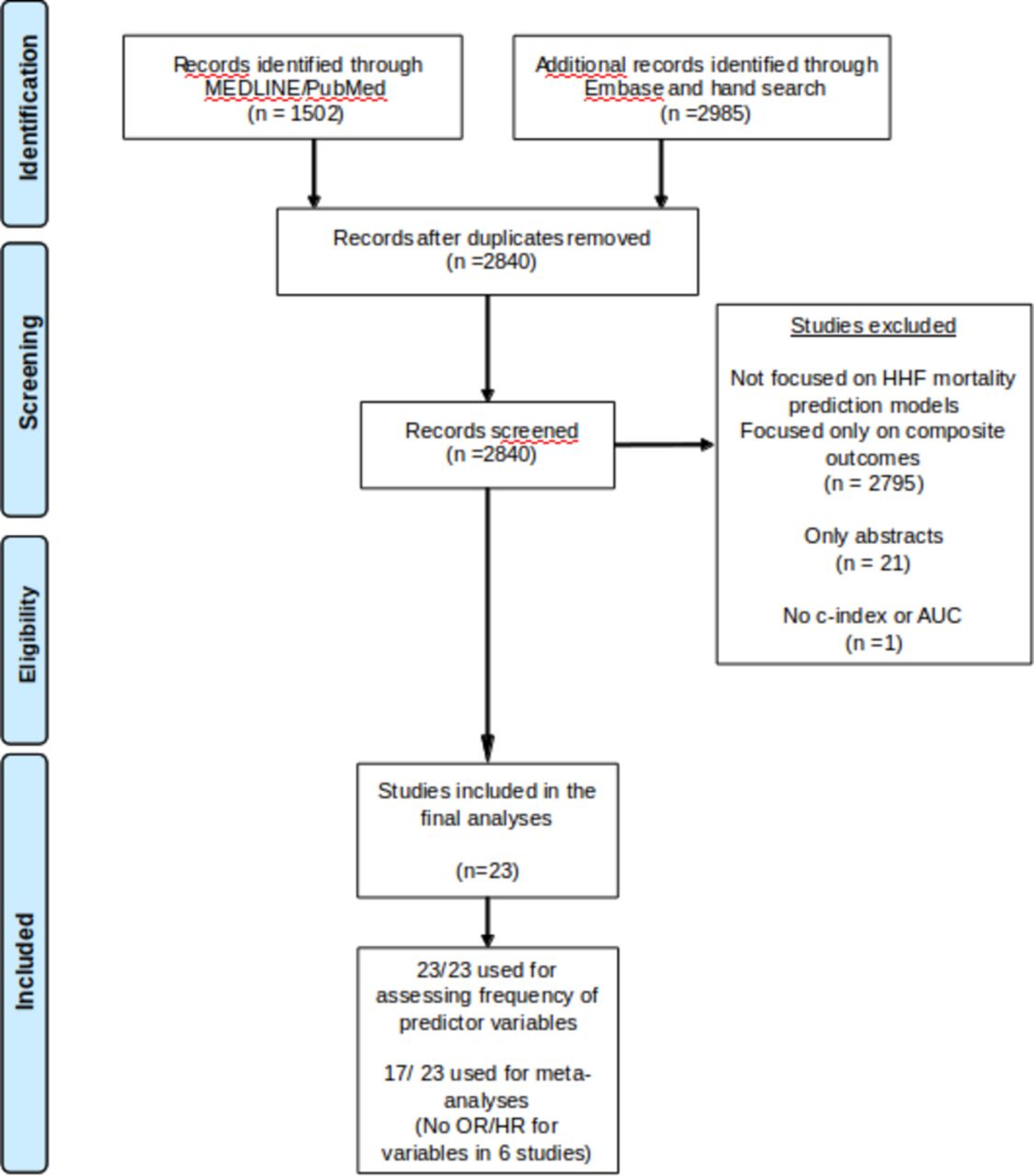
We searched the Medline/PubMed and Embase databases to identify relevant MPMs. We employed search filters that have been validated and shown to have high sensitivity for identification of clinical prediction models in Medline12 (online supplementary appendix) toSupplementary file 1 identify 4487 MPMs for HHF. Those with models only for composite outcomes (ie, HF hospitalisation and mortality), those published only as abstracts and duplicate reports were excluded. We also excluded studies when model performance was not quantified using c-statistics or receiver operating characteristic curves. This identified 23 unique MPMs from which information on individual predictor variables could be extracted. For the meta-analyses, studies lacking OR or HR for predictor variables were excluded; 17 studies were finally included in the meta-analysis (figure 1). All studies were reviewed by two independent cardiologists (TN and VS) to ascertain eligibility (see online supplementary table for details on data extraction and reduction, and statistical analysis).

{kind=link}
Flow diagram of the meta-analyses of published mortality prediction models in HHF patients. AUC, area under the curve; HHF, hospitalised due to heart failure.
Study cohorts
Pooled data from two UK and two Japanese registries of HHF were used. In all registries, HHF was defined by hospitalisation with a diagnosis of HF according to the Framingham criteria.
UK HHF cohort
The Hull and East Yorkshire Hospitals NHS Trust, King’s College Hospital NHS Foundation Trust (London) and Whittington Hospital NHS Trust (London) are three large tertiary care hospitals that each provides emergency care to approximately 500 000 people. All three Trusts participate in the England and Wales National Heart Failure Audit.1 From 2012 to 2013, 697 HHF patients (307 from Hull; 390 from London) were enrolled. Because it is a National Health Service (NHS) registry, neither specific ethical review nor patient consent is required.
The Hull LifeLab is a large, epidemiologically representative, information-rich data set of contemporary diagnosis, treatment and natural history of patients with HF. Its main focus is on out-patient referrals13; only patients hospitalised for HF at the time of enrolment between 2010 and 2011 (n=197) were included in this analysis. The registry has ethical approval and patients gave written informed consent.
Japanese HHF cohort
The WET-HF (WEst Tokyo Heart Failure) registry is an ongoing, prospective observational registry of HHF in five large academic medical centres in metropolitan Tokyo that enrolled 3030 patients between 2005 and 2016.14
The NaDEF (National cerebral and cardiovascular center for acute DEcompensated heart Failure) registry enrolled 751 patients between 2013 and 2015 from a large centre for cardiovascular medicine located in mid-west Japan.15
The study protocols were registered at the Japanese University hospital Medical Information Network (UMIN) Clinical Trial Registration (UMIN000001171 and UMIN000017024, respectively).
Statistical analysis
The weights of variables predicting mortality were meta-analysed, using fixed-effect and random-effect models. The z-scores (OR/SE and HR/SE) of the OR (for case–control studies) and the HR (for cohort studies) of predictor variables were estimated.16 Continuous variables were presented as mean±SD. Baseline variables that were significantly different between the two groups were identified using standardised differences. Among these variables, those that were used in more than one MPM (n≥2) and available in both countries were imputed in an IPTW model to develop balanced groups.17 Balance between the British and Japanese weighted cohorts was evaluated using the standardised differences approach and kernel density plots. For propensity analyses, IPTW was preferred over matching in order to preserve the sample size.18
We performed univariable/multivariable logistic regression analyses, IPTW and IPTW with logistic regression (doubly robust IPTW) to compare odds for mortality (in-hospital, 30-day postdischarge, 90-day postdischarge and 180-day postdischarge) in the UK and Japanese cohorts. Additional analysis was performed for postdischarge mortality after controlling for medicines at discharge. All analyses were performed with Stata MP64 V.15.
Results
Systematic review of MPMs
We identified 28 different MPMs from 23 papers published between 2003 and 2017 (online supplementary table). The five variables with the top z-scores were systolic blood pressure (BP), serum sodium concentration, age, blood urea nitrogen (BUN) and serum creatinine; 26 predictor variables appeared in more than one MPM (table 1).
Frequency of variables used in the models to predict mortality after hospitalisation for heart failure and their respective weights
Cohort baseline characteristics
The baseline characteristics of patients in the UK (n=894) and Japan (n=3781) are shown in table 2. The mean age was similar in UK and Japan, but British patients had more severe HF as evidenced by higher New York Heart Association (NYHA) class, lower systolic BP, lower serum sodium concentrations, higher BUN and serum creatinine concentrations. A higher proportion of Japanese patients had a left ventricular ejection fraction >45%. The prevalence of ischaemic heart disease and chronic pulmonary obstructive disease (COPD)/asthma was higher among British patients compared with their Japanese counterparts.
Baseline characteristics in the unweighted and weighted study population
Inverse probability of treatment weighting
After application of IPTW with variables which were used in two or more MPMs and available in both countries (systolic BP, hyponatraemia, age, serum creatinine, COPD/asthma, heart rate, NYHA class, ischaemic heart disease, stroke, left ventricular ejection fraction, atrial fibrillation, diabetes mellitus and sex), there was good balance between British and Japanese patients’ characteristics. Standardised differences were <0.1 for most variables other than haemoglobin and medications at discharge. After additional weighting for oral medications at discharge (ACE inhibitor/angiotensin II receptor blocker, beta blocker, mineralocorticoid receptor antagonist, diuretics and digitalis), balance (standardised difference <0.1) was achieved for all key variables (table 2).
Mortality before and after IPTW in the UK compared with Japan
Crude analyses showed that mortality was substantially higher in the UK compared with Japan at all time-points (table 3). Unadjusted mortality during hospitalisation was 3.6% in the UK vs 2.2% in Japan, and was, respectively, 3.5% vs 2.7% at 30 days, 9.0% vs 4.4% at 90 days, and 14.7% vs 6.3% at 180 days. Multivariable logistic regression analyses in the unweighted population showed that in-hospital mortality was similar in the UK and Japan, but British patients had a substantially higher mortality by 180 days (table 3). Weighted and doubly robust weighted analyses also showed higher mortality in the UK at 180 days. Because of the low number of events, we did not have the statistical power to perform doubly robust weighted analyses for in-hospital, 30-day (with and without accounting for medications at discharge) and 90-day mortality (after accounting for medications at discharge) (table 3).
Outcomes for British and Japanese HHF patients using multiple adjustment techniques
Discussion
This analysis suggests that HHF patients in the UK have more advanced disease than their Japanese counterparts and a much worse prognosis. After adjusting for differences in patient characteristics using IPTW, in-hospital mortality was similar in the UK and Japan, suggesting that the quality of in-patient care might be similar. However, substantial differences in post-discharge mortality persisted even after adjusting for the prognostic variables that were identified by a systematic literature review and available in both countries. As far as we know, this is the first analysis comparing HHF in Western and Asian countries using IPLD data with doubly robust IPTW. The fact that different methods of adjustment provided similar results suggests that our study has considerable internal validity.
Globally, HHF patients are common, and the numbers are expected to rise as the proportion of older people in the population increases and survival with conditions such as hypertension, ischaemic heart disease and HF itself improves.2 19–21 Internationally, guidelines on the management of HF are rather similar but less is known about the differences among patients from different cultures and countries to whom the guidelines are applied. For example, HHF patients in Japan are reported to have a longer length of hospital stay (Japan: 15–21 days; Europe: 7–9 days; USA: 4 days) and lower in-hospital mortality than patients in Europe and the USA (Japan: 2.0%–5.6%; Europe: 5.5%–6.7%; USA: 3.8%–8.9%).4–7 10 22–24 However, these are crude estimates unadjusted for differences in disease severity. We identified 26 prognostic variables for HHF in a systematic review and used these to adjust for variations in patient characteristics that might have accounted for the differences in mortality. To our knowledge, this is the first systematic review of prognostic variables for HHF; previous systematic reviews focused on chronic HF.16 Despite risk adjustment, 180-day postdischarge mortality remained substantially higher in the UK than in Japan.
Differences in post-discharge mortality could reflect many factors, including genetics, aetiology of disease, post-discharge care, lifestyle, diet, environment or other unmeasured confounders. For instance, in Japan it is customary for patients with HF to be seen in the outpatient clinic within 4 weeks after discharge, even if the HF is not severe, whereas in the UK patients are more likely to be managed in the community by HF specialist nurses and primary care physicians. The Japanese diet will include more rice and less wheat, more salt, more fish, and less red meat.25 The weather is warmer in Tokyo than in England. Japanese patients may be more likely to follow medical advice and adhere to their prescribed medication. On the other hand, Japanese doctors generally prescribe much lower doses of medicines than their British colleagues.26–28 While our analysis estimates the differences in outcomes after adjusting for identified predictor variables, it was not designed to identify the reason for residual disparities.
Limitations
While both the UK and Japan registries had detailed IPLD, certain important variables that were identified from a systematic literature review, such as respiratory rate, serum albumin, troponin and plasma brain natriuretic peptide levels, and medication compliance, were not consistently available. This study is geographically limited to patients hospitalised in Britain and Japan, and our results may not generalise to other Western or Asian countries. Finally, the study was not designed to identify the reason for residual disparities. However, we believe that these limitations are outweighed by methodological strengths, including prospective patient enrolment from multiple centres, a systematic review to identify predictor variables and their estimated weights, and the use of multiple adjustment methods including conventional covariate adjustment, IPTW and doubly robust IPTW, all of which yielded similar results.
Conclusion
HHF patients in the UK have a substantially worse prognosis compared with those hospitalised in Japan. Differences persist after accounting for the greater severity of patients admitted with HF in the UK. Explaining the differences in outcome among countries, cultures and health services might provide insights that could improve care and outcome and inform healthcare policy decisions.
References
Supplementary materials
Footnotes
Funding TN is supported by grants from the Daiichi Sankyo Foundation of Life Science and the Mochida Memorial Foundation for Medical and Pharmaceutical Research. This research was supported by a Butterfield Award for UK–Japan collaboration in Medicine and Health from The Great Britain Sasakawa Foundation.
Competing interests JGFC received grants and honoraria from Amgen, Novartis, Medtronic, Philips, Servier and Stealth BioTherapeutics.
Patient consent Obtained.
Ethics approval The study protocols of both the Japanese registries were approved by the respective institutional review boards.
Provenance and peer review Not commissioned; externally peer reviewed.