Article Text

Abstract
Objective Several studies indicate a prognostic value of sST2 and galectin-3 in heart failure (HF). While previous studies focused on ischaemic cause of HF, we investigated the role of sST2 and galectin-3 in patients with non-ischaemic dilated cardiomyopathy (DCM).
Methods sST2 and galectin-3 serum concentrations were measured in 262 subjects with DCM. Survival rates were determined for all-cause mortality (ACM) and cardiac mortality (CM).
Results In a univariate model, sST2 as a continuous variable was a predictor of ACM (HR 1.05; 95% CI 1.03 to 1.07, P<0.001) and CM (HR 1.03; 95% CI 1.00 to 1.06, P=0.040). In the subgroup of patients with inflammatory and/or viral DCM (DCMi⋎viral), the endpoints ACM (HR 1.10; 95% CI 1.05 to 1.17, P<0.001) and CM (HR 1.10; 95% CI 1.02 to 1.18, P=0.013) were significant. In the subgroup of patients with idiopathic DCM, the endpoint ACM (HR 1.04; 95% CI 1.01 to 1.07, P=0.019) was significant. In a multivariate model, the prognostic value of the sST2 main group remained intact for ACM (HR 1.04; 95% CI 1.02 to 1.07, P=0.003).
Univariate and multivariate analysis of galectin-3 as continuous variable did not show any significant result. However, in a quartile model, intermediate values of galectin-3 were significantly associated with a lower event rate of ACM and CM.
Conclusion The study revealed that sST2 predicts ACM and CM in patients with non-ischaemic HF and could be useful especially in patients with inflammatory background. Our findings that intermediate levels of galectin-3 allow for better prognosis were new and different to other investigations.
Trial registration number NCT03090425; Results.
- sST2
- soluble ST2
- Galectin-3
- Heart failure
- Dilated Cardiomyopathy
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key questions
What is already known about this subject?
A prognostic value of sST2 and galectin-3 in patients with the syndrome heart failure because of coronary artery disease is already known. Both biomarkers were included in the guidelines of the management of heart failure. Whether both biomarkers apply also for patients with cardiomyopathies suffering from an inflammatory origin is a point of discussion.
What does this study adds?
Information with regard to ST2 and galectin-3 as prognostic markers in different disease entities despite coronary artery disease, in this investigation, a population of 117 patients with cardiomyopathy versus 87 patients with inflammatory cardiomyopathy.
How might this impact on clinical practice?
Depending on the pathophysiology of different disease entities clinical useful prognostic relevant biomarkers might differ. It would be helpful to have available specific biomarkers with high prognostic values for specific disease entities as, for example, inflammatory heart disease resulting in severe heart failure.
Introduction
Biomarkers are an easy tool that can help to detect patients at risk of developing adverse events. Established in clinical routine and listed in the guidelines for heart failure (HF) are natriuretic peptides.1 However, these methods are limited because they do not differentiate between various causes of HF and are not independent of non-cardiac factors such as age or renal dysfunction.2
In recent years, many new biomarkers have emerged which indicate prognostic information beyond natriuretic peptides or other cardiovascular risk factors. Among them and already mentioned in the Guideline for the Management of Heart Failure 2013 with a Class of Recommendation IIb are sST2 and galectin-3.3
However, according to the 2016 European Society of Cardiology (ESC) guidelines for the diagnosis and treatment of acute and chronic HF, there is no definite evidence to recommend them for clinical practice.4
Both proteins have been shown to be pathogenetically involved in cardiac remodelling. ST2, a member of the interleukin (IL)-1 receptor family, serves as a ligand for the cytokine IL-33 and exists both as a transmembrane receptor (ST2L) and in soluble form (sST2).5 The synthesis of ST2/IL-33 in cardiac myocytes and fibroblasts is primarily induced by mechanical strain.6 While the interaction between IL-33 and ST2L acts as a cardioprotective mechanism, sST2 functions as decoy receptor and therefore counteracts the beneficial IL-33/ST2L activities.7 Galectin-3 is a beta-galactosidase-binding soluble protein and member of the lectin family.8 Various studies have demonstrated that galectin-3 is upregulated in disease processes of the heart leading to macrophage migration and fibroblast proliferation and therefore to the development of fibrosis.9
In recent years, many studies have shown a prognostic value of sST2 and galectin-3 in HF. However, most of the trials focused on ischaemic aetiology or mixed ischaemic and not on non-ischaemic populations.10–15
Therefore, we investigated patients with dilated cardiomyopathy (DCM), a leading cause of HF, to explore the role of sST2 and galectin-3 in a non-ischaemic population.
We assumed that these biomarkers could be useful especially in the subgroup of patients with inflammatory heart diseases and explored their prognostic implications regarding the specific aetiology of viral and/or inflammatory DCM (DCMi⋎viral) in comparison to familial DCM (fDCM) and idiopathic DCM.
Methods
Study design and participants
This study included 262 subjects with DCM enrolled in the subproject 9a of the German Competence Network Heart Failure between December 2004 and September 2009. Inclusion criteria were age between 18 and 70 years, left ventricular ejection fraction (LVEF) <45% in transthoracic echocardiography and left ventricular end diastolic diameter (LVEDD) ≥117% according to the formula of Henry.
Coronary stenosis >50% verified by coronary angiography, valvular heart disease and arterial hypertension accompanied by end organ damage or hypertension under antihypertensive therapy applied as criteria for exclusion. All patients underwent a careful history and clinical examination as well as laboratory studies and echocardiographic assessment in addition to the investigation of the endomyocardial biopsy. Blood samples were taken from all patients at the time of inclusion. The investigation conforms to the principles outlined in the ‘Declaration of Helsinki’. All participants provided written informed consent.
Analysis of the endomyocardial biopsies included conventional histology, immunohistochemistry and molecular biology for the detection of cardiotropic viruses and was performed as described previously.16 17 Depending on the results, the subjects were classified into different aetiologies. Viral cardiomyopathy was present if cardiotropic viral DNA or RNA was verified in endomyocardial biopsy. The term inflammatory cardiomyopathy was used if quantitative immunohistological (specified either as foci of lymphocytes and/or ≥14 lymphocytes and macrophages/mm2) or conventional histopathological criteria using the Dallas classification were positive.18 Subjects with viral evidence, the presence of inflammation or both were classified as the group DCMi⋎viral.
Patients with positive family history regarding dilated heart disease using the Mestroni criteria were categorised as the group fDCM.19 Subjects without viral or inflammatory evidence and without familial background formed the group idiopathic DCM.
Biomarker measurements sST2 and galectin-3 serum concentrations of all 262 patients were measured using a quantikine ELISA kit (R&D Systems) and blood samples of the containment. The samples were stored at a temperature of at most −20°C. Every specimen was measured twice and the mean values were used.
Follow-up and outcomes
One-year and 5-year clinical follow-up investigations including physical examination, ECG and echocardiography were carried out. At the 1-year follow-up investigation, the status of 17 patients were unknown. By the 5-year follow-up, another 46 patients were lost. Primary endpoints were all-cause mortality (ACM) and cardiac mortality (CM).
Statistical analysis
Statistical analyses were performed using the software R V.3.1.1. The demographic and baseline characteristics are summarised by their mean and SD for continuous variables and counts with percentages for categorical variables. In order to estimate correlations between sST2 and galectin-3 and selected covariables, two-sided univariate linear regression analysis were conducted and the correlation coefficient r and the corresponding P value reported. The association between the biomarkers and ACM and CM was assessed with a univariate Cox-regression model and HR, 95% CIs and P values were given. In the main group, including all 262 patients without taking account of the different aetiologies, univariate survival analyses were performed for ACM and CM with sST2 and galectin-3 as continuous variables and based on Cox-regression, a multivariate model was created for the endpoint ACM to adjust for sex, age, body mass index, diabetes, aetiology, QRS duration, New York Heart Association class, LVEF and LVEDD.
The continuous variables of the sST2 and the galectin-3 main groups with the 262 enclosed subjects were additionally split into ordinal variables according to quartiles with approximately the same size. A univariate Cox-regression model was fitted with the ordinal variables and HRs and P values were reported.
Due to the smaller number of subjects, the subgroups idiopathic DCM (n=117), fDCM (n=58) and DCMi⋎viral (n=87) were analysed only in a univariate model with both biomarkers as continuous variables.
For all statistical evaluations, P values <0.05 were considered significant.
Results
Study population
The mean age of the 262 participants in the study was 50.2±12.8 years. Patients (75.2%) were male. Subdivided according to aetiology, idiopathic DCM was predominant with 117 patients (44.7%). The second largest group was DCMi⋎viral with 87 patients (33.2%). The group of fDCM was the smallest with 58 patients (22.1%). The mean period of observation was 3.9 years with a longest period of 7.6 years. During the follow-up time, occurrence of ACM was 16.4%, among them CM was 12.6%. In the subgroup idiopathic DCM, the event rate for ACM was 14.5% and for CM 12%. In the subgroup fDCM, the event rate for ACM was 19% and for CM 15.5% and in the subgroup DCMi⋎viral, the event rate for ACM was 17.2% and for CM 11.5%. Detailed information regarding demographic and clinical baseline characteristics are presented in table 1.
Baseline characteristics
Biomarker results
R&D systems measured serum samples of sST2 in 35 healthy volunteers with the ELISA we used in our study and received a range of 6.74–20.4 ng/mL.20 For galectin-3, a range of 2.4–15.7 ng/mL was measured in 36 healthy subjects without any medical history available.21
In our investigation, the sST2 values of 28 patients were above 20.4 ng/mL with a maximum value of 60.5 ng/mL. For galectin-3, no patient had a concentration above 15.7 ng/mL.
Regression analysis
A weak positive relationship was detected between sST2 and galectin-3 (r=0.14, P=0.021). Further correlations insisted between sST2 and white cell count (r=0.17, P=0.007), LVEF (r=−0.17, P=0.007) and B-type natriuretic peptide (BNP) (r=0.36, P<0.001) and between galectin-3 and age (r=0.13, P=0.040), white cell count (r=0.16, P=0.012) and creatinine (r=0.20, P=0.001).
The entire linear regression analysis is presented in table 2.
Univariate linear regression analysis between sST2 and galectin-3 and selected covariables
Survival analysis
Univariate, higher levels of sST2 as a continuous variable were a predictor of ACM and CM in the main group. Even after adjustment, sST2 remained significant for ACM.
In the subgroup DCMi⋎viral, higher sST2 values were associated with adverse outcome for both endpoints. In the subgroup idiopathic DCM, sST2 was only associated with the endpoint ACM whereby higher values were associated with worse outcome and in the subgroup fDCM, no significant correlation with the survival rate for any of the endpoints were noticed (table 3A).
Survival analysis of sST2 and galectin-3 as continuous variables for all-cause mortality and cardiac mortality
Survival analysis of the sST2 and the galectin-3 main groups as a quartile model for all-cause mortality and cardiac mortality
In the quartile model, sST2 was only a predictor of the endpoint ACM (table 3B, figure 1A).
Analysis of galectin-3 as a continuous variable neither has shown significant results for the main group nor for any of the subgroups (table 3A). Nevertheless, in the quartile model, galectin-3 was significant for ACM and CM, whereby intermediate values (quartile 3) were associated with better outcome (table 3B). The related Kaplan-Meier curve for the endpoint CM is shown in figure 1B.
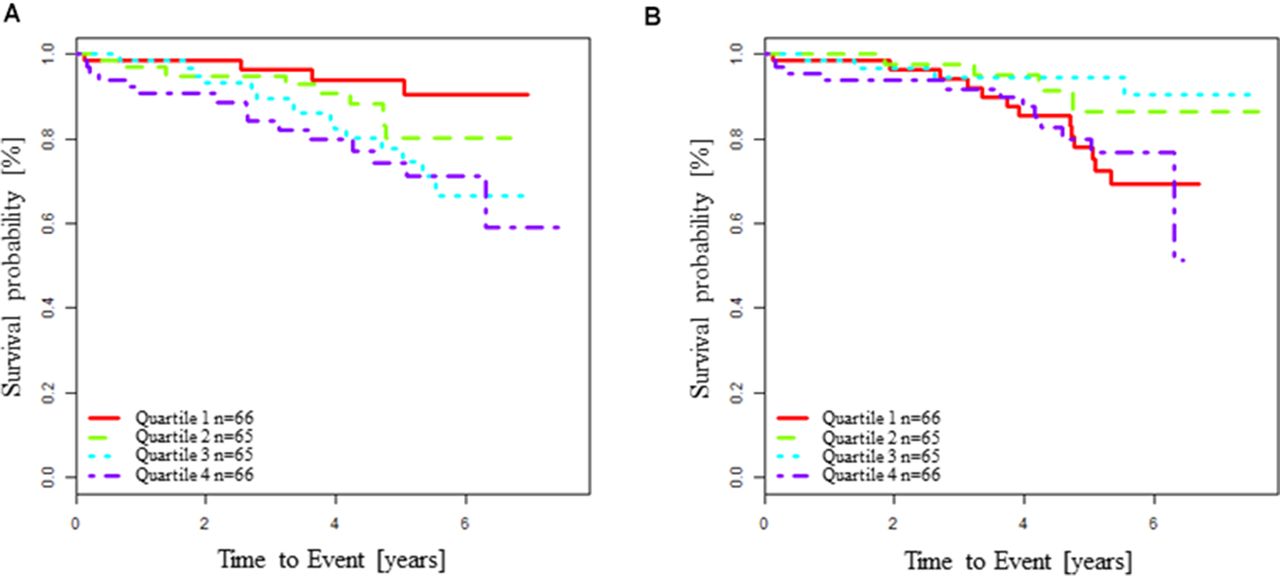
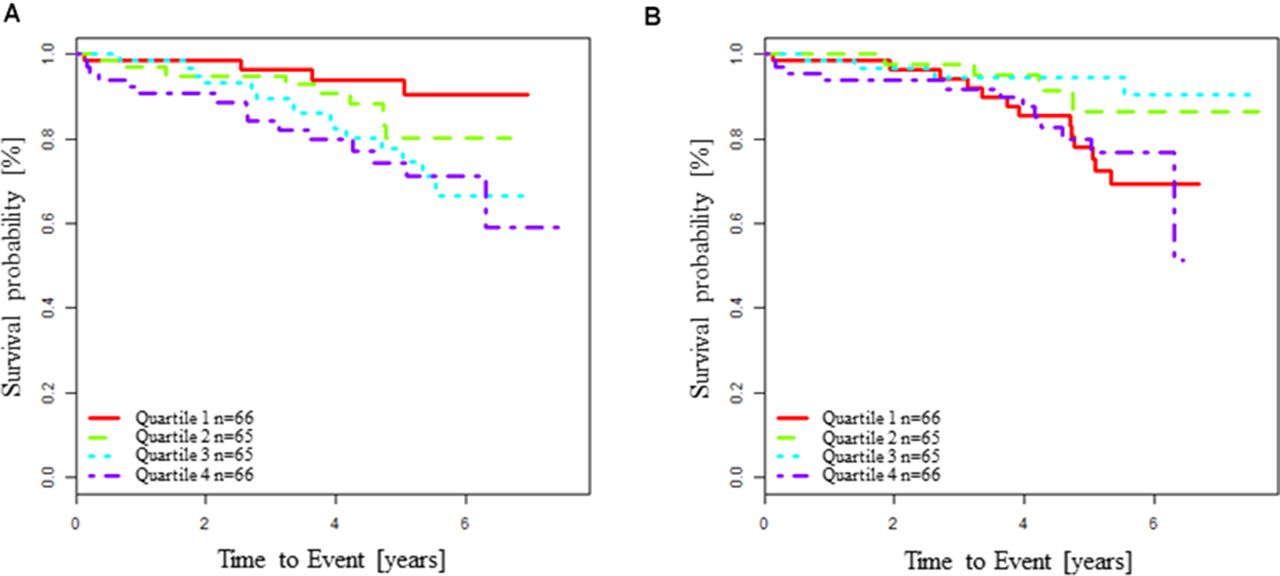{kind=link}
(A) Kaplan-Meier survival analysis for all-cause mortality according to sST2 quartiles. (B) Kaplan-Meier survival analysis for cardiac mortality according to galectin-3 quartiles.
Discussion
The main findings of this study are that sST2 as a continuous variable was a predictor of ACM and CM in patients with non-ischaemic HF. In contrast to the fDCM subgroup and the idiopathic DCM-subgroup with only a significant result for ACM, in the DCMi⋎viral subgroup higher values of sST2 were associated with higher mortality for both endpoints, indicating that sST2 could be useful especially in patients with inflammatory myocardial disease and viral persistence. The results with regard to galectin-3 indicate that intermediate values are associated with a better prognosis.
A prognostic biomarker should be independent of traditional risk factors such as age, body mass index (BMI) or creatinine to ensure similar informative value in patients with different risk profiles. Correlation of the marker with established haemodynamic parameters can be a hint that it has a prognostic value or that combined use could be beneficial. Our strongest, but nevertheless only moderate, positive correlation was between sST2 and BNP. Also we found a negative correlation between sST2 and LVEF. In contrast, no significant correlation was observed between sST2 and age, BMI or creatinine. Galectin-3 did not correlate with the haemodynamic situation reflecting parameters BNP and LVEF. However, it was associated with age and creatinine. Thus, our results of the linear regression analysis suggest that, in this respect, sST2 is superior to galectin-3. Keeping the independence of age, BMI and creatinine in mind, it has a more convenient profile compared with natriuretic peptides.
According to our findings, higher sST2 levels were accompanied by higher risk of ACM and CM in the univariate model and even for the adjusted endpoint ACM significance persisted. Therefore, the results of our study demonstrate prognostic utility of sST2 in patients with DCM as a non-ischaemic cause of HF. Particularly with regard to the pathomechanism of sST2 indicating that ST2 synthesis is upregulated by mechanical strain, the results seem comprehensible.6
Analysis of sST2 in the subgroups revealed no significant results in the subgroup fDCM, although just missing statistical significance for ACM. In the subgroup idiopathic DCM, only the endpoint ACM was significant. However, in the DCMi⋎viral subgroup, sST2 was associated with both endpoints. The HRs in this subgroup were also higher than in the other subgroups and in the analogous univariate model of all 262 patients. Broch et al examined sST2 in 102 patients with DCM. In their study, sST2 levels did not vary with monogenetic aetiology, viral persistence or myocardial inflammation compared with idiopathic aetiology. However, sST2 was associated with haemodynamic parameters. The authors suggested that sST2 in non-ischaemic HF reflects haemodynamic stress rather than pathogenic processes within the myocardium.22 In contrast to that, our findings highlight that sST2 could be useful especially in patients with inflammatory myocardial disease or viral persistence.
In the literature, it was shown that sST2 concentrations were elevated in patients with inflammatory diseases23 with IL-33 reducing inflammatory activity through interaction with the membrane-bound receptor ST2L. This IL-33-mediated effect antagonising soluble ST2 receptor is induced by proinflammatory stimuli, while the expression of ST2L remained constant.24 The pathophysiological role of sSt2 is in accordance with our findings regarding the inflammatory aspects.
So far, the survival analysis of galectin-3 indicate that it is not useful in patients with non-ischaemic HF. However, in the quartile model of galectin-3, we found intermediate values to be associated with a better prognosis. This result may imply that a physiological range could exist for galectin-3, and values above or below this range are associated with worse outcome. No other studies considering galectin-3 in HF reported such a result, rather only higher galectin-3 levels were found to be associated with adverse outcomes.
Recently, Hu et al examined galectin-3 in patients with non-ischaemic cardiomyopathy, among them 85 subjects with DCM and found higher values of galectin-3 significantly associated with adverse cardiac events in univariate analysis.25
However, to the best of our knowledge, we are the first who examined the biomarkers sST2 and galectin-3 with regard to the prognostic information in a cohort of 262 patients with DCM. Thus, no studies with equal conditions exist for comparison.
Nevertheless, our result should be regarded critically. There is no explanation why intermediate values of galectin-3 should be associated with better prognosis than low values. This is in contrast to the assumption that expression of galectin-3 results in fibrosis, because this would imply that particularly higher values were linked to poor prognosis.
Although there are no generally valid standard values so far, it should be noted that we measured not any galectin-3 concentrations above the ‘normal’ range given from R&D Systems in healthy patients. However, this range is based on a very small sample size of only 36 volunteers, and therefore the informative value is limited.
Further studies are needed to assess if sST2 improves discrimination and reclassification analysis in non-ischaemic HF when attached to clinically established biomarkers especially in inflammatory heart disease.
Study limitations
Typical to other heart disease populations, women were under-represented. Over the whole period of observation, we had a dropout rate of 24%. Due to the smaller number of participants in the subgroups with limited event rates, we renounced to do multivariate analyses in those groups.
Acknowledgments
We would like to thank the patients, physicians and nurses involved in this study.
References
Footnotes
Contributors DB performed the ELISA analyses, completed the data and wrote the manuscript. HD performed the statistics. AR and VR included the patients and data, K-DSU and BS wrote the manuscript. SP initiated the investigations, included patients and patients data, wrote and revised the manuscript.
Competing interests None declared.
Patient consent Detail has been removed from this case description/these case descriptions to ensure anonymity. The editors and reviewers have seen the detailed information available and are satisfied that the information backs up the case the authors are making.
Ethics approval Ethics committee of the Medical Faculty of the Philipps-University Marburg.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement There are no additional data available for this paper.
Presented at Parts of the data were presented as poster during the Annual meeting of the European Society of Cardiology in Rome 2016 and published as abstract as follows: Eur Heart J, 2016; 37(Suppl_1): 599–983.